Oral infections commonly originate from an odontogenic source in adults and from tonsil and lymphatic sources in children. Odontogenic infections arise from advanced dental caries or periodontal disease. Oral trauma, radiation injury, chemotherapy mucositis, salivary gland infection, lymph node abscess, and postoperative infection are potential nonodontogenic sources of infections that could potentially be life threatening. This article reviews the serious nature and potential danger that exists from oral infection and the antibiotics available to treat them are reviewed. Successful treatment requires an understanding of the microflora, the regional anatomy, the disease process, the treatment methods available, and interdisciplinary team collaboration.
Oral infections commonly originate from an odontogenic source in adults and from tonsil and lymphatic sources in children. Bacterial contamination of adjacent sterile tissue with normal oral flora result in infections the microbiology of which is usually predictable, and together with implementation of appropriate antibiotic options, can lead to successful treatment. Odontogenic infections arise as a result of advanced dental caries or from periodontal disease. Dental disease produces pulpitis, which may progress to periapical abscesses and can spread through bone, soft tissue, and into deeper structures. Periodontal infections from gingivitis, periodontitis, or periodontal abscess may be severe and also spread to deeper structures. Serious oral infections that go untreated may spread superiorly to the orbits and brain, to the retropharyngeal space or pleural space resulting in an empyema. Hematogenous spread may result in endocarditis, seeding of prosthetic material and other metastatic foci. Oral trauma, radiation injury, chemotherapy mucositis, salivary gland infection, lymph node abscess, and postoperative infection are potential nonodontogenic sources of infections that could potentially be life threatening. This article reviews the serious nature and potential danger that exists from oral infection and the antibiotics available to treat them. Successful treatment requires an understanding of the microflora, the regional anatomy, the disease process, the treatment methods available, and interdisciplinary team collaboration.
Anatomy
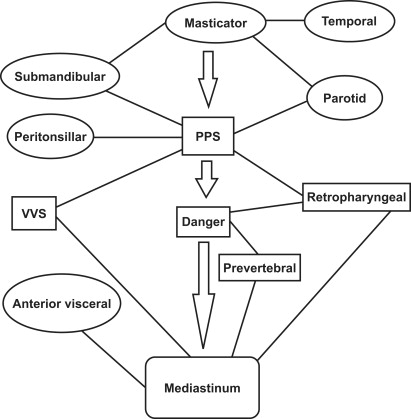
Oral infections spread in a pathway of least resistance often into the oral cavity or into the deep spaces of the neck, which may become life threatening. Deep-space infections originate most commonly from odontogenic sources in adults and from tonsil and other lymphatic sources in children. Spaces in the neck are created between the superficial, middle and deep layers of the deep cervical fascia. These spaces are interconnected ( Fig. 1 ). Three posterior pharyngeal spaces, the retropharyngeal space (RPS), the danger space (DS), and the prevertebral space (PVS), and a lateral pharyngeal space, the visceral vascular space (VVS), extend from the skull base to the mediastinum and beyond. The RPS extends to the upper mediastinum and contains the nodes of Rouviere, which involute by age 6 years; the RPS can rupture posteriorly into the DS. The DS extends to the inferior mediastinum; it lies just behind the RPS, between the alar anteriorly and the prevertebral fascia posteriorly. The PVS lies behind the DS and may extend to the coccyx as it has the vertebral body as the posterior wall and prevertebral fascia as the anterior boundary. Laterally, the VVS, which contains all 3 layers of the deep cervical fascia, extends from the skull base behind the parapharyngeal space to the mediastinum. The VVS contains the carotid artery, jugular vein, and vagus nerve. Smaller lateral suprahyoid spaces (temporal, masticator, submandibular, peritonsillar, and parotid) empty into the parapharyngeal space (PPS), which has access to mediastinum by way of the the RPS and VVS. The PPS is also known as the pharyngomaxillary space or lateral pharyngeal space. The PPS is divided into anterior and posterior portions. The anterior component contains parapharyngeal fat and the tonsillar fossa. It has no boundaries and may access other spaces; infections here are considered surgical emergencies. The posterior component of the PPS is a neurovascular space and infections here are generally limited to the capsule of the lymph node. The anterior infrahyoid neck has 2 additional spaces: the anterior visceral space (AVS) or pretracheal space extending from the thyroid cartilage to the superior mediastinum and the suprasternal space of Burns.
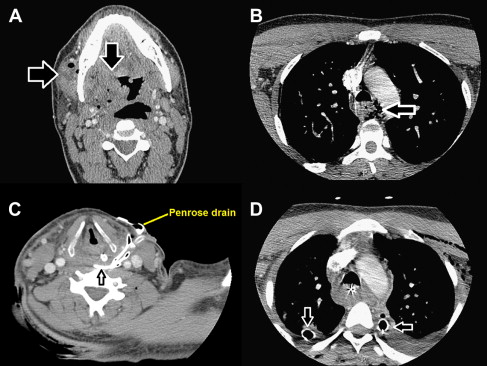
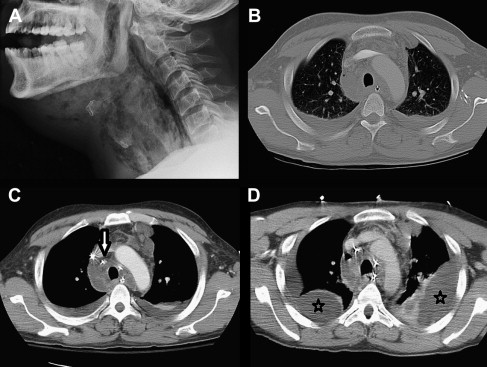
Lateral neck radiographs are a useful screening tool, with a sensitivity of 84% and specificity of 100%. An RPS abscess can be identified here by measuring the distance from the vertebra to the pharyngeal air space. An abscess is considered present when the distance at C2 greater than 7 mm, at C6 greater than 14 mm (in children), and C6 greater than 22 mm (in adults). The computed tomography (CT) scan is the workhorse for deep and superficial oral-facial infections. CT scans evaluating deep neck-space infections must include the mediastinum to rule out mediastinitis. Early recognition and treatment of mediastinitis can prevent the progressive sequela of respiratory failure requiring prolonged intensive care treatment ( Figs. 2 and 3 ).
