Ophthalmic and Systemic Manifestations of Child Abuse
J. Peter Campbell
Mary Louise Z. Collins
Alex V. Levin
The World Health Organization defines child maltreatment as “all forms of physical and/or emotional ill-treatment, sexual abuse, neglect or negligent treatment or commercial or other exploitation, resulting in actual or potential harm to the child’s health, survival, development or dignity in the context of a relationship of responsibility, trust or power.”1 Although child abuse has been present since ancient times, its recognition as a major cause of morbidity and mortality in the pediatric age group is a recent phenomenon.2,3,4,5 The physical and emotional impact on victims is enormous. Victims have an increased risk of psychiatric disorders, suicide, alcohol abuse, smoking, and the subsequent health risks associated with poor lifestyle choices.6 Economic costs are difficult to calculate, taking into account direct and indirect costs of abuse, but are estimated to be greater than 12 billion dollars per year in the United States alone.1
The epidemiology of child abuse is difficult to establish due to underreporting but is thought to be affected by income level and region of the world.7,8 In the United States in 2007, there were 3.2 million referrals to child protective service (CPS) agencies involving 5.8 million children.6 Twenty-four percent of those reports were substantiated. Fifty-seven percent of the reports were made by “professionals,” medical or otherwise. The U.S. Department of Health and Human Services estimates that in 2007, 794,000 children were victims of maltreatment, 25% of whom had been “in the system” prior to the incident event. Children younger than 1 year old had the highest rate (21.9 per 1,000) of abuse. Of the reported cases of abuse, 59% fell into the category of neglect, 18% physical abuse, 7.6% sexual abuse, and 4.2% emotional abuse.6
An estimated 3,500 children younger than 15 years of age die each year in the industrialized world due to abuse and neglect.7 In 2007, 1,760 children were known to have died due to abuse, for a rate of 2.35 deaths per 100,000 children. Three fourths of deaths were in children younger than 4 years old. Overall, 41% of fatal cases of child abuse were in Caucasian children, 26% were African American, and 17% were Hispanic. When adjusted for the total population, the highest mortality rate was in African American children at 16.7 per 1,000, followed by Indian/Alaskan native with 14.2 per 1,000 and “multiracial” at 14 per 1,000.9
Physical abuse occurs mostly in young children, with 75% of victims younger than 4 years old. Sexual abuse tends to occur more frequently after puberty but can occur at any age. Girls are at increased risk of infanticide, sexual abuse, and neglect, but boys tend to be at higher risk of harsh, nonfatal physical abuse.7 Children with disabilities, twins, and premature infants appear to be at increased risk.
Overall, abuse is more commonly perpetrated by female caregivers; however, fatal injuries are more commonly caused by men. There may be some cultural differences in the characteristics of perpetrators as Japanese investigators found mothers to be involved more frequently than reported in the western literature.8 Sexual abusers tend to be male: more than 90% with female victims, and 63% to 86% with male victims.7 Low income, single parenthood, and lack of education are other risk factors for perpetrating child maltreatment. Parents who abuse their children tend to have low self-esteem, mental health problems, poor impulse control, and poor education regarding child development and needs, though abuse occurs throughout all socioeconomic and demographic groups and, in fact, there is strong evidence that indicates that child abuse is more likely to be suspected and reported in low socioeconomic visible minorities and underreported in higher socioeconomic Caucasian families.10,11 There is a higher risk of abuse among parents who were themselves victims of abuse as children, though most victims do not become abusers. Intimate partner violence in the home increases the risk of child maltreatment.
The ophthalmologic manifestations of child maltreatment are myriad. It is incumbent on the ophthalmologist to consider abuse in the differential diagnosis of eye trauma, infection, or neglect. Failure to report this suspicion could potentially lead to further injury or even death of the victim, and may be perceived as an act of abuse in itself. There is legal precedent for such prosecution of physicians who failed to report a reasonable suspicion of abuse. In most countries of the developed world, and some countries outside, health professionals are legally bound to report suspected cases of child maltreatment and are legally protected if they do so without malice. Ophthalmologists are often consulted in cases of suspected nonaccidental head trauma to evaluate for retinal pathology. The ophthalmologist, whether the initiator of a CPS referral or a consultant, is part of a large multidisciplinary team of specialists who will help care for the patient/victim to ensure the child is safe from further harm.
