Orbital Infections
Allan E. Wulc
Brenda C. Edmonson
Orbital and periorbital infections are the most common causes of acute orbital inflammation and are distinguished clinically by anatomic location. Preseptal cellulitis and periorbital cellulitis are synonymous terms that refer to superficial spreading cellulitis without associated spread to the postseptal tissues. Orbital cellulitis, in contrast, is an infection of the postseptal orbital tissues sometimes associated with superficial spreading cellulitis. Both conditions are more commonly seen in children and young adults.1,2,3,4,5,6,7 In Schramm’s series of 303 cases of orbital cellulitis, 68% of patients were younger than 9 years of age, and only 17% were older than 15 years of age.8 Interestingly, there seems to be an unexplained preponderance of left-sided orbital infections as compared with right-sided infections.8,9,10
In the preantibiotic era, Gamble11 reported a mortality rate of 17% in patients with orbital cellulitis. An additional 20% of survivors had loss of vision. Even now, with the ubiquitous use of modern imaging techniques and new antibiotics, the relative ease and rapidity of spread of contiguous infection to the cavernous sinus and the brain renders complications associated with misdiagnosis or inappropriate therapy life threatening. Estimates of the case fatality rate in one series suggest an improvement from 9.4% to 2%, but this mortality rate is unacceptably high, particularly in newborns in which the mortality rate approaches 11%.11
Although these alarming figures are 10-fold less in patients with preseptal cellulitis rather than with orbital cellulitis, preseptal cellulitis can be associated with sepsis and bacterial meningitis and therefore is not necessarily a benign process.12,13
The discussion in this chapter focuses on the differential diagnosis, symptoms and signs, radiologic diagnosis, and microbiology of preseptal and orbital cellulitis. Over the past decade, the management of sinusitis has evolved. New vaccines, better imaging and new antibiotics along with refined methods of surgery all have improved the diagnosis and treatment of sinusitis and as a consequence, the diagnosis and treatment of periorbital and orbital cellulitis. A rational approach to the evaluation and management of these conditions, as well as their sequelae, is provided.
SYSTEMS OF CLASSIFICATION
Preseptal and orbital cellulitis are two distinct conditions that have different anatomic problems at their source but often present with a similar clinical picture.
Preseptal cellulitis usually occurs in either of four clinical settings. These settings include: (a) sinusitis, (b) bacteremia, (c) upper respiratory infection, or (d) local cutaneous infection.14,15,16 In the latter setting, preseptal cellulitis can arise from spread of a contiguous anterior eyelid infection such as a chalazion, local trauma resulting in infection such as an insect bite, or a foreign body.(Fig. 1)
 Fig. 1. Preseptal cellulitis in a 32-year-old woman. Swelling developed over 3 days. Motility was preserved. |
Prior to the Haemophilus influenzae type b (Hib) vaccine, the most common clinical presentation was of a child younger than the age of 36 months with a history of antecedent upper respiratory tract infection, otitis media, and bacteremia and usually resulted from infection with Hib.4 However, since the introduction of the Hib vaccine, the incidence of Hib induced preseptal cellulitis has declined dramatically with some studies reporting up to a 90% reduction.15
Orbital cellulitis, in contrast, usually arises from spread of infection from the paranasal sinuses. Orbital involvement occurs in 0.5% to 3% of patients with acute sinusitis.14 In a large series of patients with orbital cellulitis, sinusitis was responsible for orbital infection in 75% to 90% of cases.8,18,19 The ethmoid sinus is the most commonly implicated sinus in infections that spread to the orbit in children; the frontal and sphenoidal sinuses do not develop until age 7.20 In adults, pansinusitis often is associated with orbital cellulitis and spread is believed to occur through the ethmoid or frontal sinuses.