Oral microbiology
Odontogenic Infections
The type of bacteria found within odontogenic infections are part of the microbiota of the oral cavity. These infections are frequently polymicrobial and their invasiveness may be determined by the specific combinations present as specific bacteria vary in their pathogenicity. More than 700 bacterial species have been identified in the oral cavity, although less than 1% are cultured routinely in the clinical laboratory. In addition, eradication of all oral flora is not required for treatment of odontogenic infections, as most are nonpathogenic commensals. Ecologic niches exist within the oral cavity, whereby normal colonizing bacteria reside within biofilms. These biofilms are comprised of polysaccharides that have 2 functions: allowing bacteria to live in a protected milieu and forming a barrier against potential pathogens.
In the oral cavity, more than 80% of the cultured bacteria include streptococci , Peptostreptococcus , Veillonella , Lactobacillus , Actinomyces and Corynebacterium . Quantitative measurements of the oral flora indicate that most bacteria are anaerobes in specific locations. Although specific organisms are located in most areas of the oral cavity, it is not a homogeneous environment. Certain bacteria colonize different parts of the mouth. Streptococcus salivarius and Veillonella colonize the tongue, buccal mucosa, and saliva. Streptococcus sanguinis, Streptococcus mutans, Streptococcus mitis and Actinomyces viscosus are found on tooth surfaces. The gingival crevice contains the anaerobes Fusobacterium , Porphyromonas , Prevotella , and anaerobic spirochetes.
The normal oral flora may be altered with tobacco use, pregnancy, diet, nutrition, age, oral hygiene, deciduous teeth eruption, dental caries, periodontal disease, antibiotics, hospitalization, and by genetic or racial factors. In these situations, commensal flora may become pathogenic and cause tissue inflammation and destruction. Plaque is a supragingival biofilm that is located on the tooth surface above the gingival margin and can produce dental caries from bacterial byproducts. These plaques are composed of gram-positive facultative (grows with or without oxygen) and microaerophilic (requires low oxygen) cocci and rods. Bacteria found within caries may cause pulpitis or endodontic infection, and potentially extend down the root canal to produce a periapical abscess. This abscess can perforate the alveolar bone and extend into the adjacent soft tissue of the face, or deep neck and lead to serious sequelae (see Fig. 2 ). Subgingival plaques and tartar are found below the gingival margin, and may lead to periodontal disease such as gingivitis, periodontitis, and periodontal abscess (see Fig. 3 ). These plaques comprise mainly gram-negative anaerobic (grows without oxygen) rods and motile forms, such as spirochetes. Necrotizing periodontal disease (acute necrotizing ulcerative gingivitis) is common in patients with very poor oral hygiene. It is caused by bacterial infection that includes anaerobes ( Prevotella intermedia and Fusobacterium ) as well as spirochetes such as Borellia and Treponema . This condition can progress to gangrenous stomatitis or noma in patients with weak immune systems or in the malnourished, leading to severe facial disfigurement.
The bacterial milieu within dental caries, gingivitis, and periodontitis differ from each other. Streptococcus mutans is clearly associated with dental caries, and is the only organism that has been isolated consistently from decayed dental fissures and carious teeth, compared with noncarious teeth. Conversely, the normal oral flora within subgingival plaques includes Streptococcus oralis , Streptococcus sanguinis , and Actinomyces . However, in the presence of gingivitis, the flora shifts to anaerobic gram-negative rods such as Prevotella intermedia , Capnocytophaga , and Peptostreptococcus . Adults with chronic periodontitis have oral flora that evolve to include anaerobic gram-negatives, motile organisms, and spirochetes, including Porphyromonas gingivalis , Prevotella intermedia , Actinobacillus actinomycetemcomitans , Tannerella forsythensis (formerly Bacteroides forsythensis ), and Treponema denticola . In contrast, early or juvenile periodontitis seen predominantly in adolescents is most commonly made up of Capnocytophaga and Actinobacillus actinomycetemcomitans .
Suppurative odontogenic infections such as deep neck-space infections from periapical abscesses is polymicrobial, commonly including both aerobic bacteria ( Streptococcus ) and anaerobes, specifically Peptostreptococcus, Actinomyces , pigmented Bacteroides , and Fusobacterium nucleatum . Patients with severe underlying illnesses may become colonized with pathogens such as methicillin-resistant Staphylococcus aureus (MRSA) and facultative gram-negative bacilli. These pathogens should be considered during selection of empiric antibiotic treatment.
Nonodontogenic Infections
Nonodontogenic oral infections are related to chemical, thermal, or trauma injury and may be associated with almost any microorganism. Sexually transmitted pathogens such as herpes simplex, Neisseria gonorrhea , and Treponema pallidum may be considered. Childhood viruses may be identified in the oral cavity. In chemotherapy-associated mucositis or in patients with human immunodeficiency virus (HIV) infection, opportunistic oral infections should be considered and may include Candida, Aspergillus, Mucormycosis , mixed gram-negatives, herpetic gingivostomatitis, and Histoplasma capsulatum .
