CHAPTER 92 Oral Manifestations of Systemic Diseases
The oral cavity has been frequently referred to as a window into a person’s body. Several systemic diseases manifest initially through oral manifestations, which can be readily examined via noninvasive techniques. Saliva and crevicular fluid (exudate from the periodontal ligament) may replace certain serologic tests in the future, and buccal epithelial cells may provide diagnoses for systemic diseases. Recognition of normal and unusual oral conditions will help improve the prevention, diagnosis, dissemination, and management of many systemic diseases. Systemic conditions may require modifications of oral treatments (Table 92-1), and drugs can affect oral health (Table 92-2). This clearly requires a multidisciplinary approach to health care involving numerous specialties from medicine and dentistry.
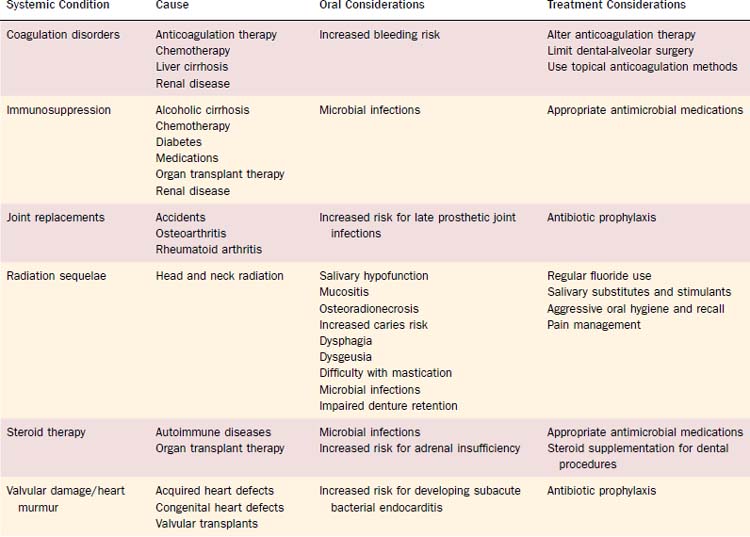
Table 92-2 Overview of Oral Sequelae of Medication Intake for Systemic Diseases
| Drug Category | Drug | Oral Problem |
|---|---|---|
| Analgesics | Aspirin | Hemorrhage, erythema multiforme |
| NSAIDs | Hemorrhage | |
| Barbiturates, codeine | Erythema multiforme | |
| Anesthetics (local) | Benzocaine, procaine HCl, lidocaine | Taste disorders |
| Antiarrhythmics | Procainamide | Lupus-like reaction |
| Quinidine | Lichenoid mucosal reaction | |
| Antiarthritic, antipyretic, anti-inflammatory | Allopurinol, auranofin, colchicine, dexamethasone, hydrocortisone, levamisole, D-penicillamine, phenylbutazone, salicylates, 5-thiopyridoxine Gold salts | Taste disorders Taste disorders, lichenoid reaction, oral pigmentation, vesiculo-ulcerative stomatitis |
| Antibiotics | All | Oral candidiasis |
| Erythromycin | Hypersensitivity reaction, vesiculo-ulcerative stomatitis | |
| Penicillin | Hypersensitivity reaction, erythema multiforme, vesiculo-ulcerative stomatitis | |
| Chloramphenicol, ciprofloxacin, clindamycin, dapsone, isoniazid, sulfa antibiotics, tetracyclines | Erythema multiforme | |
| Minocycline | Melanosis | |
| Chlorhexidine | Brown pigmentation of teeth & tongue | |
| Ampicillin, cefamandole, ethambutol, hydrogen chloride, griseofulvin, lincomycin, metronidazole, niridazole, sulfasalazine, tetracyclines | Taste disorders | |
| Anticoagulants | All | Hemorrhage |
| Anticonvulsants | Carbamazepine | Erythema multiforme, taste disorders |
| Phenytoin | Erythema multiforme, gingival enlargement, taste disorders | |
| Antidiarrheal agents | Bismuth | Dark pigmentation of tongue |
| Antihistamines | All | Salivary dysfunction |
| Chlorpheniramine maleate | Taste disorders | |
| Antihypertensives | All | Salivary dysfunction |
| Calcium-channel blockers | Gingival enlargement | |
| Angiotensin-converting enzyme inhibitors | Vesiculo-ulcerative stomatitis, pemphigus vulgaris | |
| Chloramphenicol | Vesiculo-ulcerative stomatitis | |
| Hydralazine | Lupus-like reaction, erythema multiforme | |
| Methyldopa | Lupus-like reaction and lichenoid mucosal reaction | |
| Thiazide diuretics | Lichenoid mucosal reaction | |
| Minoxidil, verapamil | Erythema multiforme | |
| Acetazolamide, amiloride, captopril, diazoxide, diltiazem, enalapril, ethacrynic acid, nifedipine | Taste disorders | |
| Antilipidemics | Cholestyramine, clofibrate | Taste disorders |
| Antimycotics | Griseofulvin | Erythema multiforme, black pigmentation of the tongue |
| Amphotericin B | Taste disorders | |