In addition to anatomic proximity, several other factors predispose the orbit to the spread of contiguous sinus infection. Dehiscences often are present in the orbital walls, particularly in the thin-walled lamina papyracea.21,22,23 As a consequence, pus or transudate may rupture through the thin-walled lamina into the orbit and result in subperiosteal abscess formation. This theoretical mechanism is consistent with the observation that most abscesses occur in the medial orbit, adjacent to the ethmoidal sinuses.24,25,26 Posteriorly, the optic nerve within the optic canal is adjacent to the lateral wall of the sphenoidal sinus. Dehiscences can also be present in the lateral wall of the sphenoidal sinus along the optic canal, in approximately 6% of cases.27
Another factor predisposing the orbit to the spread of adjacent sinus infection is the free vascular communication between the orbit and the sinuses. The orbital veins are valveless, and flow occurs in either direction28 through the anterior and posterior ethmoidal foramina. Increased pressure within the sinuses caused by obstruction to mucus outflow in sinusitis may hamper venous drainage and manifest as the eyelid edema that accompanies acute sinus inflammation. Septic thrombophlebitis can also occur within these vessels and allow bacterial spread into the orbit.29,30,31,32,33
However, all orbital cellulitis resulting from sinus disease is not secondary to acute sinusitis. Orbital fracture can spread existing chronic sinus infection into the orbit (Fig. 2).25,31,32,33 Mucoceles, slowly enlarging mucus-filled cysts within the sinuses that enlarge by pressure erosion of adjacent orbital and intracranial structures, can become infected and result in mucopyoceles that cause both cellulitis and abscess formation.34,35,36,37
 Fig. 2. Orbital cellulitis following repair of an orbital floor fracture in a 14-year-old patient with a history of stuffy nose. There was progressive onset of diplopia, pain, and extraocular movement limitation 2 days after surgery to the left orbit. A. Primary position. B. Downgaze. |
Approximately 15% of orbital cellulitis occurs from other sources.8 In particular, dacryocystitis is sometimes associated with a cellulitis that may spread posteriorly into the orbit (Figs. 3 and 4). 8 Infection can spread to the orbit from the eye, the teeth, the middle ear, or the face. Foreign bodies, such as wood, glass, or orbital floor implants, can cause orbital cellulitis refractory to treatment with antibiotics that requires removal of the nidus of infection (Fig. 5). Alternatively, a granulomatous reaction may develop around the foreign body or a cutaneous fistula may occur.25 Orbital infection has been described after uncomplicated eyelid, strabismus, and retinal surgery.38,39,40 Rarely, dental work or an infected dental cyst may cause orbital cellulitis through spread of infectious phlebitis across the pterygopalatine venous plexus.41,42 Endophthalmitis from a variety of endogenous or exogenous causes may extend extraocularly to involve the orbit. Finally, orbital cellulitis can occur secondarily from embolic spread in subacute bacterial endocarditis.2,3,12
 Fig. 3. Neonatal dacryocystitis. Untreated lacrimal sac infection may result in orbital cellulitis. In addition to antibiotics, probing and irrigation are required. |
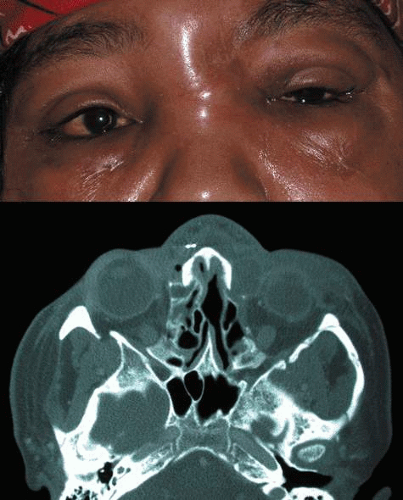 Fig. 4. A. Orbital cellulitis from a dacryocystitis. The dacryocystitis developed in this 43-year-old woman who sustained multiple orbital fractures after facial trauma. B. The axial computed tomogram shows dacryocystitis and orbital inflammation. The patient was treated with intravenous antibiotics and a dacryocystorhinostomy. |
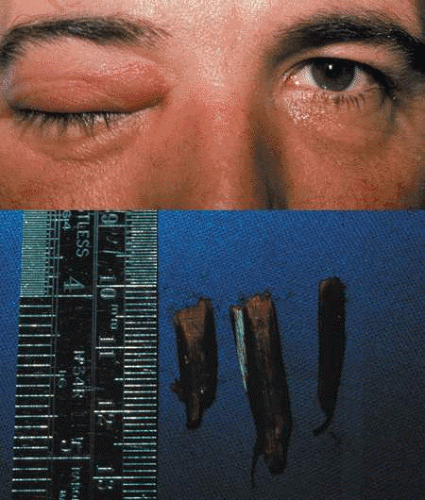 Fig. 5. A. Orbital cellulitis from a foreign body in a 45-year-old patient who 4 days earlier fell off a ladder and sustained a right nasal laceration. The cellulitis was treated with intravenous antibiotics with no improvement. All imaging scans were negative. B. At surgery, these wooden foreign bodies were removed from the right orbit. |
Regardless of its anatomic site of origin, edema develops as the orbital infection spreads within the connective tissues. Septic thrombophlebitis may ensue and increase both edema and orbital pressure as blood flow is impeded. Congestive signs such as chemosis, intraocular pressure, and proptosis increase. The infection may consolidate to form an abscess. The infection, in turn, may spread through the vascular emissaries into the cavernous sinus or intracranially, causing cavernous sinus thrombosis, meningitis, carotid occlusion, and subdural, epidural, or brain abscess.