Oral microbiology
Odontogenic Infections
The type of bacteria found within odontogenic infections are part of the microbiota of the oral cavity. These infections are frequently polymicrobial and their invasiveness may be determined by the specific combinations present as specific bacteria vary in their pathogenicity. More than 700 bacterial species have been identified in the oral cavity, although less than 1% are cultured routinely in the clinical laboratory. In addition, eradication of all oral flora is not required for treatment of odontogenic infections, as most are nonpathogenic commensals. Ecologic niches exist within the oral cavity, whereby normal colonizing bacteria reside within biofilms. These biofilms are comprised of polysaccharides that have 2 functions: allowing bacteria to live in a protected milieu and forming a barrier against potential pathogens.
In the oral cavity, more than 80% of the cultured bacteria include streptococci , Peptostreptococcus , Veillonella , Lactobacillus , Actinomyces and Corynebacterium . Quantitative measurements of the oral flora indicate that most bacteria are anaerobes in specific locations. Although specific organisms are located in most areas of the oral cavity, it is not a homogeneous environment. Certain bacteria colonize different parts of the mouth. Streptococcus salivarius and Veillonella colonize the tongue, buccal mucosa, and saliva. Streptococcus sanguinis, Streptococcus mutans, Streptococcus mitis and Actinomyces viscosus are found on tooth surfaces. The gingival crevice contains the anaerobes Fusobacterium , Porphyromonas , Prevotella , and anaerobic spirochetes.
The normal oral flora may be altered with tobacco use, pregnancy, diet, nutrition, age, oral hygiene, deciduous teeth eruption, dental caries, periodontal disease, antibiotics, hospitalization, and by genetic or racial factors. In these situations, commensal flora may become pathogenic and cause tissue inflammation and destruction. Plaque is a supragingival biofilm that is located on the tooth surface above the gingival margin and can produce dental caries from bacterial byproducts. These plaques are composed of gram-positive facultative (grows with or without oxygen) and microaerophilic (requires low oxygen) cocci and rods. Bacteria found within caries may cause pulpitis or endodontic infection, and potentially extend down the root canal to produce a periapical abscess. This abscess can perforate the alveolar bone and extend into the adjacent soft tissue of the face, or deep neck and lead to serious sequelae (see Fig. 2 ). Subgingival plaques and tartar are found below the gingival margin, and may lead to periodontal disease such as gingivitis, periodontitis, and periodontal abscess (see Fig. 3 ). These plaques comprise mainly gram-negative anaerobic (grows without oxygen) rods and motile forms, such as spirochetes. Necrotizing periodontal disease (acute necrotizing ulcerative gingivitis) is common in patients with very poor oral hygiene. It is caused by bacterial infection that includes anaerobes ( Prevotella intermedia and Fusobacterium ) as well as spirochetes such as Borellia and Treponema . This condition can progress to gangrenous stomatitis or noma in patients with weak immune systems or in the malnourished, leading to severe facial disfigurement.
The bacterial milieu within dental caries, gingivitis, and periodontitis differ from each other. Streptococcus mutans is clearly associated with dental caries, and is the only organism that has been isolated consistently from decayed dental fissures and carious teeth, compared with noncarious teeth. Conversely, the normal oral flora within subgingival plaques includes Streptococcus oralis , Streptococcus sanguinis , and Actinomyces . However, in the presence of gingivitis, the flora shifts to anaerobic gram-negative rods such as Prevotella intermedia , Capnocytophaga , and Peptostreptococcus . Adults with chronic periodontitis have oral flora that evolve to include anaerobic gram-negatives, motile organisms, and spirochetes, including Porphyromonas gingivalis , Prevotella intermedia , Actinobacillus actinomycetemcomitans , Tannerella forsythensis (formerly Bacteroides forsythensis ), and Treponema denticola . In contrast, early or juvenile periodontitis seen predominantly in adolescents is most commonly made up of Capnocytophaga and Actinobacillus actinomycetemcomitans .
Suppurative odontogenic infections such as deep neck-space infections from periapical abscesses is polymicrobial, commonly including both aerobic bacteria ( Streptococcus ) and anaerobes, specifically Peptostreptococcus, Actinomyces , pigmented Bacteroides , and Fusobacterium nucleatum . Patients with severe underlying illnesses may become colonized with pathogens such as methicillin-resistant Staphylococcus aureus (MRSA) and facultative gram-negative bacilli. These pathogens should be considered during selection of empiric antibiotic treatment.
Nonodontogenic Infections
Nonodontogenic oral infections are related to chemical, thermal, or trauma injury and may be associated with almost any microorganism. Sexually transmitted pathogens such as herpes simplex, Neisseria gonorrhea , and Treponema pallidum may be considered. Childhood viruses may be identified in the oral cavity. In chemotherapy-associated mucositis or in patients with human immunodeficiency virus (HIV) infection, opportunistic oral infections should be considered and may include Candida, Aspergillus, Mucormycosis , mixed gram-negatives, herpetic gingivostomatitis, and Histoplasma capsulatum .
Antibacterials
The proper selection of antibacterials has a twofold benefit: (1) the rapid eradication of infection, which decreases the degree of tissue destruction; and (2) decreasing the use of inappropriate antibiotics to prevent the development of antibiotic resistance. In addition to becoming familiar with the indigenous microbiota of the oral cavity, the patient’s immune status, community-acquired versus nosocomial exposures, allergy profile, and previous antibiotic usage that may predispose to resistant organisms need to be considered. For example, if a patient has been treated with penicillin in the past and presents with a relapsed infection, it is likely that the offending pathogen is resistant to penicillin and will require an alternate antibiotic choice. In addition, antibiotics containing the narrowest spectrum based on results of culture and susceptibility testing should be selected.
β -Lactam Antibiotics
All β-lactams exert the same basic mechanism of action, the inhibition of bacterial cell wall synthesis by binding to penicillin-binding proteins. Although the exact pathway is unknown, it is thought that bactericidal antibiotics such as the penicillins irreversibly destroy cell walls through the production of hydroxyl radicals. Resistance to β-lactam antibiotics has been increasing through the production of a variety β-lactamases. These are bacteria-derived enzymes that promote resistance to β-lactam agents that are selected through antibiotic pressure. This phenomenon proves the importance of controlled antibiotic use and has resulted in government mandates to hospitals to form antibiotic stewardship programs.