PHYSICAL ABUSE
The Battered Child Syndrome
The battered child syndrome refers to any trauma due to physical abuse, including bruises, lacerations, fractures, burns, abdominal trauma, blunt head injury, and other forms of injury.2,12,13 Approximately 40% of physically abused children manifest signs of ocular trauma, occasionally presenting first to the ophthalmologist.8,14,15,16
Systemic Manifestations
The possibility of child abuse should be considered whenever there is wide discrepancy between the explanation for the child’s condition and the physical findings (Table 1). For example, an accidental fall from a couch or bed is a common household occurrence, but serious injury is extremely unlikely. Another clue is inconsistency between the history of injury and the developmental skills of a child. For example, falling off a tricycle at age 1 year when a child is unable to ride a tricycle is a doubtful explanation for a child’s injury. Bruising of almost any kind prior to the child becoming ambulatory is worrisome. Histories that change repeatedly on inquiry from different members of the health care team or new explanations that seem to arise only after a mechanism for injury is suggested should also be considered suspect. A careful history or subsequent investigation may reveal that the child has been treated at different hospitals for a series of injuries of varying severity.
Table 1. Characteristic Features of the Battered Child Syndrome | ||
|---|---|---|
|
Physical examination may provide additional clinical evidence of child abuse (Table 2). Accidental bruising and abrasion is part of normal childhood, but these injuries are usually confined to the knees, anterior surface of the lower legs, the face, and other exposed areas. Accidental injuries do not follow artificial nonbiologic patterns, usually have a viable clear explanation, and are appropriate for the child’s developmental level. Bruises in an infant should raise concern (Fig. 44-1). Bruises that predominate on the buttocks and lower back are often related to punishment, and bruises on the abdomen and the back of the arms and legs often signify abuse, as they are unusual sites for accidental injury. Bruises can be morphologically similar to the implement used to inflict the trauma (Fig. 44-2).17,18 Genital or inner thigh bruises may be the result of punishment for toileting mishaps. Bruises and scars at multiple stages of healing suggest multiple episodes of abuse. Other injuries seen in abused children may include fractures. Although single fractures can certainly occur accidentally, the finding of multiple fractures at various stages of healing (Fig. 44-3) is strongly suggestive of abuse. Life-threatening intra-abdominal, pelvic, and brain injuries (discussed later) may also occur.
Table 2. Physical Manifestations of the Battered Child Syndrome | |
|---|---|
|
 Figure 44-1. Bruise noted on the knee of an infant. This injury should raise concern as the infant is not yet mobile enough to injure himself or herself. |
 Figure 44-2. Distinctive pattern of bruising consistent with a belt loop or chord held to create a loop which is then imprinted on the skin as the child is whipped. |
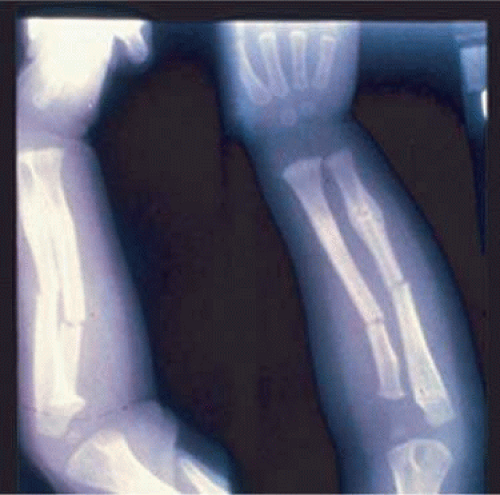 Figure 44-3. Bilateral multiple radius and ulna fractures in a young child abuse victim, in various stages of healing. |
Approximately 10% of all cases of child abuse involve burns.19,20 The most frequent cause of burns in abused children is scalding with hot water. The buttocks and perineum are frequently burned areas. Full-thickness, symmetric burns of the hands or feet suggest strongly that the extremities were held in a hot liquid. Another commonly inflicted burn is from a cigarette. Pattern burns that reflect the shape and nature of an object should raise concerns that the contact was abusive rather than accidental (Fig. 44-4). These lesions are often found on the palms, soles, or abdomen and often have an excavated center with raised edges.
