The canal wall-down (CWD) tympanomastoid scenario poses several unique challenges in the practice of otology. Although the question of when to perform CWD mastoidectomy is somewhat controversial, all otologists are required to understand how to manage a CWD cavity in the office setting from time to time. Thus, this chapter will highlight the work-up and office management of patients presenting with a discharging open mastoid cavity. Particular attention is given to the pathophysiology associated with an unstable cavity and patterns of failure that will prompt consideration for revision surgery. This information is further complemented by Chapter 35 on CWD mastoidectomy surgical technique and Chapter 41 on mastoid cavity obliteration.
14.2 Pathophysiology and Theories of Mastoid Cavity Instability
A review of the literature projects a variable rate of open mastoid cavity instability ranging from 10% to 60% over the long term.1,2,3,4,5 Several ideas have been proposed over the years to account for why some mastoid cavities will chronically discharge, whereas others are mostly dry and stable. In 1979 Rambo6 put forth one of the first major theories on this topic that would eventually gain widespread popularity, some of which even continues today. Rambo’s hypothesis was that chronic mastoid cavity instability is due to incomplete removal of diseased mastoid air cells that result in the production of moisture, as residual secretory mucosa remains present and active. This theory essentially ascribes mastoid cavity instability to untreated chronic mastoiditis, with the assumption that most ears should be dry if thoroughly drilled.
In 1982 Sade, Weinberg, Berco, Brown, and Halevy published a classic paper that further investigated mastoid cavity instability, wherein four predominant factors were identified among a large series of unstable ears, namely, an open Eustachian tube, a small meatoplasty, a large cavity, and a high facial ridge.2 Interestingly, they noted that there was a cumulative effect of having multiple negative factors at once, to the point where a 100% chance of cavity instability was asserted if all four were in play. Consideration of these findings helped lead to the hypothesis that the shape and dimensions of the mastoid cavity may be the driving determinant of cavity stability as opposed to presence of residual secreting mucosa.
Youngs, who in 1992 published the histopathologic findings from 159 discharging mastoid cavities, explored this concept with further scrutiny.5 His findings demonstrated a strong prominence of ulcerated squamous epithelium with acute and chronic inflammation as well as foreign body granulomas and aural polyp in response to retained keratin debris. Conspicuously uncommon among observed pathology was the presence of mucous cyst formation and secreting mucosa, which was seen in only a limited number of the examined specimens. As such, these findings seemed to reinforce the concept that cavity instability is predominantly a pathologic squamous epithelial response to retained keratin debris and associated infection as opposed to a mucosal secretory phenomenon as had been suggested previously by Rambo.
Wormald and Neilson examined this “retention theory” even further by studying the impact of various factors related to cavity shape and size on cavity stability.4 In 1998, their publication included detailed mastoid cavity measurements from over 100 ears prospectively examined in a clinic over a one-year period of time. They determined that a high facial ridge, a “kidney-shaped” cavity, an open mastoid tip, an open Eustachian tube (typically in the form of a perforated tympanic membrane), and a small external auditory meatus would be expected to impart a negative effect on cavity stability. In particular, a high facial ridge and a kidney-shaped cavity, which relates to the contour of the inferior tympanic bone relative to the adjacent mastoid cavity, were noted to have particular impact from a statistical perspective. However, in contrast to Sade, they did not find the absolute volume of the cavity to be significant.
In addition to the contour of the mastoid cavity, the relative size of the meatus, and the status of the tympanic membrane, the presence of recurrent cholesteatoma has since been identified as an additional negative factor that is often found in unstable mastoid cavities.7 Although residual and recurrent cholesteatoma rates should be low after CWD mastoidectomy, failures still can occur. It is a flawed notion that CWD surgery always alleviates the need for a second-look procedure. For example, this is certainly not the case if cholesteatoma extensively involved the mesotympanum because this area is not exteriorized during most CWD surgeries. Thus, chronic otorrhea should always prompt consideration that cholesteatoma may be present, even in the CWD setting.