| Antineoplastics | All | Oral candidiasis, oral hemorrhage, recurrent oral viral infections, aphthous stomatitis, vesiculo-ulcerative stomatitis |
| Anti-parkinsonian | All | Salivary dysfunction |
| Levodopa | Taste disorders | |
| Antireflux agents | All | Salivary dysfunction |
| Cimetidine | Erythema multiforme | |
| Antithyroids | Carbimazole, methimazole, methylthiouracil, propylthiouracil, thiouracil | Taste disorders |
| Antioxidants | Octyl gallate | Allergic ulcerations |
| Anxiolytics | Benzodiazepines | Salivary dysfunction |
| Chelating agents | Penicillamine | Ulcers and pemphigus vulgaris |
| Corticosteroids, immunosuppressants, antiproliferatives | All Azathioprine, bleomycin, carmustine, doxorubicin, 5-fluorouracil, methotrexate, vincristine sulfate | Oral candidiasis, recurrent oral viral, infections, vesiculo-ulcerative stomatitis Taste disorders |
| Cyclosporin | Gingival enlargement | |
| Hypoglycemics | Sulfonylurea agents | Erythema multiforme |
| Glipizide, phenformin and derivatives | Taste disorders | |
| Muscle relaxants | All | Salivary dysfunction |
| Baclofen, chlorzoxazone | Taste disorders | |
| Others | Etidronate, germine monoacetate, idoxuridine, iron sorbitex, vitamin D | Taste disorders |
| Psychotherapeutics | All | Salivary dysfunction |
| Glutethimide, meprobamate | Erythema multiforme | |
| Phenothiazines | Oral pigmentation, tardive dyskinesia | |
| Lithium carbonate | Erythema multiforme, taste disorders | |
| Trifluoperazine HCl | Taste disorders | |
| Sympathomimetics | Amphetamines, amrinone | Taste disorders |
| Vasodilators | Bamifylline hydrogen chloride, dipyridamole, nitroglycerin patch, oxyfedrine | Taste disorders |
HCl, hydrogen chloride; NSAIDs, nonsteroidal anti-inflammatory drugs.
Diseases of the Heart
Several recent epidemiologic studies have demonstrated an association, but not a causal relationship, between heart disease and dental/periodontal diseases.1–5 Periodontal pathogens and certain serologic proteins found in the gingival sulcus (particularly C-reactive proteins) have been found in carotid atheromas and shown to induce platelet aggregation. However, the role of periodontal infection as a risk factor for cardiovascular disease requires further scientific validation. Recent data have further demonstrated a possible link between periodontal conditions and systemic measures of inflammation. Intensive periodontal treatment resulted in acute, short-term systemic inflammation (increased levels of C-reactive protein, interleukin-6, and the endothelial-activation markers soluble E-selectin and von Willebrand factor), as well as mild endothelial dysfunction. However, importantly, 6 months after therapy, without any adverse events, marked benefits in periodontal health were statistically associated with improvement in endothelial function.6
The treatment of cardiovascular diseases with drugs also has deleterious oral consequences. For example, antihypertensive medications have been shown to cause salivary dysfunction (as in the cases of diuretics, calcium channel blockers, β-blockers), gingival enlargement (calcium channel blockers), lichenoid mucosal reactions (thiazide diuretics), and disturbances in taste (ACE inhibitors, calcium channel blockers). Higher salt detection thresholds have also been observed in persons with hypertension.7 Consideration of possible alteration of drug regimens is appropriate.