 Figure 44-4. Burn injury in a child from a cigarette lighter. |
Ophthalmic Manifestations
The spectrum of ocular findings in the battered child is vast.14,21 Essentially any injury to the eye or adnexa could be due to abuse. An ocular injury may be as mild as periorbital edema or ecchymosis or as severe as a ruptured globe. Signs of bilateral ocular trauma suggest inflicted injury because accidents usually involve only one eye. Perhaps one exception is bilateral periocular ecchymosis due to an accidental, single, central forehead trauma (Fig. 44-5). Attempts to date bruises by their color is unreliable, particularly in the periorbital area where the loose attachments of the skin to the underlying tissues allow for dramatic accumulations of blood and darker discoloration, which might otherwise suggest an older injury.
 Figure 44-5. Accidental bruise, right forehead, causing bilateral (right greater than left) periorbital ecchymosis. |
There are some eye findings that almost always indicate trauma and others that should raise the possibility of trauma (Table 3). Eyelid, conjunctival, corneal, and scleral lacerations are always due to trauma. Iridodialysis is similarly only a traumatic injury, although this lesion can be mimicked by congenital anterior segment malformations such as Axenfeld-Reiger spectrum. Hyphema is almost always due to trauma although spontaneous “medical hyphema” can occur, for example, as a result of iris neovascularization or juvenile xanthogranulomatosis. Certain vitreoretinal injuries, such as commotio retinae and avulsion of the vitreous base are traumatic injuries. The normal birth process has been associated with multiple ocular injuries including retinal hemorrhages, and complicated forceps deliveries with hyphema, corneal edema, facial palsy, and even ruptured globe.22 Prenatal amniocentesis can also perforate the globe causing various secondary ocular traumas.
Table 3. Ocular Findings in Children That Raise Concern about Trauma | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Subconjunctival hemorrhage is a not uncommon finding in normal birth, occurring in approximately 1% to 2% of normal deliveries. Subconjunctival hemorrhage is also associated with pertussis, hemorrhagic conjunctivitis, and thrombocytopenia. Subconjunctival hemorrhage after birth does not last longer than 2 weeks and occurs in 4% to 10% of battered infants.14,22 Subconjunctival hemorrhage is also a sign of suffocation or strangulation.
Cataract, ectopia lentis, corneal scar, iritis, retinal detachment, and optic atrophy can all occur in the absence of trauma. The ophthalmologist should always consider nonaccidental trauma when there are inconsistencies in the history or exam, or other suspicious findings that do not fit a known, common, ocular condition, particularly when the finding is unilateral. Tseng and Keys23 discuss a case simulating congenital glaucoma in a 9-week-old physically abused infant presenting with hazy enlarged corneas, elevated intraocular pressures, subluxated and cataractous lenses, vitreous hemorrhage, and hyphema.
Corporal punishment is the cause of many body and eye injuries and represents a sensitive and culturally diverse problem. Injuries, such as hyphema or ruptured globe, may be sustained in the course of discipline, occurring “accidentally” during a belt beating (Fig. 44-6). An unexpected move by the child or perpetrator not in control of the implement may cause injury to the eye. Spanking, as a form of discipline, may be controversial, but the use of an implement puts a child at significant risk for injury. Injuries to a child by beating should be reported to child protection agencies, even if the injury occurs accidentally in the course of the beating. Again, the role of the ophthalmologist is to protect the child by reporting possible victims of abuse, and not to determine guilt or innocence of the perpetrator.