14.3 Symptoms of an Unstable Mastoid Cavity
The hallmark of an unstable mastoid cavity is chronic otorrhea, which often can be quite foul smelling. Worsened hearing, otic fullness, and pain are possible but less common.1 Vertigo is also possible due to caloric effects, even in a stable cavity, but may be more pronounced when the cavity requires treatment with otic drops or aural suctioning. An unstable cavity will not be compatible with an ear-level hearing aid. In some instances, a previously stable cavity will start to discharge after a hearing aid is fit, presumably due to the resultant increase in moisture and microbial load induced by canal occlusion.8 In other ears, instability is brought about during periods of ongoing water exposure.
14.4 Examination and Assessment of a Mastoid Cavity
Microscopic examination of the ear should include inspection for the presence of pus, fungal elements, granulation tissue, aural polyp, cholesteatoma, and myringitis. Careful note is made of the status of the neotympanic membrane. Given our current evolved knowledge of open mastoid cavity pathophysiology, key factors that may contribute to chronic instability should be examined. These are portrayed in ▶ Fig. 14.1, and a brief description follows.
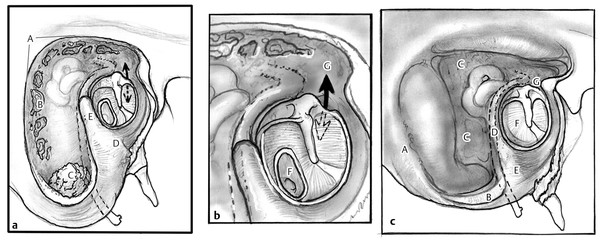
Fig. 14.1 An unfavorable versus a properly formed canal wall-down mastoidectomy. (a) In the unfavorable cavity note the steep non-saucerized edges, the potholes from residual air cells, the intact open mastoid tip with debris, the uncontoured tympanic bone forming a kidney-shaped cavity, the high facial ridge. A, steep non-saucerized edges; B, potholes from residual air cells; C, intact open mastoid tip with debris; D, uncontoured kidney-shaped tympanic bone; E, high facial ridge; (b) Also note the tympanic membrane perforation, and the unsealed communication between the mesotympanum and the exteriorized epitympanum. F, tympanic membrane perforation; G, unsealed communication with epitympanum. (c) In contrast, the properly formed canal wall-down mastoidectomy features saucerized edges, a mastoid tip that has been amputated from the digastric muscle, air cells that have been drilled away until the smooth posterior and middle fossa dural plates are exposed, a completely lowered facial ridge, an inferior tympanic bone that has been rendered concave having a smooth junction with the mastoid, an intact tympanic membrane, and an intact seal between the epitympanum and the mesotympanum. A, saucerized edges; B, mastoid tip amputated from digastric muscle; C, cells drilled away up to smooth dural plate; D, facial ridge lowered; E, tympanic bone smoothly fractured with junction of mastoid; F=intact tympanic membrane; G, middle ear sealed from epitympanum.
14.4.1 Mastoid Tip
If the mastoid tip is both present and open, it will possibly act as a gravity-dependent sewer or sump, with associated accumulation of moisture and debris. It may also be difficult in some cases to completely visualize and manipulate the entirety of an open tip in the office.
14.4.2 High Facial Ridge
A high facial ridge is defined as having >2 mm of bone overlying the mastoid segment of the facial nerve, and it should be lowered at least to the level of the chorda tympani–facial nerve junction.4,9 It has been found that surgeons tend to either lower the facial ridge completely or not at all. If high, the ridge of bone acts as a steep cliff that can impede epithelial migration (▶ Fig. 14.2). The determination of ridge height is made either by microscopic examination or by reviewing radiologic images.
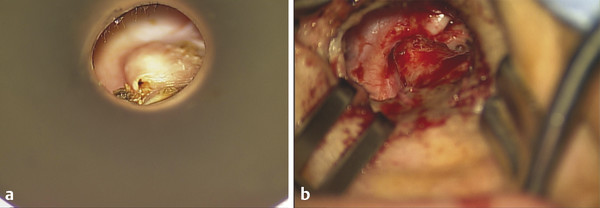
Fig. 14.2 High facial ridge. (a) Office view of a high facial ridge in a right ear. Note the presence of retained debris to the left of the ridge, which was extending into the mastoid tip. (b) Intraoperative view in the same patient with skin dissected off of the high facial ridge before drilling.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


