 Orbital Lipomatous and Myxomatous Tumors
Orbital Lipomatous and Myxomatous TumorsOrbital Fat Prolapse
General Considerations
Weakening of the orbital septum with anterior displacement of orbital fat (“baggy eyelids”) is very common in older individuals. This condition is rarely considered in the differential diagnosis of orbital tumors and is not considered further here. We do discuss, however, a variant that often simulates an orbital or conjunctival neoplasm. This is called orbital fat prolapse.
Orbital fat prolapse is not a true neoplasm, but rather a protrusion of orbital fat through a defect in Tenon’s capsule into the conjunctival fornix (1,2,3,4). It is included here because affected patients are commonly referred with the diagnosis of dermolipoma, lymphoma, or lacrimal gland epithelial tumor. In the authors’ series of 1,264 consecutive space-occupying orbital lesions, the 30 cases of orbital fat prolapse accounted for 47% of lipocytic and myxoid lesions and for 2% of all orbital masses referred to the Oncology Service. However, orbital fat prolapse into the conjunctival fornix is certainly much more common than reflected in that series, which included only more advanced cases that were referred because of suspected tumor. Surprisingly, very little has been published about diagnosis and management of orbital fat prolapse (1,2,3,4).
Clinical Features
Orbital fat prolapse can occur in either gender, but has a predilection for obese elderly men. Clinically, orbital fat prolapse is characterized by a soft yellow mass, almost always in the superotemporal conjunctival fornix and less commonly in the inferotemporal quadrant. Slit-lamp biomicroscopy demonstrates that the lesion is covered by normal conjunctiva and has glistening yellow particles of fat within the mass. Orbital fat prolapse is often confused clinically with dermolipoma, so it is important to emphasize their differences. It occurs in older individuals, is more often bilateral, is more compressible, more elevated, and has visible lipid globules without hair and the anterior border is straight or convex. In contrast, dermolipoma is generally diagnosed in childhood, is more often unilateral, not compressible, sessile in shape, has a gray-pink color, and frequently has fine white hairs on slit-lamp examination; the anterior border is often biconcave, being more parallel to the corneoscleral limbus. Dermolipoma often is associated with Goldenhar syndrome. Conjunctival or orbital lymphoma is also included in the differential diagnosis. If orbital fat prolapse is suspected, it is important to examine the opposite eye because the lesion is often bilateral, although asymmetric.
Diagnostic Approaches
Computed tomography (CT) and magnetic resonance imaging (MRI) show the lesion to be consistent with fat and to be directly continuous with the orbital fat posteriorly. With imaging studies, the prolapsed fat appears hypointense and is continuous with the orbital fat posteriorly.
Pathology
Histopathologically, orbital fat prolapse is composed of normal orbital lipocytes. On occasion, pathologists who are unfamiliar with this entity may make the diagnosis of simple lipoma or pleomorphic lipoma based on the presence of clumps of suspicious cells called florets.
Management
In most instances, orbital fat prolapse can be managed conservatively by periodic observation only. If it attains a large size and produces ocular irritation or is cosmetically unacceptable, then surgical excision is justified. The prolapsed anterior component can be excised by performing a conjunctival incision, exposing most of the fat lobules, clamping the posterior aspect of the lesion with a hemostat, cutting through the clamped fat, and allowing the remainder of the lesion to fall back into the orbit (1,2). Tenon’s fascia and conjunctiva are then closed with running or interrupted absorbable sutures. Recurrence is uncommon if the initial closure is secure.
Selected References
1. Jordan DR, Tse DT. Herniated orbital fat. Can J Ophthalmol 1987;22: 173-177.
2. McNab AA. Subconjunctival fat prolapse. Aust N Z J Ophthalmol. 1999;27: 33-36.
3. Kim YD, Goldberg RA. Orbital fat prolapse and dermolipoma: two distinct entities. Korean J Ophthalmol 1994;8:42-43.
4. Schwarz F, Randall P. Conjunctival incision for herniated orbital fat. Ophthalmic Surg 1980;11:276-279.
Orbital Fat Prolapse
In most instances, orbital fat prolapse is bilateral and fairly symmetric. This bilaterality helps to differentiate it from most neoplasms, which are generally unilateral. Orbitoconjunctival lymphoma can also be bilateral, but it is rarely symmetric and it has a pink, rather than yellow, color.
