Oral lichen planus (OLP) is a chronic, immune-mediated condition commonly affecting middle-aged women. The cause of OLP remains obscure. Strict clinical and histologic criteria need to be met to arrive at a definite diagnosis, thereby ruling out other conditions that may mimic OLP clinically and/or histologically. Although OLP is considered a premalignant condition, the risk for neoplastic change seems low.
Lichen planus (LP) is derived from the Greek leichen meaning tree moss and the Latin planus meaning flat. Erasmus Wilson first described LP in 1869, as a chronic disease affecting the skin, scalp, nails, and mucosa, with possible rare malignant degeneration. Francois Henri Hallopeau reported the first oral lichen planus (OLP)–related carcinoma in 1910.
The true cause of LP remains obscure. Treatment is generally geared to alleviating symptoms. Cutaneous lesions of LP are self-limiting and pruritic; however, oral lesions are chronic, rarely remissive, and are frequently the source of morbidity. Cutaneous lesions are characteristically erythematous to violaceous, flat-topped, pruritic, polygonal papules with the surface showing a network of fine lines (Wickham striae) affecting the flexor surfaces of arms, wrists, ankles, and genitalia. Apart from cutaneous LP in patients with OLP, there is a high prevalence of other skin diseases such as eczema and psoriasis in patients with OLP.
OLP constitutes 9% of all white lesions affecting the oral cavity. Most patients with OLP have no associated cutaneous LP or LP at any other mucosal site, so the process is often referred to as isolated OLP. Less often, a subset of patients can have simultaneous involvement of the oral mucosa and cutaneous or other mucosal sites, such as in the vulvovaginal-gingival syndrome, or penogingival syndrome. Genital LP is associated with approximately 20% of OLP, whereas cutaneous LP is associated with approximately 15% of OLP. However, some studies suggest that the association between cutaneous LP and OLP is closer to 70% to 77%. OLP has been well documented in patients with esophageal LP.
The diagnosis of OLP is made based on a strict combination of clinical criteria as well as histopathologic evaluation.
Frequency
LP has a varied prevalence based on different geographic regions, but it generally affects approximately 1% to 2% of the world’s population. Many large-scale studies of OLP have been conducted in India. The prevalence of OLP ranges between 0.5% and 3% and may occur in 70% to 77% of patients with cutaneous LP. However, some studies report that isolated OLP (without cutaneous involvement) occurs more commonly.
Age
Typically, LP affects individuals between the ages of 30 and 60 years. It is rare in children, with the youngest case documented in a child aged 3 months. Of the cases of OLP reported in children, there is a higher prevalence in the Indian population, suggesting probable differences in the genetic background and/or environmental triggers.
Causes
Numerous reports have tried to clarify the role viruses may play in the development of OLP, including Varicella zoster virus, Epstein-Barr virus, cytomegalovirus, human herpes virus, human papilloma virus, and hepatitis C virus (HCV). The association between OLP and liver disease has been investigated since 1978. The pathogenic role of HCV in the development of OLP is still undecided. It is believed that the immune reaction mediated by HCV replication may cause damage to the basal layer cells and result in OLP lesions, resulting in an extrahepatic manifestation of HCV. Some studies suggest that the hepatitis C virus exerts an indirect effect, possibly mediated by the modulation of cytokines and lymphokines in the pathogenesis of oral erosive LP. In a recent review and meta-analysis, it was concluded that patients with LP have a higher risk of being HCV seropositive and, similarly, HCV-infected patients had a higher probability of developing LP.
Although controversial, psychological disorders and stress are believed to represent possible causal factors in OLP. A few investigators have found that patients with OLP have significantly higher stress, anxiety, and depression levels compared with healthy individuals.
Pathophysiology
Although many possible causes explaining the pathogenesis of LP have been proposed, the exact cause remains unclear. OLP is classified as an inflammatory disease of the stratified squamous epithelium, and it is still unclear what antigen, whether endogenous or exogenous in origin, triggers the inflammatory immune response in OLP lesions.
Most data suggest that OLP is a CD8+ T cell–mediated autoimmune disease. However, the triggering factors and pathogenic mechanism are still not conclusively identified. There seems to be no definite role of B cells, plasma cells, immunoglobulins, or complements in the mediation of LP. In a study comparing the T cell clone response of lesional LP and normal mucosa, the T cell lines in patients with LP were significantly more cytotoxic and were identified as CD8+. These CD8+ T cells are believed to induce keratinocyte apoptosis and cause epithelial basal cell layer damage via several possible suggested mechanisms: (1) secretion of tumor necrosis factor-α (TNF-α), which binds the TNF-α receptor 1 on the keratinocyte surface; (2) the binding of CD95 (Fas) on the keratinocyte surface with CD95L, which is expressed on the T cell surface; and (3) entry and assimilation of granzyme B secreted by T cells into the keratinocytes by perforin-induced membrane pores. A variety of factors are believed to trigger the cytotoxicity of CD8+ T cells. One is the expression of major histocompatibility complex class (MHC) II presented by the langerhans cells and keratinocytes, which secrete interleukin-12 (IL-12) thus activating the CD4+ T cells. This activation of CD4+ T cells and subsequent expression of interleukin-2 (IL-2) and interferon-γ (INF-γ), in association with the MHC class I, which are associated with basal keratinocytes, promotes cytotoxic CD8+ T cell induction of keratinocytes apoptosis. The immunologic abnormality leads to a delay in the growth of mucosal epithelium that is responsible for hyperkeratosis.
