Recurrent aphthous stomatitis is a common oral ulcerative disease, affecting 10% to 15% of the general US population. This article reviews the epidemiology and clinical presentations of recurrent aphthous stomatitis, including diagnosis and management.
Recurrent aphthous stomatitis (RAS) in the oral cavity a painful ulcer that causes causing substantial morbidity in the United States and elsewhere. RAS is one of the most common oral ailments. These ulcers have been generally described to typically appear first in childhood and tend to abate around the third decade of life. Patients often report a family history of RAS. However, contrary to general belief, the burden of RAS among adults is high. RAS often is confused with intraoral ulcers associated with several systemic diseases or conditions. However, experts have suggested reserving the term recurrent aphthous stomatitis for recurrent ulcers confined to the mouth and seen in the absence of systemic disease. Recurrent ulcers that do not have all the typical clinical characteristics or a childhood onset may perhaps be termed aphthous-like ulcers and not labeled as RAS.
Clinical presentation
RAS anywhere in the oral cavity is painful, and is one of the most common oral ailments. The disease is characterized by recurring painful ulcers of the mouth that are round or ovoid and are surrounded by inflammatory halos. These ulcers typically appear first in childhood. RAS may present as small ulcers 2 to 8 mm in diameter, called minor aphthous ulcers , and may heal spontaneously in 10 to 14 days. Larger ulcers, often 1 cm or more in diameter, are called major recurrent aphthous ulcers . Herpetiform ulcers are a bunch of small pinpoint ulcers occurring close together that may later coalesce.
Severe RAS is a rare but extremely disabling disorder. The lower vestibule is the most commonly involved site. Most recurrent aphthous ulcers develop on freely movable nonkeratinized oral mucosa, including the buccal mucosa, vestibules, inner lips, under surface of the tongue, and soft palate. Although sometimes prodromal symptoms such as altered sensation or focal erythema or slight swelling may be present, these are usually ignored by most patients until the painful ulcers develop.
Epidemiology
Among the most commonly cited studies for RAS prevalence, only three are population-based, of which the only one performed in the United States involved school children and was based on the National Institute of Dental Research (renamed the National Institute of Dental Research and Craniofacial Research [NIDCR]) National Survey of Oral Health in US School Children (1986–1987). Although various factors have been reported to be associated with RAS, independent risk or causative factors of RAS have not been clearly established in population-based studies, and most evidence comes from convenience samples and clinic-based studies.
Historically, reports have provided varying estimates for prevalence of RAS, ranging from 1% to 66% among adults and 1% to 40% among children. Most of these estimates were derived from hospital-based studies that could be subject to several selection biases. Most of these reports likely overestimated RAS prevalence because of improper sampling design for the purpose of estimating true disease burden. Sampling design and selection of study populations seriously impact the conclusion of studies, and convenience samples can provide estimates that may not reflect reality. Results based on data from the Third National Health and Nutrition Examination Survey (NHANES III), analyzed with appropriate nesting and weighting statements to adjust the variance for the complex sampling design of the survey, can be generalized to the United States population. Such a study found a substantially lower prevalence of RAS (1.03% overall), which, when stratified by age, suggests a 0.85% prevalence among adults and 1.5% prevalence among children and adolescents.
This population-based study in the United States found that overall the prevalence of recurrent aphthous ulcers was 1030 per 100,000 persons (95% CI, 830–1220). The prevalence of RAS among children was 1500 per 100,000 (95% CI, 1090–1910), which was greater than that among adults, at 850 per 100,000 (95% CI, 630–1070). It is estimated that in the United States, at least 3 million people have RAS, of which approximately 2 million are aged 17 years or older and 1 million are younger than 17 years.
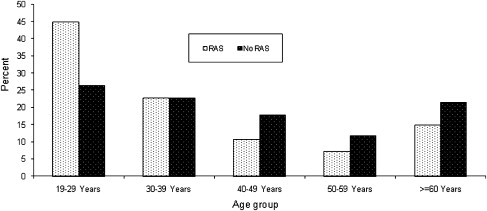
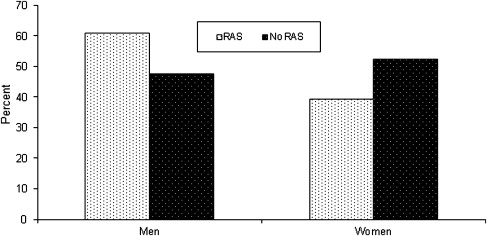
Multivariable analyses to determine independent risk indicators and risk factors in adults suggested that adjusted odds of RAS were greatest for persons aged 17 to 29 years (adjusted odds ratio [OR], 2.7; 95% CI, 1.4–5.5), men (adjusted OR, 1.7; 95% CI, 0.9–2.8), and persons with low serum insulin levels (OR, 2.0; 95% CI, 0.9–4.4). Never-smokers had greater risk for recurrent aphthous ulcers (OR, 9.2; 95% CI, 2.8–30.1) than people who smoked more than 10 cigarettes per day. Results from a separate analysis based on NHANES III data show RAS-associated age distribution and sex differences ( Figs. 1 and 2 ).
