 Orbital Histiocytic Tumors and Pseudotumors
Orbital Histiocytic Tumors and PseudotumorsOrbital Juvenile Xanthogranuloma
General Considerations
Proliferative disorders of histiocytes comprise a spectrum, ranging from solitary benign inflammatory processes to widely disseminated lesions that exhibit malignant behavior (1,2,3,4,5,6,7,8,9,10). Conditions to be considered here include juvenile xanthogranuloma (JXG), Langerhans’ cell histiocytosis (LCH), Erdheim-Chester disease (ECD), sinus histiocytosis with massive lymphadenopathy (SHML), and multinucleate cell angiohistiocytoma. Necrobiotic xanthogranuloma (NXG), a related condition, is discussed in the section on eyelid tumors.
Clinical Features
The general clinical features and other ocular findings in JXG are discussed in the sections on eyelid, conjunctival, and intraocular tumors. Orbital involvement with JXG seems to be more common in the anterior extraconal spaces and presents as eyelid swelling and a palpable mass. Most JXG in the orbit has been solitary, without a history of cutaneous lesions. Orbital JXG has usually been diagnosed in the first year of life in contrast to lesions in the conjunctiva and eyelid, which can appear in older children or adults (9). Inflammatory signs are usually minimal. Orbital JXG can occasionally be more aggressive and invade orbital bone and the intracranial cavity (7,8,10).
Diagnostic Approaches
Imaging studies show an irregular, solid mass that is usually located in the anterior orbital structures. It shows mild to moderate enhancement with contrast agents. The diagnosis is not often made clinically, but is recognized histopathologically after incisional or excisional biopsy.
Pathology
JXG is characterized histopathologically by a proliferation of histiocytes, along with lymphocytes, plasma cells, eosinophils, and typical Touton giant cells that stain positive for lipid. Immunohistochemical markers for histiocytes are positive and S-100 protein is negative. Electron microscopy does not generally show cytoplasmic Birbeck granules, structures that characterize LCH.
Management
If it were possible to diagnosis orbital JXG clinically, a period of observation or oral or perilesional corticosteroids would seem to be appropriate management. However, the diagnosis is rarely made clinically and most cases are removed surgically because of suspicion of neoplasm. If possible, the mass should be removed entirely. If that is not possible and partial biopsy establishes the diagnosis, then corticosteroids are the preferred treatment. More advanced cases with bone involvement may require wide surgical excision and supplemental corticosteroids. Irradiation is generally not warranted.
Selected References
1. Shields JA. Histiocytic tumors and pseudotumors. Juvenile xanthogranuloma. In: Shields JA, ed. Diagnosis and Management of Orbital Tumors. Philadelphia: WB Saunders; 1989:384-385.
2. Henderson JW. Juvenile (infantile) xanthogranuloma. In: Henderson JW, ed. Orbital Tumors. 3rd ed. New York: Raven; 1994:315-316.
3. Jakobiec FA, Bilyk JR, Font RL. Juvenile xanthogranuloma. In: Spencer WH, ed. Ophthalmic Pathology. An Atlas and Textbook. 4th ed. Philadelphia: WB Saunders; 1996:2754-2758.
4. Shields JA, Shields CL. Clinical spectrum of histiocytic tumors of the orbit. Trans Pa Acad Ophthalmol Otolaryngol 1990;42:931-937.
5. Shields CL, Shields JA, Buchanon H. Solitary orbital involvement with juvenile xanthogranuloma. Arch Ophthalmol 1990;108:1587-1589.
6. Hidayat AA, Mafee MF, Laver NV, et al. Langerhans’ cell histiocytosis and juvenile xanthogranuloma of the orbit. Clinicopathologic, CT, and MR imaging features. Radiol Clin North Am 1998;36:1229-1240.
7. Sanders TE. Infantile xanthogranuloma of the orbit. A report of three cases. Am J Ophthalmol 1966;61:1299-1306.
8. Gaynes PM, Cohen GS. Juvenile xanthogranuloma of the orbit. Am J Ophthalmol 1967;63:755-757.
9. Mencia-Gutierrez E, Gutierrez-Diaz E, Madero-Garcia S. Juvenile xanthogranuloma of the orbit in an adult. Ophthalmologica 2000;214:437-440.
10. Miszkiel KA, Sohaib SA, Rose GE, et al. Radiological and clinicopathological features of orbital xanthogranuloma. Br J Ophthalmol 2000;84:251-258.
Orbital Juvenile Xanthogranuloma
Juvenile xanthogranuloma can occur as a solitary orbital mass in infants. A clinicopathologic correlation is illustrated.
Shields CL, Shields JA, Buchanon H. Solitary orbital involvement with juvenile xanthogranuloma. Arch Ophthalmol 1990; 108:1587-1589.