A spectrum of progressive infectious changes in orbital cellulitis initially was described by Hubert30 and modified by Smith and Spencer43 and later by Chandler,29 and is useful to the understanding of the nature of the evolution of orbital cellulitis, in classifying the severity of infection and defining progression and management.
Stage 1 inflammation represents preseptal cellulitis. All changes that are seen on examination are confined to the anterior eyelid tissues. Occasionally, edema may spread secondarily posterior to the septum but does not represent the spread of cellulitis posteriorly. Chemosis may be present, and it may even cause minimal limitation of ocular movement.
Stage 2 inflammation represents orbital cellulitis, with leukocytosis, and often fever, proptosis, extraocular movement limitation, and the congestive signs discussed earlier (Fig. 6).
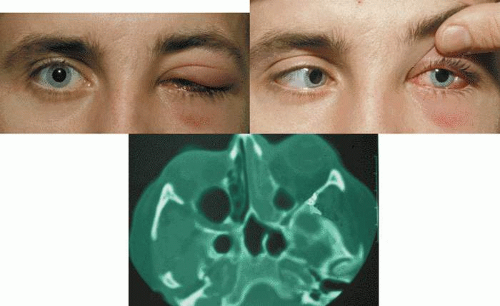 Fig. 6. A. Orbital cellulitis presenting in a 27-year-old man with normal visual acuity. B. Chemosis and limitation of abduction. C. Computed tomography shows ethmoid sinusitis on the left side. |
With stage 3 inflammation, subperiosteal orbital abscess formation occurs. The globe is often displaced and limited in the field of gaze of the abscess, which occurs concomitant with the signs of orbital cellulitis seen in stage 2.
In stage 4 inflammation, a true orbital abscess develops. These patients have severe proptosis, chemosis, ophthalmoplegia, and, often, visual loss.
Stage 5 inflammation represents retro-orbital spread of infection into the cavernous sinus. In these instances, orbital signs may occur in the fellow eye and other central nervous system signs supervene.29
SYMPTOMS AND SIGNS
PRESEPTAL CELLULITIS
Patients with preseptal cellulitis often present with a short history of painless swelling of the eyelids. A history of previous upper respiratory tract infection, trauma, insect or animal bite, conjunctivitis, or chalazion may be elicited.
Fever is an inconstant feature but may be present in approximately 62% of cases.12 The eyelid characteristically is erythematous and edematous and may show signs of the trauma, bite, or chalazion that initiated the cellulitis (see Fig. 1). The eyelid may be painful to palpation. The superficial spreading cellulitis is confined to the eyelid and delimited by the attachments of the orbital septum to the arcus marginalis of the orbital rim so that infection will extend to this area and not beyond.
Rarely, the etiology of the eyelid infection may be diagnosed clinically. Necrotizing eyelid cellulitis may be caused by erysipelas, an infection with a group A β-hemolytic Streptococcus, and can give rise to lid necrosis (Fig. 7).44,45 H. influenzae produces a characteristic nonsuppurative preseptal cellulitis with a purplish discoloration of the eyelids.46 Staphylococcal species may cause a suppurative cellulitis with abscess formation.
