Purpose
To compare the optical quality of implantable Collamer lens (ICL) with and without central hole (Hole ICL and conventional ICL) at different degrees of decentering.
Design
Experimental laboratory investigation.
Methods
Wavefront aberrations of the −3, −6, and −12 diopter (D) V4b and −3, −6, and −12 D V4c ICLs were measured in 3 conditions—centered and decentered 0.3 and 0.6 mm—at 3-mm and 4.5-mm pupils. The root mean square of total higher order aberrations, trefoil, coma, tetrafoil, secondary astigmatism, and spherical aberration were evaluated. In addition, point spread function and simulated retinal images of ICLs were calculated from the wavefront aberrations for each ICL and all conditions of decentering at 4.5-mm pupil.
Results
No statistically significant differences in any Zernike coefficient terms evaluated were found between conventional and Hole ICLs for any ICL powers and pupils evaluated ( P > .05). We could not appreciate differences in the point spread function images and in simulated retinal images. Regarding the effect of the ICL decentration, coma aberration increased significantly with ICL decentration ( P < .05), although these differences were not visible in the point spread function images and simulated retinal images. The ICL decentration was affected in the same manner on the conventional and Hole ICLs.
Conclusions
The outcomes showed good and comparable optical quality of the conventional and Hole ICLs for all ICL powers evaluated. Despite that coma aberration increased with ICL decentering, these values were clinically negligible and did not have a significant effect on the simulated visual performance.
Phakic intraocular lens implantation is becoming more popular to correct high and moderate refractive errors. This popularity is attributable to the fact that phakic intraocular lens implantation leaves the central cornea untouched, inducing less higher-order aberration and showing better optical and visual quality than corneal refractive treatments; in addition, it is a reversible surgery. The implantable Collamer lens (ICL; STAAR Surgical, Nidau, Switzerland) is a posterior phakic intraocular lens implantation approved by the US Food and Drug Administration (FDA) for myopia correction. Several studies have shown the safety and effectiveness of the ICL for correction of myopia, hyperopia, and astigmatism.
However, cataract development has been noted after ICL implantation. The majority of reported complications after ICL implantation are cataract formation, and FDA studies have reported that the incidence of secondary cataract was 2.1% within 1 year and 2.7% within 3 years after surgery. This complication likely results from direct physical contact between the ICL and the crystalline lens or from localized malnutrition causing poor circulation of the aqueous humor. Therefore, Fujisawa and associates created a 3-mm central perforation in the ICL to improve the aqueous humor circulation, reducing the incidence of cataract formation in porcine eyes. Shiratani and associates showed that an ICL with a hole 1.0 mm in diameter in the center of the optic had no optical effect on vision and was sufficient to increase the aqueous humor perfusion volume on the anterior surface of the crystalline lens, preventing cataract formation. Uozato and associates measured in vitro the modulation transfer functions of conventional ICLs and ICLs with central hole of 0.36 mm for various powers and pupil diameters. They reported that the differences between ICLs with and without hole were small and clinically negligible.
Two peer studies evaluated the visual performance with the Hole ICL implanted; both studies agree that the Hole ICL showed good results of safety, efficacy, predictability, and stability for the correction of high to moderate myopic errors and the Hole ICL appears to be equivalent in the induction of higher-order aberrations and contrast sensitivity function to conventional ICL implantation. In addition, Hole ICL does not require additional peripheral iridotomies and may also reduce the risk of cataract formation.
In addition, the effect of decentration was also considered to evaluate how it influences higher-order aberrations and its effect on the optical quality of these lenses.
The aim of the present study was to compare accurately the optical quality in vitro of the conventional ICL and Hole ICL for 3 powers (−3, −6, and −12 diopters [D]) and to evaluate the effect of decentering (0.3 and 0.6 mm) at 3-mm and 4.5-mm pupils. The point spread functions (PSFs) and simulated retinal images, which are related to the visual performance of the patient implanted with these lenses, were computed from wavefront aberrations for each ICL and all conditions of decentering at 4.5-mm pupil.
Methods
This experimental laboratory investigation was approved by the Institutional Review Board at the University of Valencia Research Group of Optometry. The Visian ICL (STAAR Surgical, Nidau, Switzerland) is a phakic lens made from Collamer, a flexible, hydrophilic, and biocompatible material with a plate-haptic design and a central convex/concave optical zone. The ICL lenses are foldable, allowing for posterior chamber injection through a microscopic incision of 3.5 mm or smaller. When properly placed, the ICL should be positioned completely within the posterior chamber between the iris and crystalline lens with support on the ciliary sulcus. In this study we have analyzed the V4b and V4c models for different powers: −3, −6, and −12 D for both models. The V4c model ICL introduces a central hole (diameter 0.36 mm) to increase the aqueous humor perfusion and reduce the risk of secondary cataract formation. The length of the ICLs was 12 mm and the optical diameter was 5.5 mm in all cases.