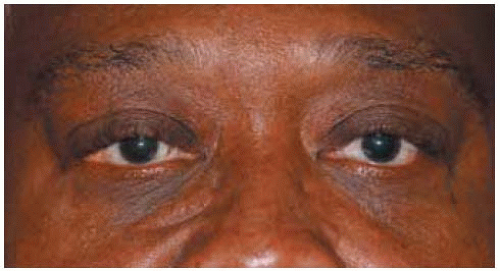 Figure 34.1. Facial appearance of elderly African-Am erican man. A yellow-pink conjunctival lesion can be seen in the lateral canthal region. |
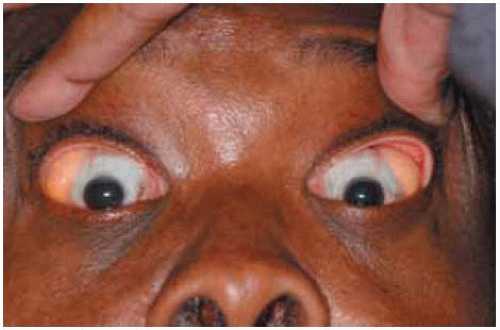 Figure 34.2. Same patient with elevation of both eyelids. The fluctuant, yellow-pink masses can be seen bilaterally. |
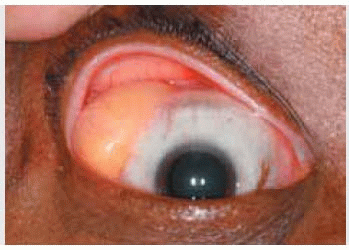
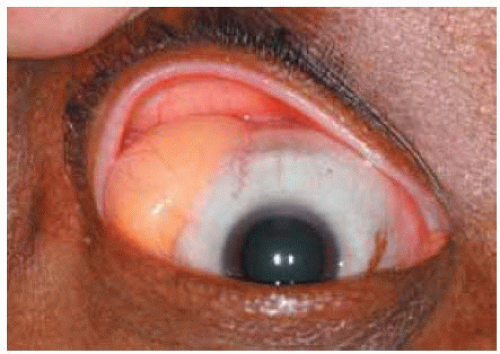 Figure 34.3. Closer view of superotemporal mass in right eye of patient seen in Figure 34.2. The brilliant yellow material within the lesion represents lipid, sometimes forming glistening cholesterol crystals. |
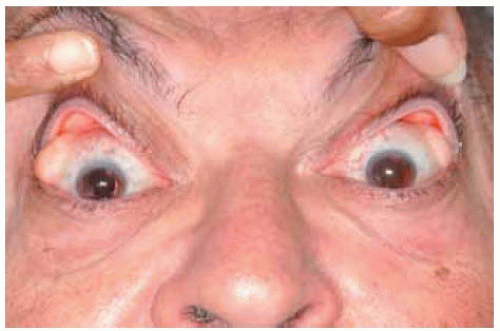 Figure 34.4. Similar bilateral superotemporal masses in an elderly Caucasian man. The upper eyelids are being elevated to afford a better view. |
 Figure 34.5. Closer view of mass on right eye of patient shown in Figure 34.4. |
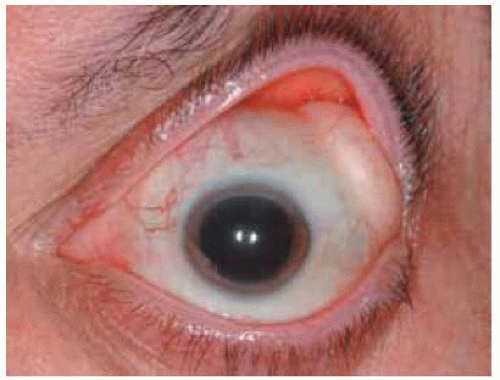 Figure 34.6. Similar but less prominent mass on left side of patient shown in Figure 34.4. |
Orbital Fat Prolapse
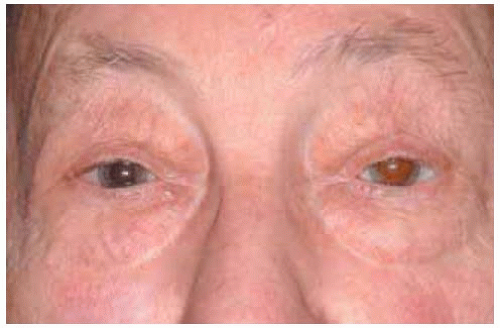 Figure 34.7. Facial appearance of an elderly man with bilateral subcutaneous fluctuant masses owing to herniated orbital fat. |
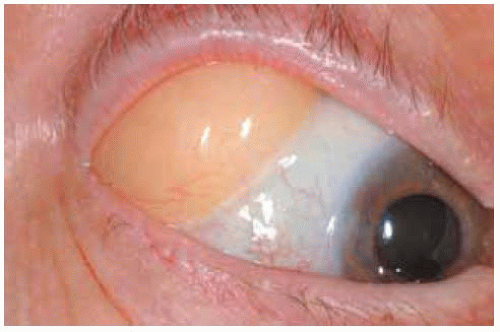 Figure 34.8. Closer view of yellow mass seen in right eye of patient shown in Figure 34.7. |
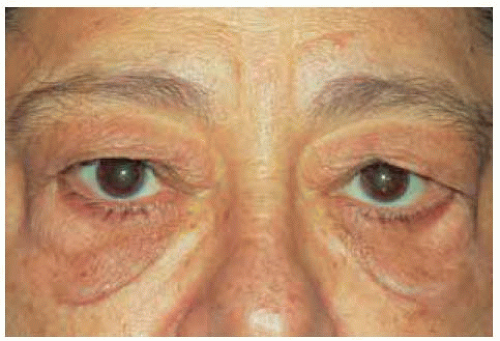 Figure 34.9. Elderly man with bilateral subcutaneous fat similar to patient shown in Figure 34.7. Note the protrusion of the lower eyelids, also owing to fat prolapse. |
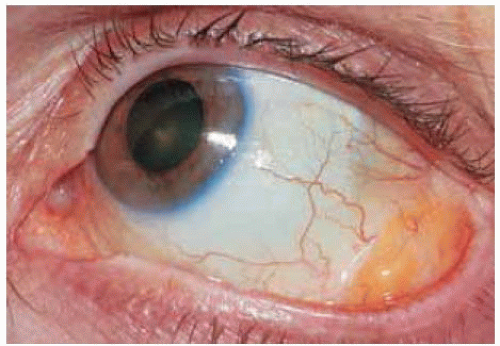 Figure 34.10. Inferotem poral orbital fat prolapse in a 71-year-old woman. Inferotemporal location is less common than superotemporal location. |
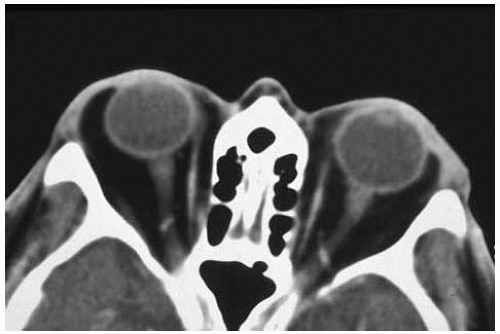 Figure 34.11. Computed tomography of bilateral herniated orbital fat worse in the right eye (on the left in the photograph). Note that the black area represents fat, which extends from the conjunctival fornix into the orbit and is indistinguishable from the orbital fat. |