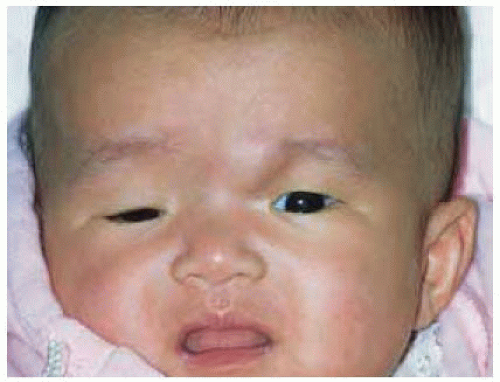 Figure 35.1.Subcutaneous mass superonasal to left eye secondary to juvenile xanthogranuloma in a 3-month-old girl. The mass was noted at birth and had shown gradual enlargement. |
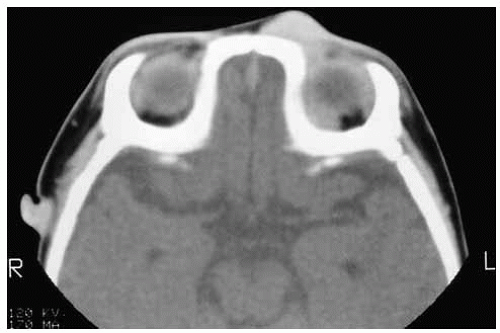 Figure 35.2.Axial computed tomography showing solid mass extending posteriorly along the superonasal wall of the orbit. |
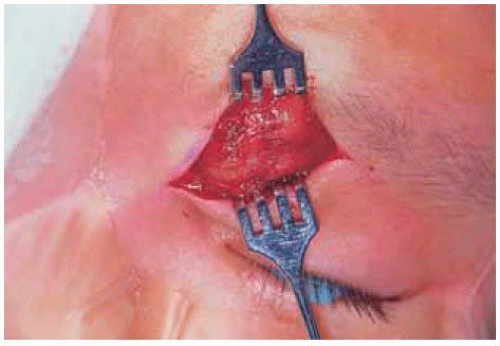 Figure 35.3. A biopsy of the subcutaneous portion of the mass was taken through a superonasal skin incision. |
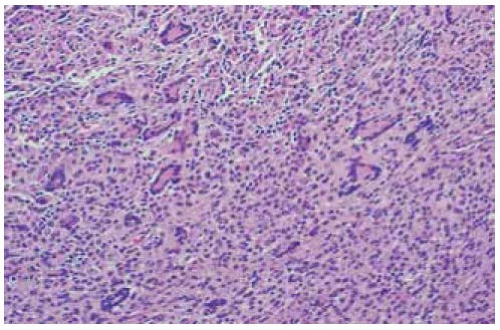 Figure 35.4. Histopathology showing sheets of histiocytes, chronic inflammatory cells, and giant cells. (Hematoxylin-eosin 50.) |
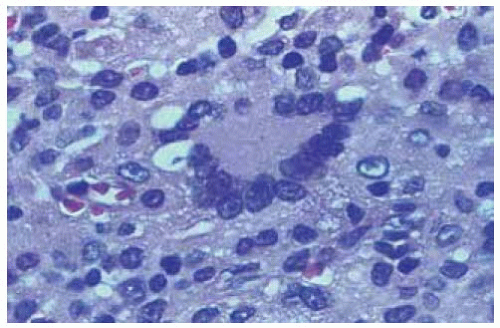 Figure 35.5. Histopathology showing giant cell with some lipid. It was classified as an atypical Touton giant cell. (Hematoxylin-eosin 250.) |
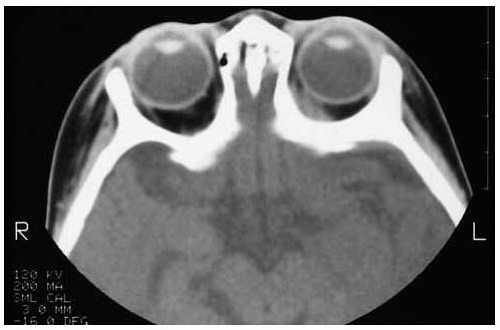 Figure 35.6. Axial computed tomography showing resolution of orbital mass after a course of systemic corticosteroids. |
Orbital Langerhans’ Cell Histiocytosis (Eosinophilic Granuloma)
General Considerations
Langerhans’ cell histiocytosis is the currently accepted name for a group of diseases previously included under the term “histiocytosis X,” namely eosinophilic granuloma (EG), Hand-Schuller-Christian disease, and Letterer-Siwe disease. The ultrastructural finding of typical rod-shaped or tennis recquet-shaped structures, called Birbeck bodies, suggest that the Langerhans’ cell is involved in the disease process (1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25). The Langerhans’ cell is a specific variant of dendritic histiocyte that ordinarily resides in the epidermis. The clinical manifestations of LCH vary widely, from a benign, self-limited process to an aggressive systemic condition that can cause death. Some of the more malignant histiocytoses have been reclassified as true histiocytic lymphomas (2). The most important of these with regard to the orbit is EG, which can occur in the orbital region in children as a solitary lesion of bone. Orbital EG is more common than orbital juvenile xanthogranuloma. The 9 EGs accounted for 53% of all histiocytic lesions and for 1% of all orbital lesions in the authors’ series of 1,264 orbital lesions (4).