Penicillins
Penicillin is the primary class of β-lactams and is divided into 5 groups:
- 1.
Natural penicillins
- 2.
First generation penicillin
- 3.
Second generation penicillin
- 4.
Third generation penicillin
- 5.
Fourth generation penicillin.
Natural penicillins
Penicillin G and penicillin V are natural penicillins and are most useful for non–β-lactamase producing gram-positive bacteria, such as streptococci, staphylococci, enterococci, gram-positive rods such as Listeria monocytogenes and most anaerobes (an important exception is Bacteroides ). Bacteria that are sensitive to natural penicillins tend to be more effectively inhibited by this group compared to the semi-synthetic penicillins. Penicillin penetrates the normal blood-brain barrier poorly but achieves therapeutic levels in the presence of inflamed meninges when administered in high intravenous doses. Oral penicillin V and intravenous/intramuscular penicillin G are interchangeable except against gram-negative organisms, as oral penicillin V is less active against Neisseria and Haemophilus . Penicillin G is bactericidal with the notable exception of Enterococcus for which it is bacterostatic and in some cases, resistant because of production of penicillinase. Therefore, serious enterococcal infections require synergistic combination therapy of a cell wall active agent (such as the penicillins or vancomycin) with gentamicin, which decreases protein synthesis. Gentamicin synergy is commonly reported as part of Staphylococcus and Enterococcus susceptibility testing. Penicillin and the semi-synthetic penicillins are cleared by the kidneys and require dose adjustment if the patient has abnormal renal function.
First generation penicillin
Nafcillin, oxacillin, cloxacillin, and dicloxacillin are antistaphylococcal penicillins resistant to hydrolysis by penicillinase. They are the drugs of choice for penicillin-resistant Staphylococcus aureus and Staphylococcus epidermidis but are not active against oxacillin-resistant staphylococci. They also cover streptococci including Streptococcus pneumoniae , Streptococcus viridans , Streptococcus pyogenes , and other hemolytic streptococci and anaerobic gram-positive bacilli such as Clostridium . This group is not superior to penicillin for the treatment of penicillin-susceptible streptococci, and if susceptibilities allow, penicillin should be used for infections with these organisms. Conversely, in the case of oxacillin-susceptible staphylococcal infections, this group is more active than vancomycin based on clinical and in vitro studies. These agents are not active against enterococci, Listeria monocytogenes , and gram-negative pathogens such as Neisseria .
This group of antibiotics is classically associated with acute kidney injury, specifically acute tubulointerstitial nephritis (TIN) that can be diagnosed by the presence of eosinophils in the urine or renal biopsy. If TIN is suspected, discontinuation of the antibiotic is often adequate for renal recovery. Nafcillin is metabolized primarily through the liver and to a lesser extent, through the kidneys. If nafcillin is to be used in patients with liver disease, close monitoring of liver functions is recommended. Nafcillin is stable in solution and may be used in the homecare setting as a continuous infusion for a 24-hour period. Complete blood count monitoring is recommended in addition to renal and liver functions, as neutropenia is reported if used for more than 3 weeks. The original penicillinase-resistant penicillin, methicillin, is no longer used because of a high incidence of TIN.
Second generation penicillin
Ampicillin and amoxicillin are aminopenicillins that have identical coverage as penicillin against the same non–β-lactamase containing gram-positive pathogens. This group has additional coverage against non–β-lactamase producing strains of Haemophilus influenzae , Escherichia coli , Proteus mirabilis , Salmonella , and Shigella but lacks coverage against Pseudomonas aeruginosa . The overall prevalence of ampicillin-resistant, β-lactamase producing nontypeable Haemophilus influenzae strains is 30%, but geographic variability exists. In addition to Haemophilus influenzae , other pathogens important in the pathogenesis of otitis media and sinusitis such as Moraxella catarrhalis may produce β-lactamases, resulting in resistance to the aminopenicillins. Therefore, knowledge of the local susceptibilities is recommended.
Aminopenicillins have an increased incidence of drug hypersensitivity reactions with rashes compared with other penicillins. This is most evident when these agents are used for the treatment of exudative tonsillitis in the face of infectious mononucleosis. Nonaminopenicillins should be considered for empiric therapy of exudative tonsillitis pending culture and monospot results. Comparing these 2 agents, amoxicillin has enhanced intestinal absorption (particularly at mealtime) and is preferable to oral ampicillin, which is destroyed by low gastric pH. Both middle ear fluid and serum levels are higher with the use of amoxicillin.
Third generation penicillin
Ticarcillin, the only third generation penicillin available, is less active than ampicillin against penicillin-resistant streptococci and relatively inactive against enterococci. Ticarcillin has a broader spectrum of activity against β-lactamases of organisms like Pseudomonas aeruginosa , Enterobacter , and Proteus. Ticarcillin is no longer available as a single drug because of potential hydrolysis by β-lactamases, and is used in combination with the β-lactamase inhibitor clavulanate. This addition has further expanded the coverage of ticarcillin-clavulanate to include Staphylococcus aureus (except for MRSA) and anaerobes. Ticarcillin-clavulanate is a disodium salt, which may result in volume overload and may cause a bleeding diathesis by prolonging the bleeding time and interfering with platelet function, particularly in the presence of renal failure.
Fourth generation penicillin
Piperacillin is an acyl ureidopenicillin (extended spectrum β-lactam), which is a derivative of ampicillin with activity against gram-positive species, Neisseria , Haemophilus and many members of Enterobacteriaceae. It has excellent activity against anaerobes and is more active than ticarcillin against Pseudomonas aeruginosa . As opposed to ticarcillin, pipercillin may be used as a single agent. However, because of β-lactamase production by Pseudomonas aeruginosa and Enterobacter , a combination of pipercillin with the β-lactamase inhibitor tazobactam is commonly used.