Epidemiology
Among the most commonly cited studies for RAS prevalence, only three are population-based, of which the only one performed in the United States involved school children and was based on the National Institute of Dental Research (renamed the National Institute of Dental Research and Craniofacial Research [NIDCR]) National Survey of Oral Health in US School Children (1986–1987). Although various factors have been reported to be associated with RAS, independent risk or causative factors of RAS have not been clearly established in population-based studies, and most evidence comes from convenience samples and clinic-based studies.
Historically, reports have provided varying estimates for prevalence of RAS, ranging from 1% to 66% among adults and 1% to 40% among children. Most of these estimates were derived from hospital-based studies that could be subject to several selection biases. Most of these reports likely overestimated RAS prevalence because of improper sampling design for the purpose of estimating true disease burden. Sampling design and selection of study populations seriously impact the conclusion of studies, and convenience samples can provide estimates that may not reflect reality. Results based on data from the Third National Health and Nutrition Examination Survey (NHANES III), analyzed with appropriate nesting and weighting statements to adjust the variance for the complex sampling design of the survey, can be generalized to the United States population. Such a study found a substantially lower prevalence of RAS (1.03% overall), which, when stratified by age, suggests a 0.85% prevalence among adults and 1.5% prevalence among children and adolescents.
This population-based study in the United States found that overall the prevalence of recurrent aphthous ulcers was 1030 per 100,000 persons (95% CI, 830–1220). The prevalence of RAS among children was 1500 per 100,000 (95% CI, 1090–1910), which was greater than that among adults, at 850 per 100,000 (95% CI, 630–1070). It is estimated that in the United States, at least 3 million people have RAS, of which approximately 2 million are aged 17 years or older and 1 million are younger than 17 years.
Multivariable analyses to determine independent risk indicators and risk factors in adults suggested that adjusted odds of RAS were greatest for persons aged 17 to 29 years (adjusted odds ratio [OR], 2.7; 95% CI, 1.4–5.5), men (adjusted OR, 1.7; 95% CI, 0.9–2.8), and persons with low serum insulin levels (OR, 2.0; 95% CI, 0.9–4.4). Never-smokers had greater risk for recurrent aphthous ulcers (OR, 9.2; 95% CI, 2.8–30.1) than people who smoked more than 10 cigarettes per day. Results from a separate analysis based on NHANES III data show RAS-associated age distribution and sex differences ( Figs. 1 and 2 ).
Associations and etiology
Box 1 lists various causative and predictive factors suggested to be associated with RAS, none of which has been proven conclusively to be independently associated with RAS.
Trauma
Variety of physical and chemical trauma
Foods and nutrients
Chocolates
Dairy products
Nuts
Tomatoes
Wheat
Deficiency
Vitamins B 1 , B 2 , and B 6
Folate
Zinc
Iron
Chemokines, biological body products
TNF-α
Interleukins
Heat shock proteins
Systemic conditions
Endocrinologic
Menstruation
Low insulin levels
Gastroenterologic
Crohn’s disease
Malabsorption syndrome
Celiac disease
Ulcerative colitis
Gluten enteropathy
Hematologic
Anemia
Cyclical neutropenia
Hematologic malignancies
Immunologic
Immunodeficiencies (T-cell responses and defects, HIV)
Microbiologic
Streptococci
M tuberculosis
H pylori
Herpes viruses
Varicella zoster
Cytomegalovirus
Multiorgan diseases
Behçet’s disease
MAGIC (mouth and genital ulcers with inflamed cartilage) syndrome
Marshall’s syndrome
Reactive arthritis
Erythema multiforme
Genetic
HLA B51
Others
Keratinocyte maturity deficiency
Defective mucosal epithelial turnover
Behavioral factors
Smoking
Oral contraceptives
Psychological
Physiologic stress
Medications
Nonsteroidal anti-inflammatory drugs
β-blockers
Nicorandil
Alendronate
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