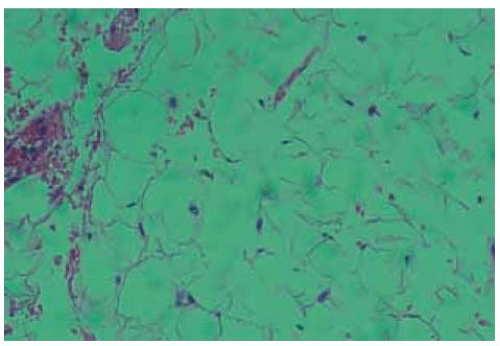 Figure 34.12.Pathology of herniated orbital fat. It is indistinguishable from normal fat. (Hematoxylin-eosin 50.) |
Orbital Fat Prolapse: Clinical and Computed Tomography Features and Surgical Approach
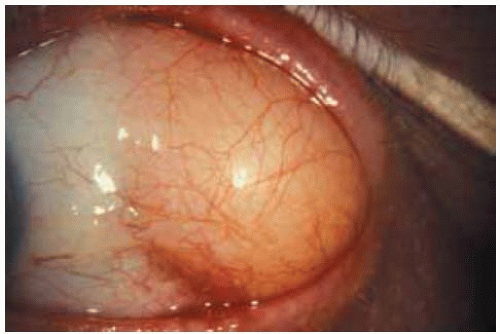 Figure 34.13. Superotem poral herniated orbital fat on left side. This became progressively more prominent and the patient requested surgical excision. |
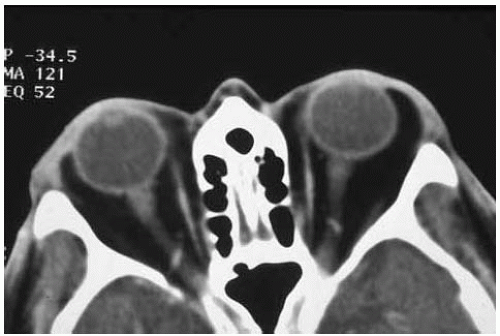 Figure 34.14. Axial computed tomography of lesion shown in Figure 34.13 demonstrating more advanced herniated orbital fat in left orbit. |
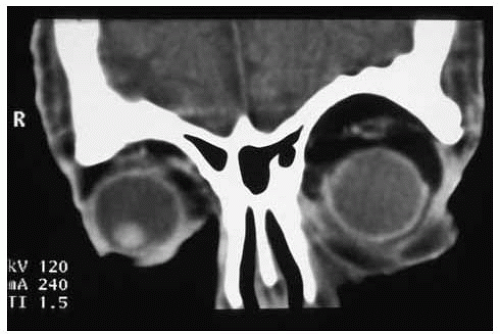 Figure 34.15. Coronal computed tomography through the anterior aspect of the eyes of lesion shown in Figure 34.13. Note the excess orbital fat in left orbit. |
 Figure 34.16. Orbital fat exposed at time of surgery. Scissors are being used to start a conjunctival incision over the mass. |
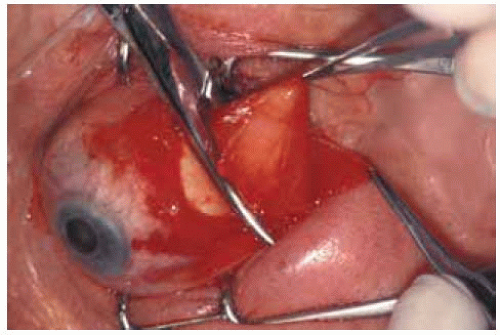 Figure 34.17. The conjunctival incision has been done exposing the fat, which is being lifted with blunt-tipped forceps. A hemostat is being used to clamp the lesion in the anterior aspect of the orbit. Scissors are then used to cut the fat anterior to the hemostat, the hemostat is removed, and the fat allowed to recede into the orbit. |
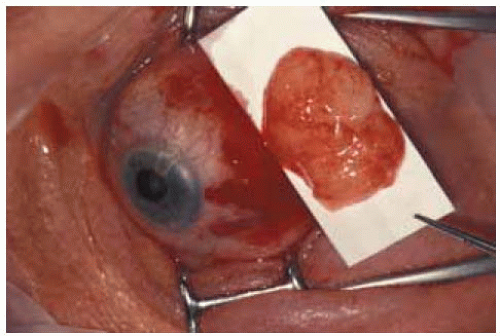 Figure 34.18. The excised tissue is placed on a piece of paper and then sent for histopathologic study. The conjunctival wound is then closed with a running 7-0 absorbable suture. A pressure patch is applied. The residual hemorrhage resolved in a few days. |
Orbital/Conjunctival Dermolip
General Considerations