β -Lactamase Inhibitors
β-Lactamase inhibitors such as clavulanate and sulbactam are weak β-lactam compounds, but when coadministered with β-lactam antibiotics, bind and inactivate β-lactamase enzymes. The commonly used combination agents include ampicillin-sulbactam, ampicillin-clavulanate, pipercillin-tazobactam, and ticarcillin-clavulanate. The net result is successful eradication of β-lactamase producing bacteria, particularly Haemophilus influenzae , Moraxella catarrhalis , Staphylococcus aureus , Bacteroides , and Enterobacteriaceae. Clinically, the oral combination of amoxicillin-clavulanate and intravenous combination of ampicillin-sulbactam are commonly used in the treatment of head and neck infections.
Cephalosporins
Cephalosporins represent a popular group of β-lactam agents that cover a broad spectrum of organisms and are easy to administer with low toxicity issues. They can often be used in place of penicillins when patients have a history of mild rashes associated with penicillin use. Conversely, cephalosporins should not be used in patients who describe anaphylaxis, angioedema, urticaria, or asthma when using penicillin. The half-lives of these agents vary, resulting in dosing ranges between once daily and four times daily depending on renal function. The pharmacokinetics allow for therapeutic levels in peritoneal, pleural, synovial fluid, and pericardial tissues with biliary concentrations that exceed serum levels. In terms of pneumococcal susceptibility, resistance or reduced susceptibility to any cephalosporin infers alteration in the bacterial penicillin-binding proteins and resistance to the entire group. They are considered active against most gram-positive pathogens and are divided into generations based on their spectrum of activity against aerobic and facultative gram-negative bacteria.
First-generation cephalosporins
Cefazolin, the most commonly used intravenous first-generation cephalosporin available is recommended for patients who are allergic to penicillin. It has similar activity against most gram-positive cocci including Staphylococcus aureus , group A β-hemolytic Streptococcus ( Streptococcus pyogenes ), and penicillin-susceptible Streptococcus pneumonia . It is used for surgical prophylaxis for head and neck surgery that requires crossing the oropharyngeal mucosal barrier. Cefazolin lacks activity against oxacillin-resistant staphylococci, penicillin-resistant pneumococci, Listeria monocytogenes , and enterococci. In terms of gram-negative bacteria, coverage is more limited to enteric pathogens, such as most strains of Escherichia coli , Klebsiella pneumoniae , and Proteus mirabilis. Cefazolin is inactive against nonenteric gram-negatives such as Pseudomonas aeruginosa and Acinetobacter , indole-positive Proteus , Enterobacter , Serratia , and gram-negative cocci such as Neisseria meningococcus and Haemophilus influenzae . In terms of anaerobes, cefazolin lacks coverage of Bacteroides and should not be used if this pathogen is suspected.
The first-generation oral cephalosporins include cephalexin, cefadroxil, and cephadrine (not available in the United States). These agents are similar in antibacterial spectrum, but differ in dosing schedules. These agents have high oral bioavailability and are active against Streptococcus pyogenes . They are not useful against penicillinase-producing Streptococcus pneumoniae , Haemophilus Influenzae , and Moraxella catarrhalis , and are therefore not recommended for sinusitis, otitis media, or lower respiratory tract infections.
Second-generation cephalosporins
In the United States, second-generation cephalosporins include cefaclor, cefprozil, cefuroxime, and cefoxitin. This group has broader gram-negative coverage than the first-generation cephalosporins but less gram-positive activity. There are 2 basic subgroups. The first subgroup with activity against Haemophilus influenzae includes cefuroxime, the only intravenous formulation in this subgroup, which also covers strains of Enterobacter and indole-positive Proteus , compared with cefazolin. Intravenous and oral cefuroxime is stable against ampicillin-resistant, β-lactamase producing Haemophilus influenzae . It is the only second-generation cephalosporin to cross the blood-brain barrier and is approved for the treatment of Haemophilus influenzae meningitis. However, because of reports of treatment failures and delayed responses, third-generation cephalosporins are now the preferred treatment of Haemophilus influenzae . They are less active than amoxicillin against Streptococcus pneumoniae , specifically strains with intermediate susceptibility to penicillin and should not be used with strains that are fully resistant. Cefuroxime also covers β-lactamase producing Moraxella catarrhalis . In comparison, cefprozil is less active against Haemophilus influenzae and Streptococcus pneumoniae , and is inactive against Moraxella catarrhalis . Cefaclor is the least active of this group, with poor coverage of Moraxella catarrhalis and Haemophilus strains. This agent is also associated with serum sickness. The second subgroup is the cephamycins, which also covers anaerobes such as Bacteroides and includes agents such as cefoxitin, cefmetazole, and cefotetan. The spectrum of activity of cephamycins includes common aerobic and facultative gram-negatives and anaerobes and is optimal for gastrointestinal and pelvic infections, with no clear advantage in the prophylaxis or treatment of oral infections.
Third-generation cephalosporins
Ceftriaxone and cefotaxime cover many important infections because of their broad coverage, high potency, low toxicity issues and favorable pharmacokinetics, such as high levels in the cerebrospinal fluid. These compounds have less activity against gram-positive pathogens compared with the first-generation cephalosporins, although they are usually useful for pneumococci that have intermediate susceptibility to penicillin. Pneumococcal strains that are completely resistant to penicillin are commonly resistant to the third-generation cephalosporins as well. Agents such as cefixime and ceftibuten may be used for acute otitis media or sinusitis only when resistant pneumococci have been previously treated. Oral cefpodoxime, cefdinir, and cefditoren are technically third-generation cephalosporins but exert the same antibacterial activity as the second-generation agents. Cefpodoxime is considered the most active of the oral cephalosporins for the treatment of acute otitis media and sinusitis.