Polymorphisms and genetic variations in the expression of cytokines have been linked with the risk of developing lesions of OLP and governs whether lesions are limited to the oral cavity (INF-γ), or skin (TNF-α).
Another nonspecific mechanism in the development of LP is believed to be the degranulation of mastocytes and a posterior activation of matrix metalloproteinases, which degrades components of the extracellular matrix and basal membrane and also participates in the migration of lymphocytes through the epithelium. OLP lesions have more than 60% of degranulated mastocytes in comparison with normal mucosa.
Genetics, familial clustering, and human leukocyte antigen association, although initially implicated to play a role in the pathogenesis of OLP, are no longer considered critical factors.
Clinical findings
LP may affect the hair follicles, nails, esophagus, and, less frequently, the eyes, urinary tract, genitals, nasal mucosa, and larynx. Scalp involvement causes pruritic, follicular and perifollicular, scaly, violaceous papules, referred to as lichen planopilaris, and can also lead to permanent patchy hair loss. When LP affects nails, it causes pitting, subungual hyperkeratosis, permanent nail loss, and so forth.
The clinical presentation orally is nearly always in a bilateral, symmetric pattern. The buccal mucosa (bilaterally) is the most typical site of involvement, but other panoral mucosal sites and the lips can also be involved. After the buccal mucosa and tongue, the gingiva seems to be commonly involved. If only the erosive subtype of OLP affects the gingival tissue, the descriptive clinical term desquamative gingivitis (DG) is often used. OLP is confined to the gingiva in about 10% of patients. Lesions of OLP affecting the palate, floor of the mouth, and upper lip are not common.
Most patients with OLP show no increased prevalence of cigarette smoking or alcohol consumption. Although OLP patients do not seem to have an increased risk of diabetes, diabetics who develop OLP have an increased frequency of atrophic-erosive lesions, especially affecting the tongue. A correlation between OLP and hypertension has also been proposed. An association between OLP, diabetes mellitus, and hypertension has been described, the triad being termed the Grinspan syndrome.
Clinical features
To better define the criteria for diagnosis of OLP, the World Health Organization (WHO) devised a set of clinicopathologic criteria in 1978 ( Box 1 ). Because these criteria lacked consensus regarding a clinical and histologic diagnosis of OLP, modifications were proposed to the WHO criteria in 2003 ( Box 2 ), which resulted in a substantial increase in consensus and clinicopathologic correlation. In addition, knowledge about history of systemic diseases, history of drug use, and cutaneous lesions can be helpful in arriving at a definite diagnosis.
Clinical criteria
- •
Presence of white papule, reticular, annular, plaque-type lesions, gray-white lines radiating from the papules
- •
Presence of lacelike network of slightly raised gray-white lines (reticular pattern)
- •
Presence of atrophic lesions with or without erosion, and possibly also bullae
- •
Histopathologic criteria
- •
Presence of thickened ortho- or parakeratinized layer in sites that are normally keratinized, and, if site is normally nonkeratinized, this layer may be thin
- •
Presence of Civatte bodies in basal layer, epithelium, and superficial part of connective tissue
- •
Presence of a well-defined bandlike zone of cellular infiltration that is confined to the superficial part of the connective tissue, consisting mainly of lymphocytes
- •
Signs of liquefaction degeneration in the basal cell layer
- •
Clinical criteria
- •
Presence of bilateral, more or less symmetric lesions
- •
Presence of a lacelike network of slightly raised gray-white lines (reticular pattern)
- •
Erosive, atrophic, bullous, and plaque-type lesions are only accepted as a subtype in the presence of reticular lesions elsewhere in the oral mucosa
- •
In all other lesions that resemble OLP but do not complete the aforementioned criteria, the term “clinically compatible with” should be used.
Histopathologic criteria
- •
Presence of a well-defined, bandlike zone of cellular infiltration that is confined to the superficial part of the connective tissue, consisting mainly of lymphocytes
- •
Signs of liquefaction degeneration in the basal cell layer
- •
Absence of epithelial dysplasia
- •
When the histopathologic features are less obvious, the term “histopathologically compatible with” should be used.