 Figure 44-6. Left subconjunctival hemorrhage and periorbital ecchymosis sustained when child moved during belt beating and was struck by belt buckle. Also present (but not visible on this image) are left hyphema and commotio retinae. |
ABUSIVE HEAD TRAUMA AND THE SHAKEN BABY SYNDROME
The classic description of the shaken baby syndrome (SBS) involves central nervous system injury (such as subdural hematoma, subarachnoid hemorrhage, or diffuse axonal injury, cerebral edema, parenchymal contusion or laceration), typical skeletal injury (skull, rib, and/or metaphyseal long bone fractures), and retinal hemorrhages. Recently, the American Academy of Pediatrics recommended the broader term “abusive head trauma” (AHT) to include all forms of abusive head injury with or without the repeated acceleration-deceleration forces (with or without blunt head impact) that characterize SBS.
Abusive head trauma is the most common cause of death in infancy.24 The infant and young child are particularly vulnerable to SBS because of their relatively large head, weak cervical musculature, large size of the cranial vault in relation to the size of the brain, and immature, unmyelinated brain. Violent shaking causes repetitive anteroposterior and side-to-side disorganized head movement with abrupt acceleration-deceleration forces.25 The magnitude of acceleration-deceleration forces needed to cause brain and eye injuries in humans has been the topic of debate. Although in Caffey’s original description of the “whiplash shaken-baby syndrome”25 he inferred that normal play activities could cause AHT-like injuries, this has been widely refuted.24,26 Most victims of AHT are younger than 3 years old, with most younger than 12 months of age. Reported mortality rates vary between 8% and 61%.24,27 Cases in older children, and even adults, are rare but have occurred.
Although one study using a mechanical model and autopsy investigation suggested that blunt head impact is required to generate the forces necessary to cause the brain injury of AHT,28 a wealth of clinical and pathologic investigations indicate that shaking alone can cause significant injury and even death. Violent shaking causes shearing forces that tear the bridging veins running from the cortex to the dural venous sinuses, resulting in subdural and subarachnoid hemorrhage. Shearing also causes diffuse axonal injury with secondary brain edema. Secondary hypoxic-ischemic injury also drives much of the cerebral edema and brain injury.28,29,30 The diagnosis of brain injury is usually confirmed with computed tomography (CT) scan, although the CT scan may initially be normal or show edema without hemorrhage.31,32 Magnetic resonance imaging (MRI) may be useful to find hemorrhage not visualized on CT and to date the findings seen on CT.33
Skull fractures occur in 9% to 31% of shaken babies,27 with the parietal and occipital bones most affected. The characteristics of skull fractures that are highly suggestive of abuse include branching, stellate, crossing suture lines, multiple, greater than 5 mm wide, or progressively expanding fractures in a child younger than 3 years of age.34 Rib fractures are the most common bone injury in AHT and are usually posterolateral due to the perpetrator’s hands grasping the child. The characteristic metaphyseal long bone fractures, which rarely occur in young children except in the setting of abuse, result in a “corner” or “bucket handle” chip fracture at the end of the bone. Other injuries seen in AHT include hemorrhagic stripping of the periosteum, spiral fractures, and nonsupracondylar humerus fractures due to shaking while the infant is held by an extremity, causing the long bones to be twisted and broken.21,28,34,35
The long-term prognosis for children with brain injury secondary to SBS is poor. In one study, only 28% of survivors had normal neurologic exams on discharge from the hospital; this figure decreased to 8% to 14% in long-term studies.27 Late findings seen on imaging studies include cerebral atrophy, hydrocephalus ex vacuo, chronic subdural effusion, and encephalomalacia. Patients may have quadriplegia, diplegia, hemiplegia, mental retardation, developmental delay, learning disability, seizures, and psychiatric/behavioral issues.27,36
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


