 Orbital Metastatic Cancer
Orbital Metastatic CancerOrbital Metastatic Cancer
General Considerations
Several types of metastatic cancer can reach the orbital soft tissues or bones by hematogenous routes (1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77). Orbital metastasis can occur in adults and children with different primary tumors in each group. This chapter covers only cancers metastatic to the orbit. Lymphomas and secondary cancers that reach the orbit by direct continuity are covered elsewhere.
In adults, most tumors that metastasize to the orbit are carcinomas that arise in breast, prostate gland, lung, kidney, gastrointestinal tract, and other organs. Carcinoid tumors of the small intestine and appendix have a tendency to metastasize to the orbit, whereas bronchial carcinoid tumors tend to metastasize to the uveal tract (38,39,40,41,42). Cutaneous and uveal melanoma and soft tissue sarcomas can occasionally metastasize to the orbit. In children, orbital metastases are uncommon and come mainly from adrenal neuroblastoma and less often from Wilms tumor, and Ewing tumor.
Most patients with breast cancer metastasis to the orbit have a history of breast cancer. Many patients with metastasis from lung cancer or carcinoid tumor have no history of cancer and the orbital mass is often the first sign of malignancy. Overall, about 20% of patients who present with orbital metastasis have no history of a primary cancer and the orbital tumor is the first sign of an undiagnosed primary malignancy (2).
Clinical Features
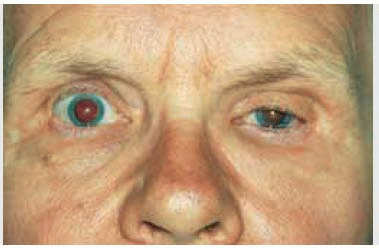
The clinical features of orbital metastasis vary depending on the type of primary neoplasm. Although there are a range of symptoms and signs, the classic presentation is a rather rapid onset of pain, blepharoptosis, proptosis, displacement of the globe, diplopia, and conjunctival and eyelid edema. Some scirrhous tumors, particularly from breast and stomach cancers, can produce a paradoxical enophthalmos because of fibrosis and shrinkage of such tumors (20,23,24).
Diagnostic Approaches
Each patient with suspected orbital metastasis should have a history taken and systemic evaluation to rule out a primary cancer. In cases of orbital metastasis, computed tomography (CT) and magnetic resonance imaging (MRI) findings vary with the primary tumor. Metastatic breast cancer to the orbit tends to be confined to soft tissue, is more diffuse in configuration, and grows along fascial planes and muscle (1,2,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26). Prostate metastasis tends to affect orbital bone (1,2,27,28,29,30). Metastatic melanoma, carcinoid tumor, and renal cell carcinoma may be round to ovoid and circumscribed, resembling a benign orbital tumor (31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50). The diagnosis should generally be confirmed by orbital biopsy. If no primary tumor is known, an orbitotomy with open excisional or incisional biopsy is appropriate. If the patient has a known history of cancer and the orbital lesion is anterior, a fine-needle aspiration biopsy (FNAB) can be done to confirm the diagnosis (1).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