Third-generation cephalosporins have the advantage of being resistant to the common β-lactamases of gram-negative bacilli with enhanced activity against Enterobacteriaceae such as Escherichia coli , Serratia spp, Proteus mirabilis , indole-positive Proteus , Klebsiella , Citrobacter , and Enterobacter . Some Enterobacteriaceae have recently developed β-lactamase enzymes such as extended spectrum β-lactamases (ESBLs), carbapenemases and AmpC β-lactamases. These enzymes pose a growing threat to the continued usefulness of these agents.
There are 2 basic subgroups of third-generation cephalosporins based on coverage of Pseudomonas aeruginosa . One subgroup will lack pseudomonal coverage, including ceftriaxone, cefotaxime, cefdinir, cefditoren, cefotetan (a cephamycin), cefixime, ceftibuten, cefpodoxime and ceftizoxime. A second subgroup will cover Pseudomonas aeruginosa , the most commonly being ceftazidime. Ceftazidime has poor activity against gram-positives and should be reserved for Pseudomonas aeruginosa infections.
Ceftriaxone and cefotaxime are the only third-generation cephalosporins that maintain excellent activity against Streptococcus pneumoniae , including those isolates reported as intermediate or high-level resistance to penicillin. Conversely, third-generation agents such as ceftriaxone, cefotaxime, and ceftazidime achieve higher cerebrospinal fluid levels in the presence of inflamed meninges and are approved for the treatment of bacterial meningitis. If multidrug resistant pneumococcus is suspected, intravenous vancomycin can be added to ceftriaxone or cefotaxime. Ceftriaxone is considered more potent than cefotaxime against gram-positive pathogens and requires only single daily dosing. It can be used in intramuscular form for persistent otitis media and gonococcal infections.
Fourth-generation cephalosporins
Cefepime is the only fourth-generation cephalosporin available in the United States. It has enhanced penetration through the outer membrane of gram-negative bacteria and is less susceptible to inactivation by certain β-lactamases of gram-negative bacilli. As a result, 75% to 80% of Enterobacteriaceae that are resistant to ceftazidime are susceptible to cefepime. Cefepime is also active against gram-positive cocci such as Streptococcus pneumoniae and staphylococci compared with ceftazidime. However, both ceftazidime and cefepime usually have excellent activity against Pseudomonas aeruginosa , depending on susceptibility testing of the individual isolates and provide nonnephrotoxic and nonototoxic alternatives to aminoglycosides.
Fifth-generation cephalosporins
Cetobiprole is the only fifth-generation cephalosporin produced thus far, and is available in Europe. The fifth-generation cephalosporins are active against MRSA, ampicillin-resistant enterococci, Streptococcus pneumoniae , and Pseudomonas aeruginosa . They also share similar activity with many third- and fourth-generation cephalosporins against gram-negative bacilli.
Carbapenems
Carbapenems are a class of β-lactam antibiotics with the widest spectrum of antibacterial coverage because they are commonly resistant to β-lactamases. The 4 approved agents in the United States include ertapenem, imipenem-cilastatin, meropenem, and doripenem. Their general coverage includes (1) gram-positive organisms including Listeria and Enterococcus faecalis (but not against MRSA and vancomycin-resistant Enterococcus faecium ), (2) gram-negative organisms, including beta-lactamase producing Haemophilus influenzae , Neisseria gonorrheae , the Enterobacteriaceae, Pseudomonas aeruginosa , Acinetobacter , and ESBLs. Carbapenems other than ertapenem are the drugs of choice for the treatment of carbapenem-susceptible, multiresistant Acinetobacter baumannii infections, although carbapenem resistance is a growing problem and (3) anaerobes including Bacteroides fragilis , anaerobic gram-positive cocci, Fusobacterium, Prevotella , and Porphyromonas .
There are variations in the susceptibility of carbapenems. Ertapenem is the only carbapenem that has poor activity against Pseudomonas aeruginosa compared with doripenem, which is most effective, including strains resistant to antipseudomonal penicillins and cephalosporins. Although imipenem-cilastatin, meropenem, and doripenem may exhibit activity against Pseudomonas aeruginosa initially, resistance may occur when these agents are used as monotherapy and coadministration with aminoglycosides should be considered.
Imipenem-cilastatin, meropenem, and doripenem are useful for the treatment of a wide variety of infections including bacteremias, bone and soft tissue infections, pneumonia, and serious hospital-acquired or mixed infections. They may be used as single agents for the empiric treatment of unidentified infections pending culture results or when treatment with cephalosporins or penicillin has been unsuccessful.
Ertapenem has a narrower spectrum of activity compared with the other carbapenems. It is active against most Enterobacteriaceae and anaerobes but less useful for Pseudomonas aeruginosa , Acinetobacter , and gram-positive pathogens, such as penicillin-resistant pneumococci and enterococci. Unlike meropenem, it is not approved for meningitis although it penetrates the blood-brain barrier. It has the advantage of single daily dosing and is used in skin and soft tissue, pelvic, gastrointestinal infections, community-acquired pneumonia and urinary tract infections.
Imipenem is coadministered with cilastatin, an inhibitor of dehydropeptidase I, an enzyme that cleaves imipenem. Imipenem is more active against highly resistant pneumococci and has some activity against Enterococcus faecalis . Both imipenem and meropenem have excellent penetration into the cerebrospinal fluid in the presence of inflamed meninges. The main toxicity of imipenem is central nervous system (CNS) involvement with myoclonus, altered mental status and seizures, and should be used with caution in patients with underlying CNS or renal disease.
