Optic Nerve Sheath Meningiomas
Syndee J. Givre
Jonathan J. Dutton
Introduction
Meningiomas are the second most common brain neoplasms after gliomas. They are benign lesions arising from meningothelial cells of the meninges, representing 15% to 20% of all intracranial tumors in adults and 2% of intracranial tumors in children. About 90% of meningiomas occurring in the orbit are extensions from intracranial sites, most commonly the sphenoid wing.1 However, primary lesions arising within the orbit are well documented. Regardless of the site of origin, meningiomas may have considerable effect on visual function.
Primary Optic Nerve Sheath Meningiomas
Primary orbital meningiomas, mostly originating in the optic nerve sheath, represent 1% to 2% of all meningiomas. They are the most common tumor of the optic nerve sheath and represent the second most common primary optic nerve tumor after optic nerve gliomas. This entity was first described by Antonio Scarpa in 1816,2 but many early cases probably also included optic nerve gliomas until these two lesions were clearly distinguished by Hudson in 1912.3 Meningiomas primarily affect middle-age adults with a slight female predominance. Patients typically present with visual loss, frequently associated with proptosis, optic atrophy, and often with optociliary shunt vessels.4,5,6,7 The lesion is usually unilateral, but rarely can be bilateral. Meningiomas characteristically show indolent growth over many years, progressing inexorably to profound visual loss in the affected eye. The diagnosis is usually suspected from the clinical findings and from neuroimaging, making tissue biopsy unnecessary in most cases.8 However, in difficult cases it has been shown that a shave biopsy of the optic nerve, sparing the central macular fibers, can provide diagnostic tissue without visual or visual field compromise.9 Previously management has usually been conservative, but during the past decade newer treatment options, such as radiotherapy, have significantly improved visual prognosis. Even when untreated, the prognosis for life is excellent, with an overall tumor-related mortality of 0%.
Demographic Characteristics
Age at Presentation
Despite several early reports of orbital meningiomas occurring with high frequency in young individuals, later series confirm that this is a disease primarily of middle age. On imaging studies meningiomas may be confused with arachnoid proliferation associated with optic gliomas in young patients, and this may account for some confusion when the diagnosis is based on radiologic evaluation. The mean age for presentation of optic sheath meningiomas is 41 years, with a range of 2.5 years to 80 years (Table 38.1). Only 4% of reported patients are under 20 years of age. The onset of symptoms for bilateral cases appears to be significantly younger, with a mean age of 13 years, but involvement of the second eye may be delayed for up to several decades.4
TABLE 38.1 Demographics of Primary Orbital Meningiomas | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Sex Distribution
It has long been recognized that meningiomas occur more frequently in females. However, when large series of reported patients are examined the ratio tends to equalize, but still there does appear to be a slight female predominance of approximately 60%.
Laterality
A predilection for the right optic nerve has been reported in several studies, but others have not confirmed these findings. However, when larger series are examined, 52% of sheath meningiomas occur in the right optic nerve, 42% occur in the left, and 6% are bilateral. Interestingly, among bilateral cases, 60% are canalicular meningiomas, compared to all sheath meningiomas together where canalicular tumors account for only 8%.
Sites of Origin
Approximately 10% of all optic nerve sheath meningiomas arise within the orbit, and of these, the vast majority (96%) derive from the retrobulbar optic nerve sheath (Table 38.2). Growth usually diffusely thickens the optic nerve sheath, but sometimes tumor can rupture through the dura forming an exophytic growth pattern. Intracranial extension is seen more commonly with tumors that have a posterior orbital component and in younger patients.6 Although most meningiomas are unilateral, a small percentage may be bilateral, involving both optic nerves. Some bilateral tumors may represent extensions across the planum sphenoidale,10 whereas others appear to have arisen multifocally.11 Among these canalicular tumors there is a significant propensity toward bilaterality, with 65% being unilateral and 35% being bilateral. This compares with only 6% bilaterality for all sheath meningiomas taken together. This raises the question of possible undetected intracranial contiguity of tumor for at least some of these, perhaps extending from an intracranial site.
TABLE 38.2 Sites of Origin for Orbital Meningiomas | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
In 8% of cases the meningioma may be confined to the optic canal, often making diagnosis more difficult.12 Because of the confines of the bony canal, visual symptoms occur early and imaging studies are often negative initially. Canalicular meningiomas may represent lesions arising from the optic nerve sheath, or from periforaminal meningiomas originating in the region of the anterior clinoids, tuberculum sellae, or planum sphenoidale.