Final diagnosis of OLP or oral lichenoid lesions (OLL)
To achieve a final diagnosis, clinical as well as histopathologic criteria should be included
OLP
A diagnosis of OLP requires fulfillment of clinical and histopathologic criteria
OLL
The term OLL will be used in the following conditions:
- 1.
Clinically typical of OLP but histopathologically only compatible with OLP
- 2.
Histopathologically typical of OLP but clinically only compatible with OLP
- 3.
Clinically compatible with OLP and histopathologically compatible with OLP
- 1.
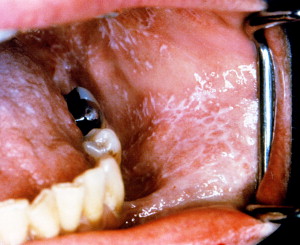
The oral manifestations of OLP have been described in many large studies. Clinically, there are 6 clinical subtypes of OLP that can be seen individually or in combination: papular, reticular, plaquelike, atrophic, erosive, and bullous. The most common of these are the reticular, erosive, and plaquelike subtypes, and these variants can coexist within the same patient. Mucosal lesions are usually bilateral and involve multiple sites within the oral cavity. The most common presentation is that of pinpoint white papules that gradually enlarge and come together to form the reticular or plaquelike pattern. In the absence of the classic reticular pattern on oral mucosal surfaces, which appears as multiple papules with a network of small, raised, whitish-gray, lacy lesions referred to as Wickham striae ( Fig. 1 ), it is challenging to clinically diagnose nonreticular types. Histologic confirmation of the diagnosis is thus required.
The erosive form of OLP may present with erythema caused by inflammation or epithelial thinning, or both, and ulceration/pseudomembrane formation with periphery of the lesion surrounded by reticular keratotic striae ( Figs. 2 and 3 ). Gingival lesions frequently present with erythema and ulceration affecting the marginal and attached gingiva, as a manifestation of erosive LP ( Fig. 4 ). The plaque form of OLP mimics leukoplakia in that it appears as a white, homogeneous, slightly elevated, multifocal, smooth lesion ( Fig. 5 ). The plaque form of OLP commonly affects the dorsum of the tongue and buccal mucosa. Bullous LP may present with bullae ranging from a few millimeters to a few centimeters in diameter. Typically, bullae ulcerate and become covered by whitish pseudomembrane. Bullous LP is uncommon in the oral cavity, as is the papular type of OLP.



Lichenoid reactions (OLL/oral lichenoid reactions [OLR]) have similar features, clinically and histologically, to LP, but have a less characteristic morphology or have a distinct cause, unlike OLP ( Fig. 6 ). OLL therefore needs to be distinguished because treatment modalities are different from those for OLP.
Symptoms and signs
Symptoms and signs can range from patients being unaware of the disease, with lesions that are completely asymptomatic as in reticular OLP, to those experiencing mucosal sensitivity and burning and debilitating pain. Approximately two-thirds of the patients affected with OLP experience oral discomfort. Because OLP has periods of relapses and remissions, during a period of exacerbation there may be an increase in symptoms and clinical signs. During periods of quiescence, symptoms and signs of OLP are diminished. Factors such as stress may aggravate the clinical presentation of the disease. Precipitating factors similar to the Koebner phenomenon, which is characteristic of cutaneous LP whereby lesions develop in response to trauma, can also affect the oral cavity. Sharp cusps and ill-fitting dental prosthesis may be the triggers. Chronic accumulation of plaque and calculus can also exacerbate OLP, perhaps because of the Koebner phenomenon. Gingival OLP can eventually lead to gingival recession, advanced periodontal disease, and so forth, and therapeutic periodontal procedures may aggravate these conditions. An association between OLP and xerostomia has been established.
Histologic findings
The histologic features of OLP were first described by Dubreuill in 1906 and later revised by Shklar in 1972. The WHO developed a set of histopathological criteria for OLP in 1978, which was most recently modified in 2003 (see Box 2 ).
Definite diagnostic histologic findings include liquefactive degeneration of the basal cells, colloid bodies (Civatte, hyaline, cytoid), homogeneous infiltrate of lymphocytes in a dense, bandlike pattern along the epithelium-connective tissue interface in the superficial dermis, cytologically normal maturation of the epithelium, sawtooth rete ridges, and hyperkeratosis (orthokeratosis or parakeratosis) ( Fig. 7 ). In addition, the surface epithelium may show signs of ulceration, typically seen in erosive LP. If the erosive component is severe, bullae may form in the area of the epithelial separation, which eventually ulcerate ( Fig. 8 ). Several histologic criteria that are considered as exclusionary in diagnosing OLP include the absence of basal cell liquefaction degeneration, polyclonal inflammatory infiltrate, abnormal cytology suggestive of dysplasia, abnormal keratinization, flat rete ridges, and absence of colloid bodies.