Meropenem has less central nervous system toxicity and may be used in patients with underlying CNS or renal disease. It has a spectrum of activity similar to imipenem, but is more active against Haemophilus influenzae . It is the only carbapenem approved for the treatment of bacterial meningitis.
Doripenem is the most recently approved carbapenem and, together with meropenem, has enhanced activity against gram-negative bacilli. Doripenem is the most active carbapenem against Pseudomonas aeruginosa and is approved for complicated intra-abdominal infections and urinary tract infections. Data suggest that doripenem may be used for nosocomial pneumonia and oral and dental surgical infections.
Monobactams
Aztreonam is the only monobactam available. Monobactams are β-lactams that have the β-lactam ring alone, and not fused to another ring. They are used exclusively for gram-negative aerobic bacterial infections and have no activity against gram-positive or anaerobic bacteria. They are very active against Haemophilus influenzae and Neisseria gonorrheae infections as well as Escherichia coli , Klebsiella , Serratia and Proteus but less activity against Pseudomonas aeruginosa compared with imipenem or ceftazidime. For patients who are allergic to penicillin, ertapenem can be added to clindamycin or vancomycin for the treatment of oral infections.
Aminoglycosides
Aminoglycosides including gentamicin, tobramycin, streptomycin and amikacin have bactericidal activity against susceptible gram-negative bacilli and may be additive or synergistic with penicillins or cephalosporins against gram-positive cocci or gram-negative bacilli. Aminoglycosides block protein synthesis and resistance has remained relatively low. Despite these properties, the toxicity issues with aminoglycosides often limit their use. Renal toxicity results in acute kidney injury ranging from 0% to 50%. Ototoxicity can produce irreversible cochlear and vestibular damage. Although few patients complain of hearing loss, damage is noted in up to 62% of asymptomatic high-frequency audiograms. Overall, the incidence is reported to be between 3% and 14%. A commonly used definition of drug-induced ototoxicity is an increased auditory threshold of 15 dB or greater at any of 2 or more frequencies. Toxicity is identified initially in the outer hair cells of the organ of Corti, although the exact interactions are unknown. Vestibular toxicity occurs in the type 1 hair cell of the ampullary cristae and is symptomatic with nausea, vomiting, and true vertigo. Neuromuscular blockade can result in weakness of respiratory muscles, dilated pupils, and flaccid paralysis, and can be rapidly reversed with intravenous calcium gluconate.
Macrolides
Macrolides activity to block bacterial protein synthesis comes from the presence of the macrolide ring. The commonly used macrolide antibiotics include erythromycin, azithromycin, and clarithromycin. Erythromycin has activity against streptococci and pneumococci compared with penicillin but has become less popular than azithromycin and clarithromycin because of gastrointestinal intolerance, more limited spectrum of activity, decreased oral absorption and a longer half-life. Specifically, most strains of Haemophilus influenzae are resistant to erythromycin, so that its use as monotherapy in otitis media is limited. Erythromycin may be an effective agent against Moraxella catarrhalis and respiratory pathogens such as Mycoplasma pneumoniae , Chlamydia pneumoniae , Legionella pneumophilia , and Bordatella pertussis . Erythromycin is also useful for Mycoplasma or pharyngitis caused by Chlamydiae. There are several issues that may limit the use of erythromycin. Resistance to erythromycin may develop early in treatment, including Haemophilus influenzae and Streptococcus pneumoniae . There is no activity against MRSA. Gastrointestinal distress is common but is improved with use of enteric-coated preparations. There is risk of inadequate absorption if taken with food. Reversible hearing loss can occur with high doses of intravenous erythromycin. Prolongation of QT interval is found with all macrolides. Significant drug interactions exist with statins, antiarrythmics, sildenafil citrate (Viagra), theophylline, cyclosporine, warfarin, carbamezapine, benzodiazepines, digoxin, methylprednisolone, alfentanil, and dopamine agonists. Compared with erythromycin and clarithromycin, azithromycin has more activity against gram-negative bacteria, particularly Haemophilus influenzae and Moraxella catarrhalis . Azithromycin also has the benefit of lacking the drug interactions listed earlier.
Clindamycin
Clindamycin is a semisynthetic derivative of lincomycin, a natural antibiotic produced by the actinobacterium Streptomyces lincolnensis . It is bacteriostatic by inhibiting protein synthesis. Clindamycin is an excellent agent for the treatment of infections of the oral cavity and surpasses penicillin in the eradication of streptococci in tonsillo-pharyngitis, likely because of the β-lactamase production of some of the polymicrobial flora, resulting in resistance to penicillin. It is effective against most pneumococci and streptococci and most penicillin-resistant staphylococci including some MRSA isolates. It also shows enhanced activity against most clinically important anaerobes, especially Bacteroides fragilis , although resistance is now being reported. It concentrates well in saliva, mucus, respiratory tissues, and bone, and is the drug of choice for the treatment of osteomyelitis with susceptible pathogens. From a head and neck standpoint, clindamycin is particularly useful in the treatment of the polymicrobial oral infections, including Bacteroides and other anaerobes common in chronic tonsillitis and deep neck abscesses of oral and dental origin. The main concerns with regard to clindamycin are gastrointestinal distress with nausea and vomiting and a risk of esophagitis. This risk can be minimized with ingestion during meals, and yogurt or acidophilus. Clostridium difficile pseudomembranous colitis is a complication that may occur after all antibacterial agents but has been classically associated with clindamycin. Treatment includes discontinuation of the antibiotic and treatment with oral metronidazole, vancomycin, or nitazoxanide. Clindamycin has poor penetration of the blood-brain barrier, and therefore not useful for the treatment of intracranial infections. Penicillin-resistant pneumococci are becoming increasingly resistant to clindamycin.