Persons who have undergone cardiac transplantation and are receiving postoperative immunosuppressive pharmacologic regimens must be evaluated for potential oral complications. Immunosuppressive therapy increases the prevalence of oral opportunistic infections such as reactivation of herpes simplex virus and overgrowth of C. albicans. Cyclosporine, a frequently used antirejection drug, has been reported to cause gingival enlargement in up to 13% to 85% of patients.8
Consideration must be given to cardiac conditions before dental treatment is undertaken. Patients receiving anticoagulation therapy may present with hemorrhagic lesions of oral mucosal tissues (see “Cerebrovascular Diseases” later). Antibiotic prophylaxis is recommended for persons with cardiac valvular abnormalities at risk for developing subacute bacterial endocarditis (Table 92-3). Recent modification of the antibiotic recommendations simplified and clarified the regimen to reduce overuse of antibiotics, potential adverse effects, and drug resistance.9 Dental procedures for which endocarditis prophylaxis is reasonable (see Table 92-3) are events that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa. The regimen for antibiotic prophylaxis is provided in Table 92-4.
Table 92-3 Cardiac Conditions Associated with the Highest Risk of Adverse Outcome from Endocarditis for Which Prophylaxis with Dental Procedures Is Reasonable
* Except for the conditions listed above, antibiotic prophylaxis is no longer recommended for any other form of CHD.
† Prophylaxis is reasonable because endothelialization of prosthetic material occurs within 6 months after the procedure.
From Lockhart PB, Loven B, Brennan MT, Fox PC. The evidence base for the efficacy of antibiotic prophylaxis in dental practice. J Am Dent Assoc. 2007;138(4):458-474; and Wilson W, Taubert KA, Gewitz M, et al. Prevention of infective endocarditis: guidelines from the American Heart Association: a guideline from the American Heart Association Rheumatic Fever, Endocarditis and Kawasaki Disease Committee, Council on Cardiovascular Disease in the Young, and the Council on Clinical Cardiology, Council on Cardiovascular Surgery and Anesthesia, and the Quality of Care and Outcomes Research Interdisciplinary Working Group. J Am Dent Assoc. 2007;138(6):739-745, 747-760.

Although the dental office environment and dental treatment can increase heart rates and blood pressures, treatment can be safely rendered to patients with ischemic heart disease with adequate anxiety and pain control.10 The use of local anesthetics with epinephrine can be a concern in the treatment of cardiac patients because of the effect of increased heart rate, stroke volume, and cardiac output. However, at low doses, epinephrine has been found to have few of these systemic effects and in stable cardiovascular patients it can be safely used. For patients with a questionable cardiac history, 0.04 mg of epinephrine should be the maximum dose given (≈two 1.8-mL carpules of local anesthetic with 1 : 100,000 epinephrine), whereas unstable cardiac patients should receive epinephrine only for emergency dental treatment.
Malignant Neoplasms
Oropharyngeal cancer involves the soft palate, tonsil, base of the tongue, and vallecula and is diagnosed in nearly 9000 men and women in the United States annually.11 Cancers of the oral cavity and pharynx, which represent 2.1% of all neoplasms in the United States, have a direct and frequently permanent deleterious effect on oral health and function. Although men experienced a much greater likelihood of developing oral-pharyngeal cancer in the past, the male-female ratio is now 2 : 1. The prevalence and mortality of oral cancers increase with age, and the major preventable risk factors are tobacco use and excessive alcohol consumption.
Most of the remaining 10% of head and neck tumors are salivary gland tumors or lymphomas; further, approximately 1% of all tumors originate below the clavicles and metastasize to the head and neck.12 Accordingly, visual inspection and palpation of the head and neck region must include lymph nodes, muscles of mastication and facial expression, and salivary glands. Furthermore, a histopathologic examination is required of all nonhealing head, neck, and oral lesions.