In 4% of optic sheath meningiomas, tumor may enter the globe along penetrating vascular channels resulting in focal invasion of the optic disk, sclera, choroid, or retina. Meningioma cells have even been demonstrated within the vascular lumina of ciliary arteries and the central retinal vessels.
About 4% of primary orbital meningiomas appear to arise ectopic to the optic nerve sheath, and within the orbital soft tissue.4,10 The exact etiology of such lesions remains uncertain, but it has been suggested that such lesions may arise from arachnoid clusters within the orbit, from meningeal tissue along orbital nerves, or from arachnoid tufts that may grow through the dura of the optic nerve. Shuangshoti13 suggested that they could arise directly from orbital mesenchymal cells. It is also possible that in some cases they represent other lesions mistaken for meningiomas such as fibroxanthomas, hemangiopericytomas, or fibrous histiocytomas.14,15
Association With Neurofibromatosis
The incidence of neurofibromatosis (NF) among patients with optic nerve sheath meningioma is unclear because most studies in the past failed to mention the occurrence of this association. Of the studies that specifically examined for NF, 9% of patients with sheath meningioma are so affected.4 This is considerably lower than the 29% association with optic nerve gliomas, but still significantly higher than the 0.3% to 0.5% incidence of NF in the general population. In a recent survey of 30 consecutive patients with NF followed for a mean of 8 years, 26.7% presented with or later developed symptoms and radiographic findings consistent with optic nerve meningioma.16 Therefore, it is important for physicians to be aware of this relationship.
Clinical Signs and Symptoms
The triad of clinical findings consisting of visual loss, optic atrophy, and optociliary shunt vessels has been considered as nearly pathognomonic for optic nerve sheath meningiomas.17 Although this combination remains strongly suggestive of the diagnosis, nevertheless, the simultaneous occurrence of all three findings in any one individual with a sheath meningioma is uncommon. This triad has also been shown to be a relatively nonspecific finding in cases of optic nerve compression from other causes.18 Orbital pain is very uncommon, even with large tumors.
Visual Acuity
The most frequent presenting symptom of optic sheath meningioma is loss of vision, seen in 96% of cases. Visual loss is typically indolent, often progressing to blindness over many years, but in some cases vision will remain stable for long periods of time.19,20,21 Transient obscurations may be the initial symptom, and in more than 25% of cases visual disturbance may be gaze-evoked or postural in nature. In about 45% of cases visual acuity is relatively good on presentation, in the range of 20/20 to 20/40, and in 25% it is counting fingers or worse.4 In bilateral cases, visual loss typically begins in one eye, and involvement of the second eye may be separated in time by 2 to 30 years. In the absence of radiographic confirmation of an optic nerve mass, symptoms may simulate chronic optic neuritis.22,23 A case has recently been reported of sudden unilateral visual loss during pregnancy which proved to be from a sheath meningioma. It was suggested that pregnancy might accelerate the growth of meningiomas.24
Visual Fields
Visual field defects can be demonstrated in most patients with visual loss. Most commonly these include peripheral constriction or central, centrocecal, and paracentral scotomas. Less frequently altitudinal defects or increased size of the blind spot may be seen. The incidence of generalized constriction appears to be higher with canalicular lesions.25
Proptosis
Proptosis is found on initial examination in 60% of patients. It usually follows the onset of visual loss, but in some cases it may be the initial symptom. Generally, proptosis is relatively mild, in the range of 2 to 5 mm, although in advanced cases it can exceed 10 mm (Fig. 38.1). It is seen less frequently in patients with canalicular lesions, because they typically have significant visual loss while the tumor is still very small.
 FIGURE 38.1 Clinical appearance of a patient presenting with visual loss and proptosis from an optic nerve sheath meningioma. |
Ocular Motility
Limitation of ocular motility is variable but may be seen in nearly half of patients at the time of initial presentation. Upgaze is commonly severely impaired, possibly because of stiffening of the optic nerve from the relatively firm tumor.26 In some cases cranial nerve palsy may be responsible.
Intraocular Findings
Chronic disk edema is an early finding in 48% of patients (see Table 38.3). It is seen less frequently with tumors confined to the optic canal. Optic atrophy, which can be subtle, may be a somewhat later finding, and its occurrence increases with the duration of optic nerve compression. At presentation, optic atrophy is found in nearly half of reported cases. Both edema and atrophy sometimes may be seen together. Overall, 98% of patients will show one or the other of these two findings.