Clinical Features
EG usually has typical clinical features, although the clinical findings can vary somewhat from case to case. It generally occurs in the first decade of life as a subacute swelling in the superotemporal aspect of the orbit, often with pain, redness, and tenderness over the affected bone superotemporally (1,2,3). It can resemble a ruptured dermoid cyst, dacryoadenitis, or idiopathic orbital inflammation (“inflammatory pseudotumor”). EG can occasionally develop in other quadrants and in the deeper orbital tissues, and can sometimes be multifocal. It can rarely be bilateral, with the opposite orbit becoming involved months after the first tumor. The lesion tends to gradually heal spontaneously. We have observed EG to recur later in the opposite orbit (25).
Diagnostic Approaches
Computed tomography (CT) and magnetic resonance imaging (MRI) have rather typical features in cases of EG. In the early stages, the lesion appears as an irregular, enhancing, radiolucent area of expanding bone, often with distinct fragments of bone within the mass. It usually affects the zygomatic and/or frontal bones, but other orbital bones can be affected. With time, the intraosseous lesion breaks through the cortical bone producing a moth-eaten appearance. The soft tissue component usually shows some enhancement with CT and MRI (2). Radiographically, it can resemble metastatic neuroblastoma, which occurs in somewhat younger children. Some degree of intracranial extension is not rare. Multiple osseous lesions are occasionally seen in other orbital and cranial bones (16). Although we generally prefer an open biopsy, fine-needle aspiration biopsy has been used to make the diagnosis in some cases (14).
Pathology
EG is characterized histopathologically as a proliferation of large mononuclear histiocytes with multinucleated giant cells of the Touton type, and scattered eosinophils, lymphocytes, and sometimes bone fragments. Positive immunohistochemistry reaction to S-100 protein is helpful in making the diagnosis. The diagnostic ultrastructural features finding are the Birbeck granules, distinctive rod-shaped or tennis racquet-shaped structures that are characteristic of Langerhans’ cells.
Concerning pathogenesis, it is believed that transient immune dysfunction may provoke the cytokine-mediated proliferation of pathologic Langerhans’ cells within the bone marrow of the anterolateral frontal bone. These cells cause osteolysis through elaboration of interleukin-1 and prostaglandin E2 (10,11).
Management
Management includes biopsy with possible frozen sections to make a provisional diagnosis, followed by prompt surgical curettage. Systemic or local corticosteroids can be employed (4). Cytotoxic agents or low-dose radiotherapy are rarely used today except for massive destructive lesions. The lesion also has a tendency to heal spontaneously without treatment (5).
Selected References
1. Shields JA. Histiocytic tumors and pseudotumors. Juvenile xanthogranuloma. In: Shields JA, ed. Diagnosis and Management of Orbital Tumors. Philadelphia: WB Saunders; 1989:384-385.
2. Henderson JW. Juvenile (infantile) xanthogranuloma. In: Henderson JW, ed. Orbital Tumors. 3rd ed. New York: Raven; 1994:315-316.
3. Shields JA, Bakewell B, Augsburger DG, et al. Space-occupying orbital masses in children. A review of 250 consecutive biopsies. Ophthalmology 1986;93:379-384.
4. Shields JA, Shields CL, Scartozzi R. Survey of 1264 patients with orbital tumors and simulating lesions: the 2002 Montgomery Lecture, part 1. Ophthalmology 2004;111:997-1008.
5. Shields JA, Shields CL. Clinical spectrum of histiocytic tumors of the orbit. Trans Pa Acad Ophthalmol Otolaryngol 1990;42:931-937.
6. Feldman RB, Moore DM, Hood CI, et al. Solitary eosinophilic granuloma of the lateral orbital wall. Am J Ophthalmol 1985;100:318-323.
7. Jordan DR, McDonald H, Noel L, et al. Eosinophilic granuloma. Arch Ophthalmol 1993;111:134-135.
8. Wirtschafter JD, Nesbit M, Anderson P, et al. Intralesional methylprednisolone for Langerhan’s cell histiocytosis of the orbit and cranium. J Pediatr Ophthalmol Strabismus 1987;14:195-197.
9. Glover AT, Grove AS. Eosinophilic granuloma of the orbit with spontaneous healing. Ophthalmology 1987;94:1008-1012.
10. Harris GJ, Woo KI. Eosinophilic granuloma of the orbit: a paradox of aggressive destruction responsive to minimal intervention. Trans Am Ophthalmol Soc 2003;101:93-103.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