Early detection of oral cancer is critical because patients with early-stage tumors have considerably better survival rates than those with late-stage cancers that have already spread to regional tissues and the lymphatic system. For example, 5-year survival rates for small and localized tongue cancers (stage I and II) and those tongue cancers with lymph node involvement and possible metastasis (stage III and IV) are 67% and 30%, respectively. Accordingly, since 1980, the American Cancer Society has recommended a cancer-related checkup every 3 years for persons aged 20 to 39 years and annually for individuals 40 years and older.13 This is particularly relevant for the elderly population, which sees their dental practitioner less frequently than their younger counterparts, and in particular, older edentulous adults.
Treatment for oral-pharyngeal neoplasms includes surgery, radiation therapy, and chemotherapy, depending on the tumor stage and extent of regional spread.14 Extensive removal of the cancerous growth and affected lymph nodes can result in significant facial disfiguration, dysphagia, altered speech and mastication, trismus, facial and oral paresthesia, salivary gland dysfunction, and diminished neck and shoulder mobility. Head and neck radiation is frequently used after surgery for the treatment of residual and microscopic disease; however, it also has significant adverse effects. These sequelae include mucositis, stomatitis, dysphagia, permanent salivary gland dysfunction, smell and taste dysfunction, oral microbial infections (e.g., reactivation of herpes simplex and varicella zoster viruses, C. albicans infections), and increased risk of developing osteoradionecrosis.14
Recent findings of osteonecrosis of the maxilla and mandible have been associated with the bisphosphonate class of antiosteoclastic medications. A majority of the reported cases were found in patients being treated for osteometastatic breast carcinoma or multiple myeloma. The pathophysiology of the disease has not yet been determined.15
Cerebrovascular Diseases
The motor, sensory, and cognitive alterations that accompany cerebrovascular diseases have deleterious effects on oral health and function. A cerebrovascular accident (CVA) can cause permanent oral sensory and motor deficits, resulting in poor tongue function and lip seal, difficulty eating and drinking, impaired use of dentures, and visuospatial problems with adverse social and psychologic consequences.16 Nutritional deficiencies and diminished quality of life can result from impaired food and fluid intake.
Anticoagulation therapy, the standard preventive treatment after a stroke, will produce hemorrhage, petechiae, ecchymoses, and purpura of all oral mucosal tissues. Dental treatment can be safely performed if the prothrombin time is within twice the normal range or if the international normalized ratio (INR) is less than 3.17 However, if excessive dental-alveolar surgery is planned, conversion to low-molecular-weight heparin or heparinization in a hospital setting is recommended. Aspirin use is popular in adults at risk for cardiovascular thrombotic events, and low-dose aspirin is an excellent preventive agent; however, its antiplatelet properties have contributed to a perceived increased risk for bleeding after dental extractions. For most patients requiring simple oral surgical procedures, if local hemostatic and conservative surgical techniques are used, discontinuation of aspirin may not be necessary.17
Head and neck radiographic findings and oral/periodontal status may aid in identification of persons at risk of CVAs. Carotid calcifications of atherosclerotic plaques have been found on 4% of panoramic radiographs of asymptomatic persons older than 55 years.18 In addition, periodontal disease and tooth loss are associated with increased risk of stroke.19,20 It is hypothesized that the infectious burden of oral disease can initiate proliferation of inflammatory cells and clotting factors resulting in atherogenesis and thromboembolic events.20 In addition, periodontal bacteria have been isolated from the atheromatous plaques after a CVA. The evidence to support a CVA-periodontal disease relationship is stronger than that found in investigations of cardiovascular and oral diseases.
Pulmonary Diseases
A common link between pulmonary diseases (COPD; bronchitis, asthma, and emphysema) and oral health is smoking. Smoking, one of the two preventable causes of oral cancer (see “Malignant Neoplasms” earlier), is also associated with benign oral mucosal pathology (nicotinic stomatitis, oral fungal infections). Little is known regarding the direct effects of COPD on oral health, yet it is well established that a common treatment modality of COPD (corticosteroids) has many oral consequences.21 Chronic use of corticosteroids suppresses the hypothalamic-pituitary-adrenal axis that can result in acute adrenal insufficiency during stress. Therefore steroid replacement therapy is sometimes required for extensive dental and surgical procedures.21 Many patients use steroid inhalers that should be brought to all dental appointments for use if necessary to ensure protection of a patent airway. Chronic use of systemic and inhaled corticosteroids also predisposes patients to oral fungal infections. Finally, nitrous oxide use is contraindicated in persons with severe COPD, secondary to oxygen-driven respiratory function.