TABLE 38.3 Diagnostic Clinical Findings of Optic Nerve Sheath Meningioma | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
The association between optic sheath meningiomas and optociliary shunt vessels has long been considered a key finding suggestive of this diagnosis. These represent collateral vessels from the retinal to the choroidal venous circulation resulting from compression of the central retinal vein, with dilation of vestigial retinociliary anastomoses that re-establish embryonic flow to the vortex veins (Fig. 38.2). However, chronic disk edema and congestion of the central retinal vein often precede the first appearance of shunts by several years, and the shunts usually disappear as optic atrophy becomes complete. Thus, optociliary shunt vessels are relatively infrequent with sheath meningiomas, seen in only 30% of reported cases. Because shunts tend to appear some years after symptoms begin and involute as optic atrophy is complete, this probably does not indicate their true incidence during the course of the disease. Indocyanine green videoangiography has been shown to be superior to fluorescein angiography in demonstrating these vessels,27 and in some cases they may just be missed on standard fluorescein angiography studies. Optociliary shunt vessels are also seen in other conditions such as retinal vein occlusion, chronic glaucoma, optic disk drusen, high myopia, and diabetes mellitus; and rarely as a congenital anomaly.28,29
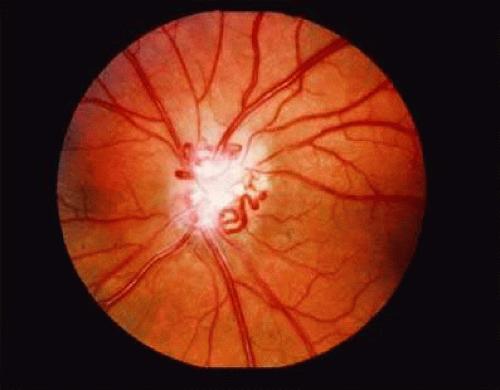 FIGURE 38.2 Fundus photograph showing an optic nerve sheath meningioma with disk pallor and optociliary shunt vessels. |
Histopathology
Meningiomas arise from meningothelial cells found at specific locations along the meninges. Large collections of these cells project into the intracranial dural sinuses and veins, and smaller collections (called arachnoid villi) are located along the sphenoid ridge, planum sphenoidale, tuberculum sellae, olfactory groove, and the canalicular and orbital optic nerves. Optic sheath meningiomas are believed to originate from meningothelial cap cells of the arachnoid villi that lie along the intraorbital optic nerve. They may arise at multiple sites simultaneously.
Two histologic patterns are seen, but optic sheath lesions are usually of the meningothelial type (Fig. 38.3). Here we find distinctive small nodules of tumor cells having a whorled pattern resulting from the cells wrapping around their more central neighbors.32 Spindle cells have round to oval nuclei, inapparent nucleoli, moderate amounts of eosinophilic cytoplasm, and indistinct cell borders. Intranuclear vacuoles are characteristic features of the neoplastic cells. Psammoma bodies are basophilic laminated concretions that develop from hyalinization and deposition of calcium salts in the center of whorls, and they are responsible for the calcifications noted on radiologic studies. In the transitional pattern, spindle-shaped or oval cells are arranged in a concentric whorl formation. Rarely, they may be associated with large cyst formation that can confuse the radiologic diagnosis.33,34,35 They can also result from a sheath compartment syndrome with an elevated concentration gradient accumulation of albumin, IgG, and beta-trace protein.36
 FIGURE 38.3 Histopathology of an optic nerve sheath meningioma showing spindle cells arranged in a concentric whorl formation (original magnification ×25). |
Meningiomas are neoplasms that spread within the subarachnoid space. Although they are not truly encapsulated, the overlying intact arachnoid and dura serve as a functional capsule. These tumors may invade the optic nerve along its septae or extend into the spaces surrounding the central retinal vessels.37 Tumor cells may also rupture through the dura and into surrounding orbital tissues as an exophytic growth.38 When adjacent to bone, tumor can extend into the haversian canal system inciting hyperostosis and bone proliferation, resulting in the thickened bone seen with secondary and some primary meningiomas. Although primary optic nerve sheath meningiomas can extend along the intracranial optic nerve to the chiasm, they do not invade the brain, nor do they cause increased intracranial pressure or hypothalamic dysfunction.25 Even when left untreated they do not cause any neurologic deficit other than vision loss.19
Diagnosis
Individual clinical signs and symptoms and imaging characteristics of optic nerve sheath meningiomas may be mimicked by other entities. Therefore the diagnosis relies on the presence of a combination of suggestive features. However, even without pathologic confirmation, the diagnosis of optic nerve sheath meningioma is not difficult to make in the large majority of cases.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