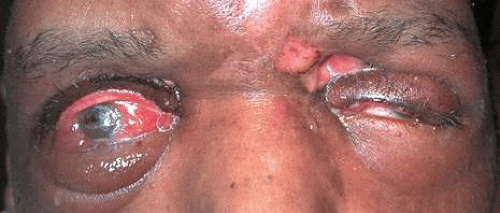 Fig. 7. A. Orbital cellulitis in 58-year-old patient secondary to Group B Streptococcus with no previous history of eyelid trauma. Exfoliation, crusting, and necrosis of skin can be seen. |
Chemosis and extraocular motility deficits are seen only occasionally and are presumed to result from anterior edema rather than spread of infection. Vision and pupillary examination are always unaffected by preseptal cellulitis, and proptosis and globe displacement never are present. Therefore, in the examination of patients with presumed preseptal cellulitis, vision, proptosis, and extraocular movements are key distinguishing points.
ORBITAL CELLULITIS
Orbital cellulitis presents as pain, proptosis, globe displacement, double vision, and/or vision loss (Figs. 6 and 8). Patients often have accompanying headache and malaise. In children fever occurs with equal incidence as in preseptal cellulitis (62%),12 whereas in adults it may be absent 66% of the time.47
 Fig. 8. A. Orbital cellulitis presenting in a 7-year-old girl. B. Computed tomography shows bilateral ethmoid and maxillary sinusitis. |
Antecedent and significant past medical history may include a history of headache, rhinitis, sinusitis, polyposis, nasal discharge, anosmia, or recent upper respiratory tract infection. The patient may give a history of prior orbital fracture or orbital fracture surgery with implantation of alloplastic materials. Scleral buckling procedures and strabismus surgery have been noted to cause orbital cellulitis; thus, the patient should be queried regarding prior ophthalmic surgery.38,39,40 The patient may also give a history of recent dental work, specifically dental extractions.42 The patient may have had prior surgery of the eyelids or of the facial skeleton with insertion of wires, rigid internal fixation (miniplates), alloplastic plates, or nondissolving suture material.34
Pain is not invariably present. It is notably absent in approximately 40% of cases, even those presenting with abscess.25
Fever is a nonspecific sign. In the presence of purulent sinusitis, pain may be present when the affected sinus is palpated; and with ethmoid sinusitis, pain may be elicited with pressure on the inner canthus. The sinus may not transilluminate. Mucopurulent rhinorrhea may be present, and the ophthalmologist when possible should look in the nose or seek the opinion of an otorhinolaryngologist.
Proptosis, chemosis, and extraocular motility deficit are the clinical hallmarks of orbital cellulitis (see Fig. 6). Visual acuity decrease, pupillary signs, and vision loss may occur rapidly. Rarely, if sphenoid sinusitis occurs in isolation, the patient may present with atypical optic neuritis without proptosis or with little in the way of superficial cellulitis.48 Optic neuropathy, with the associated pupillary finding of a relative afferent pupillary defect and optic nerve head findings such as optic disc edema, may be observed. As orbital pressure increases, patients can show signs of retinal and choroidal arterial and venous stasis with congestion and a picture resembling chronic vein occlusion or central retinal artery occlusion. Hypesthesia of the nasociliary or frontal nerves is rarely seen. Hypotony, choroidal folds, and anterior segment inflammation with hypopyon can occur and imply intraocular spread. A dilated nonreactive pupil implies third nerve involvement. Patients may show signs of third, fourth, or sixth nerve involvement when the infection extends into the orbital apex.
Subperiosteal abscess formation most often is diagnosed on neuroimaging and is indistinguishable clinically from orbital cellulitis. Signs of an abscess include displacement of the globe away from the affected sinus and limitation of abduction and adduction,24 but these signs can occur with orbital cellulitis as well. Intraorbital abscess formation can present in the patient who has been partially treated for an orbital infection and may present as proptosis or globe displacement without any infectious signs or as orbital cellulitis.25
If infection spreads posteriorly through the superior orbital fissure to involve the cavernous sinus, additional signs may supervene. Signs of cavernous sinus thrombosis include headache, ipsilateral hypesthesia from involvement of the ophthalmic and maxillary division of the trigeminal nerve; third, fourth, and sixth cranial nerve palsies; and mental status changes from confusion to obtundation. The contralateral side may develop cranial nerve signs, periorbital edema, or cellulitis (Fig. 9).