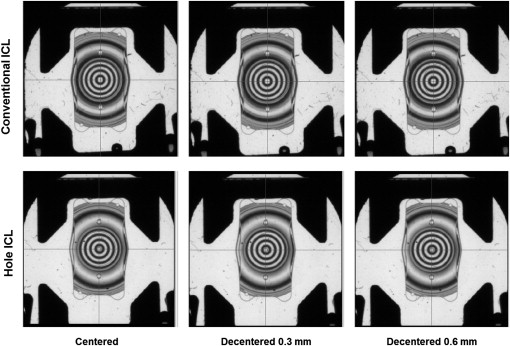
The NIMO TR0805 instrument (Lambda-X, Nivelles, Belgium) was used to analyze and measure wavefront aberrations of the lenses. The working principle of the NIMO instrument is based on a phase-shifting schlieren technique. The principle of schlieren imaging has been known for some time and is commonly used to visualize variations in density for gas flows. By combining this principle with a phase-shifting method, the NIMO instrument allows the measurement of light beam deviations, which can be used to calculate the power characteristics of the lenses and the wavefront analysis considering 36 Zernike coefficients. This technology has been shown to effectively measure in vitro the optical quality of the ICL. In this study, we measured 3 conventional ICLs and 3 Hole ICLs with the following refractive powers: −3, −6, and −12 D. In addition, we evaluated these lenses in 3 positions: centered, decentered 0.3 mm, and decentered 0.6 mm ( Figure 1 ). Zernike coefficient values were retained as the average of 10 measurements. We analyzed the root mean square of total higher-order aberrations (third to seventh order), trefoil (Z 3 −3 ; Z 3 3 ), coma (Z 3 −1 ; Z 3 1 ), tetrafoil (Z 4 −4 ; Z 4 4 ), secondary astigmatism (Z 4 −2 ; Z 4 2 ), and spherical aberration (Z 4 0 ) at 3-mm and 4.5-mm pupils.
Data Analysis
The analysis of variance (ANOVA) was used to disclose differences between both ICL models and different conditions of decentering. Post hoc multiple comparison testing was performed using the Holm-Sidak method. Differences were considered statistically significant when the P value was less than .05.
Results
Figures 2 and 3 show bar graphs of the root mean square of trefoil (Z 3 −3 , Z 3 3 ), coma (Z 3 −1 , Z 3 1 ), tetrafoil (Z 4 −4 , Z 4 4 ), secondary astigmatism (Z 4 −2 , Z 4 2 ), and spherical aberration (Z 4 0 ) for both conventional and Hole ICLs and all conditions at 3-mm and 4.5-mm pupils, respectively. All ICLs evaluated had negative values of spherical aberration, which increases with the ICL power. We did not find statistically significant differences at any Zernike coefficient root mean square values evaluated between conventional and Hole ICLs at any ICL powers and for both pupils ( P > .05). Regarding the effect of decentering, we only found statistically significant differences in coma aberration between the centered position and both degrees of decentering for all ICLs and pupils evaluated ( P < .05). Coma aberration increased with ICL decentration; this increment was greater for higher ICL powers and pupil sizes. No statistically significant differences were found in other Zernike coefficient root mean square values evaluated between centered and decentered positions for any ICLs and pupils evaluated ( P > .05).
Figure 4 shows bar graphs of total root mean square for each ICL evaluated and all conditions at 3-mm and 4.5-mm pupil. No statistically significant differences were found between conventional and Hole ICLs at any refractive power and pupil diameter ( P < .05). In relation to the effect of decentering on both types of ICLs, for a 3-mm pupil, we found statistically significant differences only between centered and 0.6 mm of decentering for −12 D ( P < .05). At 4.5-mm pupil, statistically significant differences were found between centered position and 0.6 mm decentering for all ICLs evaluated ( P < .05).
Figure 5 shows the images of PSFs computed from the wavefront aberrations of the ICLs evaluated and for different degrees of decentering at 4.5-mm pupil. The differences between these images were minimal; a slightly greater spread-out can be observed at conventional and Hole −12 D ICLs in relation to lower-power ICLs because of the effect of spherical aberration increment with the refractive power. The corresponding simulated retinal images are shown in Figure 6 ; as expected, they did not show differences between conventional and Hole ICLs for any refractive power and position.