Dermolipoma (lipodermoid) is a choristoma that often affects the orbit and conjunctiva (1,2,3,4,5,6,7,8,9,10,11,12,13,14). It is also discussed in the section on conjunctival tumors. Dermolipoma is a congenital lesion that is often not detected until adulthood; it may even remain undetected throughout life. In the authors’ series of 1,264 consecutive space occupying orbital lesions, the 31 dermolipomas accounted for 3% of all orbital lesions (7).
Clinical Features
Orbital/conjunctival dermolipoma is a light pink to yellow, firm, sessile to moderately elevated lesion, the anterior portion of which is usually visible in the conjunctival fornix superotemporally. Fine hairs often protrude from the surface of the mass and are best seen with slit-lamp biomicroscopy. Although yellow lipid globules may be seen, the lipid is not so strikingly apparent as in orbital fat herniation. The lesion may extend anteriorly almost to the limbus and some patients complain of a visual field defect owing to the elevated lesion. It is occasionally bilateral, but often asymmetric. It is usually asymptomatic and is either noticed by the patient or by the physician on routine examination. It can cause mild ocular irritation or a foreign body sensation. It is generally stationary and significant enlargement is unusual. There is no predisposition for gender or race. Dermolipoma, like dermoid tumor, can occasionally be associated with certain systemic syndromes, such as Goldenhar syndrome, organoid nevus syndrome, mandibulofacial dysostosis, and others (11,12,13).
Diagnostic Approaches
Orbital dermolipoma is generally apparent on external examination and the diagnosis is easily made. In the case of a larger lesion, orbital computed tomography and magnetic resonance imaging can help to delineate the posterior extent of the lesion. These studies disclose a circumscribed oval or elongated mass extending into the orbit superotemporally in close association with the lacrimal gland and orbital fat. It appears solid, rather than cystic, and has attenuation similar to orbital fat.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