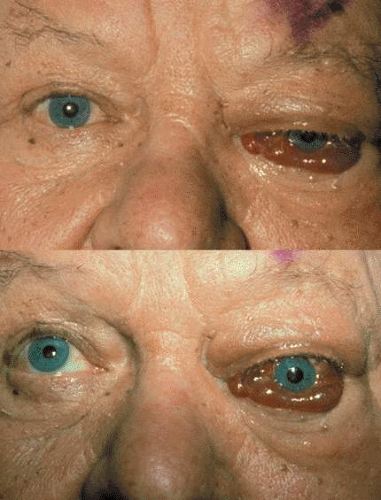 Fig. 9. Cavernous sinus thrombosis in a 74-year-old patient with 2-day history of right orbital cellulitis with rapidly developed obtundation and left-sided orbital changes. A. Primary position. B. Upgaze. |
DIFFERENTIAL DIAGNOSIS
Several conditions can mimic orbital and periorbital cellulitis. Most of these present as the same constellation of symptoms and signs and often can have a similar appearance on neuroimaging.
PRESEPTAL CELLULITIS
Conditions that may masquerade as preseptal cellulitis include allergic edema of the eyelids, severe blepharoconjunctivitis, dacryoadenitis (Fig. 10), trauma, thyroid eye disease (Fig. 11), leukemic infiltrates,49 blepharochalasis syndrome, and autoimmune inflammatory disorders such as lupus.
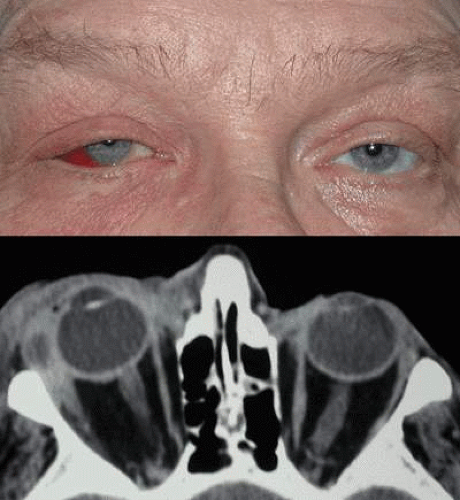 Fig. 10. A. Bacterial dacryoadenitis. B. Computed tomography shows a mass in the left lacrimal gland. |
 Fig. 11. A. Inflammatory thyroid eye disease; note bilateral eyelid retraction and proptosis. B. Malar festoons and right eyelid retraction. |
ORBITAL CELLULITIS
Conditions that may mimic orbital cellulitis include thyroid eye disease, idiopathic inflammatory orbital pseudotumor (Fig. 12), orbital myositis,50 orbital abscess,51 ruptured dermoid cyst, necrotic intraocular melanoma or retinoblastoma,52,53 orbital trauma, orbital foreign body, orbital vasculitis, Wegener’s granulomatosis, herpes simplex or zoster (Fig. 13), and carotid cavernous fistula. Acute-onset proptosis with inflammatory signs in a child always should alert the clinician to the possibility of rhabdomyosarcoma (Fig. 14).