Metronidazole
Metronidazole is useful in the treatment of oral infections by virtue of its activity against clinically important anaerobes including Bacteroides , Prevotella , Fusobacterium , Peptostreptococcus (anaerobic Streptococcus ), and Clostridium . One study of metronidazole showed inhibition of periodontal pathogens, irrespective of its β-lactamase production, except for Actinomyces . Specifically, metronidazole relieves the pain of pharyngeal and tonsillar ulcers associated with Vincent angina and may improve the tonsillitis of infectious mononucleosis, inferring a significant role of anaerobic bacteria in these conditions. In addition, it is used in the treatment of perioral dermatitis, acute necrotizing gingivitis, and childhood granulomatous periorificial dermatitis.
Metronidazole lacks activity against all aerobic bacteria, an issue in the treatment of oral infections, which are often polymicrobial. Therefore, combination of metronidazole with other agents such as the penicillins, cephalosporins, and quinolones is required for the treatment of mixed infections such as tonsillitis, sinusitis, odontogenic disease, infected cholesteatoma, or deep neck abscesses. Patients treated with metronidazole need to be reminded to avoid alcohol consumption because of the risk of a disulfuram-like reaction.
Vancomycin
Given the increasing incidence of MRSA and penicillin-resistant pneumococcal infections, vancomycin use has become more prevalent. A glycopeptide antibiotic, it is of particular importance to otolaryngology-head and neck surgeons because of its use in combination with gram-negative and anaerobic antibiotics for head and neck infections, and because of its potential for vancomycin-associated ototoxicity. It is bactericidal against almost all Staphylococcus , Streptococcus , Pneumococcus , Enterococcus , and Clostridium species. One of the first reports of vancomycin usage included 6 cases of severe ototoxicity with high-frequency sensorineural hearing loss described in up to 12% and higher in the elderly. Concomitant use of aminoglycosides is believed to potentiate the toxicity of vancomycin. In rare cases, tinnitus and vertigo may develop and precede the hearing loss. The ototoxicity is reversible with discontinuation of the drug. If vancomycin dosing exceeds 2 g/d, monitoring for renal function and vancomycin trough levels between 15 and 20 μg/mL is recommended. Vancomycin is known to produce red man or red neck syndrome with rapid infusions in 3.4% to 11.2% of cases. Classically, patients experience a rapid onset of an erythematous rash and/or pruritis involving the head, neck, and upper trunk that may or may not be associated with angioedema and hypotension anaphylactoid reaction. This reaction resolves with discontinuation of vancomycin without other measures in most cases. The risk of this adverse reaction can be reduced by decreasing the rate of the infusion, and if necessary, the use of antihistamines. Reversible neutropenia occurs in 1% to 2% with a more recent report of thrombocytopenia with severe bleeding. There are reports of nephrotoxicity ranging from 0% to 12%, which increases with combined use of other nephrotoxic agents such as aminoglycosides.
Linezolid
Linezolid is a synthetic antibiotic that has activity against MRSA and vancomycin-resistant Enterococcus (VRE) and can be used for patients with penicillin allergies. Although this agent also has activity against pneumococcus, it lacks activity against penicillin-resistant strains. It has been used for the treatment of parotitis. The major concerns regarding linezolid include thrombocytopenia and pancytopenia (particularly with more than a 2-week course), high cost, serotonin syndrome when used in conjunction with monoamine oxidase inhibitor antidepressants, hypertension when used together with decongestants containing pseudoephedrine, ephedrine, or phenylephrine, and increasing reports of peripheral neuropathy and lactic acidosis.
Daptomycin
Daptomycin has rapid bactericidal activity against staphylococci, pneumococci, and enterococci including MRSA, vancomycin-intermediate Staphylococcus aureus and vancomycin-resistant Enterococcus isolates. In addition to aerobic gram-positive activity, it has in vitro activity against gram-positive anaerobes such as Peptostreptococcus and Clostridium perfringens although established guidelines for susceptibility testing are not available. It has the advantage of once daily intravenous dosing and is approved for skin and soft tissue infections, bacteremia, and right-sided endocarditis. The 2 caveats with daptomycin use are the lack of lung penetration, and therefore it is not indicated for the treatment of pneumonia, and increase in creatine phosphokinase (CPK) level and associated muscle toxicity.
Sulfonamides
Sulfonamides have been in existence since the 1930s and exert antimicrobial activity against many Haemophilus influenzae isolates. However, trimethoprim (TMP)-sulfamethoxazole (SMZ) should not be used as a first-line agent against otitis media, particularly when resistant respiratory pathogens are present. This class of bacteriostatic antibiotics has only variable activity against pneumococci, streptococci, anaerobes, and Moraxella catarrhalis . Therefore, it is common to use sulfa in combination with other agents such as SMZ with TMP, which is believed to potentiate the action of sulfonamides by the inhibition of folic acid synthesis and ultimately protein synthesis. Classically, TMP-SMZ has been used together with erythromycin for the treatment of acute otitis media and purulent rhinosinusitis against Haemophilus influenzae and pneumococci in the pediatric population. More recently, TMP-SMZ has been useful for the treatment of MRSA, although susceptibility testing needs to be done. TMP-SMZ has an effective role in the treatment and prevention of relapse of Wegener granulomatosis, as an adjuvant to immunosuppressive agents. It is the most common agent for the prophylaxis and treatment of Pneumocystis carinii , a cause of otitis media and mastoiditis in individuals infected with HIV with CD4 counts less than 200/mm 3 . Sulfonamides have several adverse reactions that require monitoring. These include rashes (ranging from mild morbilliform rashes to urticaria and Stevens Johnson syndrome), blood dyscrasias (ranging from aplastic anemia, agranulocytosis, and thrombocytopenia), nephrotoxicity, type 4 renal tubular acidosis, and drug interactions with phenytoin, rifampin, warfarin, oral hypoglycemics, methotrexate, and cyclosporine.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