Aspiration pneumonia, a common condition, particularly in hospitalized and older adults with compromised host defense mechanisms, is caused by the aspiration of gastric or oropharyngeal secretions. Oropharyngeal swallowing dysfunction, a consequence of neuromuscular and cerebrovascular diseases, debilitation, salivary hypofunction, and medications, is a frequent risk factor for aspiration pneumonia.22 Colonization of the oropharynx with gram-negative bacilli predisposes to bacillary pneumonia.23 A major source of anaerobe infection is the gingival crevice. Furthermore, the prevalence of bacterial colonization increases with poor oral hygiene and periodontal disease. Therefore patients at risk should receive routine dental examinations and treatment, and they may benefit from daily antimicrobial rinses.24 Broad-spectrum antibiotics are the standard treatment regimen for pneumonia. Extended antibiotic use increases the risk of developing oral fungal infections and antibiotic resistance.
Tuberculosis, a major global health problem caused by the spread of Mycobacterium tuberculosis, manifests infrequently in the oral cavity. The classic oral mucosal lesion is a painful, deep, irregular ulcer on the dorsum of the tongue, with additional sites including the palate, lips, buccal mucosa, and gingival.25 M. tuberculosis can also infect the cervical and submandibular lymph nodes (referred to as scrofula) and rarely affects the salivary glands.26
Oral tuberculosis lesions require diagnosis and appropriate antimicrobial management, as well as education on possible transmission via infected oral sites. A recent investigation reported positive oral cultures of M. tuberculosis from samples of saliva, dental plaque, caries lesions, and denture plaque collected from tuberculosis patients, demonstrating the possibility of oral infectivity of these patients.27 Interestingly, detection rates from these oral sites using polymerase chain reaction techniques were considerably higher (between 89% and 100% detection rates) than traditional culture methods (0% to 17%).28 With the growing rate of human immunodeficiency virus/acquired immunodeficiency syndrome in the world, a disease that frequently manifests with tuberculosis, clinicians must be familiar with infection control procedures to protect workers against exposure to pathologic and possibly aerosolized microorganisms.
Endocrine and Exocrine Disorders
Diabetes Mellitus
The presence or absence of diabetes and the degree of glucose metabolic control in patients significantly influence the level and severity of diabetes-related oral diseases. Patients who control their diabetes have fewer oral health problems than those with poorly controlled diabetes,29 and some data suggest that persons with controlled diabetes have the same incidence of oral disease as the general population.30 Alternatively, poorly controlled diabetes is associated with a plethora of oral health problems. The most common oral disease seen in persons with diabetes and in greater prevalence than persons without diabetes is periodontal disease.29,31 Many studies have shown that poor glycemic control precedes the incidence and progression of periodontitis. Furthermore, there is an association between severe periodontitis and an increased risk of poor glycemic control.16,29,32
Several mechanisms have been proposed to explain the increased susceptibility of persons with diabetes to periodontal diseases including alterations in host response, subgingival microflora, collagen metabolism, vascularity, gingival crevicular fluid, and heredity patterns.32 Multiple pathophysiologic mechanisms (e.g., compromised neutrophil function; decreased phagocytosis and leukotaxis) have also been implicated in the increased alveolar bone loss found in persons with diabetes,29,30 increased tendency for more active carious lesions and missing teeth,33 and increased susceptibility to oral infections and mucosal lesions.34 Autoimmune phenomena have been suggested as the cause of the increased prevalence of oral lichen planus in persons with diabetes.35
Diabetes predisposes an individual to sensory and peripheral neuropathies, which inhibit pain perception and may produce chemosensory deficits such as impaired taste function and decreased smell sensitivity.30 This sensory dysfunction can inhibit the ability to maintain a proper diet, which leads to poor glycemic regulation. Persons with diabetes also have reported increased complaints of glossodynia and stomatopyrosis (burning mouth syndrome), as well as increased complaints of dry mouth (xerostomia). There is no consensus demonstrating a relationship between glycemic control and salivary gland dysfunction. However, the xerostomic complaints may be due to a variety of reasons including salivary gland basement membrane changes and diabetes-associated thirst.