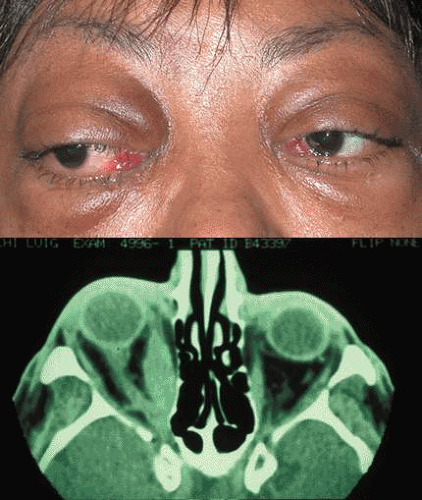 Fig. 12. A. Idiopathic inflammatory orbital pseudotumor. Note chemosis and limitation of abduction. There was no evidence of anterior cellulitis. B. Computed tomography demonstrates enlargement of right medial rectus muscle. |
 Fig. 13. A. Herpes zoster affecting the V1 nerve and causing upper eyelid edema and erythema. |
 Fig. 14. Acute-onset proptosis in 12-year-old child caused by pseudocellulitis resulting from rhabdomyosarcoma. |
LABORATORY AND IMAGING STUDIES
As a routine, white blood cell counts and at least two sets of blood cultures are obtained in all patients who present with orbital infections. However, since the decline in Hib as an etiologic agent, blood cultures in patients with preseptal cellulitis are less likely to yield positive results.14,15 Cultures of the nasopharynx and conjunctiva may be obtained, although this may not yield significant information unless a predominant organism is present. Cultures of the leading edge of the cellulitis are performed if there is an obvious sign of an entry wound responsible for the cellulitis. Cultures of purulent discharge may also be helpful. Cerebrospinal fluid is obtained for culture if the patient shows central nervous system signs or bilateral disease. Neuroimaging via computed tomography (CT) usually is obtained in patients with orbital cellulitis in Chandler stages 3 through 5.16,54,55 However, CT may be obtained in Chandler stages 1 and 2 based on the clinical situation, and index of suspicion of posterior infection, sinus disease, or abscess formation. Repeat CT is also indicated if there is no improvement after 48 hours of appropriate antibiotic treatment or if there is worsening of the clinical signs and symptoms.16,54,55
The white blood cell count may be elevated with leukocytosis in both orbital and preseptal cellulitis. In one study, elevated absolute white blood cell counts were seen in children with periorbital cellulitis and bacteremia but not as frequently as in orbital cellulitis.12 The erythrocyte sedimentation rate may be elevated. If the infection is from α-hemolytic Streptococcus, the antistreptolysin O titer may be elevated.
If meningitis is present, the cerebrospinal fluid may demonstrate pleocytosis, increased protein, and decreased sugar.
ULTRASOUND
Ultrasound has higher resolution (0.1 mm) when compared with CT (0.8 mm) but adds little clinically significant information because ultrasound misses the posterior third of the orbit and does not image the bone and sinuses.56 Ultrasound in orbital cellulitis, however, may be useful in ruling out orbital myositis, determining the location of orbital foreign bodies or abscesses, and following patients with drained orbital abscesses to rule out reaccumulation.
Ultrasound findings in subperiosteal abscess can include a signal of low or medium reflectivity adjacent to the involved orbital wall. If the abscess is intraconal, a low reflective signal is encountered within the cone, the muscles may be thinned as they are placed on stretch, the sclera may be thickened, or a T sign (usually associated with orbital pseudotumor) may be seen. Ultrasound is not helpful in distinguishing inflammatory transudate from infectious exudate or hemorrhage.
NEURORADIOGRAPHIC STUDIES
Routine skull films and polytomography have been supplanted by CT in the evaluation of patients with orbital cellulitis.57 CT allows the clinician to differentiate a preseptal cellulitis from an orbital cellulitis.58 If orbital cellulitis has resulted from adjacent intercurrent sinus infection, the diagnosis can be made and the extent of the sinus disease estimated. Sinuses may show changes of osteomyelitis with blurring of the osseous margins of the sinuses, air–fluid levels, or inflammatory tissue within the normally aerated sinus.59 Central nervous system complications can be assessed by neuroimaging, and progression of disease can also be monitored.58
CT should be performed using thin-section (2–4 mm) high-resolution scanning with multiple views of both bone and soft tissue detail.53 Axial and coronal views should be obtained; in one-third of patients with subperiosteal abscesses, the abscess was seen in the coronal sections only.18 Helical CT is a fairly new technology that allows increased resolution with decreased imaging time.60 This type of scan may be especially beneficial in children because of the ability to obtain good imaging with a shorter imaging time.60 elica He HhIntravenous contrast material is not advocated at all centers because there is intrinsically high contrast between infectious changes and orbital fat. However, some authors believe that it is essential to the diagnosis, and it thus remains the preference of the individual clinician, as well as the neuroradiologist.22,59,62
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


