 Questions
Questions
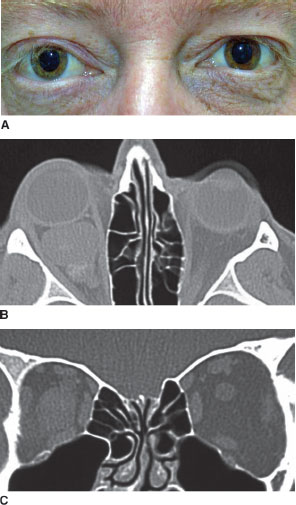
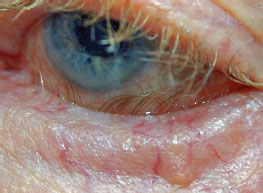
1. A patient is referred for a postoperative evaluation of a 1.2 g gold weight implanted in the left upper eyelid for facial nerve palsy. The patient is shown below in attempted closure of the eye. The complication depicted may be avoided by which of the following?
a. Using a 0.8 g gold weight implant.
b. Using a 1.8 g gold weight implant.
c. Inserting the weight under the orbicularis muscle.
d. Meticulous suture closure of the skin.

2. A patient is (shown in the right column) in attempted closure of his eyes. The surgical management of the patient’s condition includes all of the following, except
a. gold weight implantation.
b. lower eyelid repair.
c. blepharoplasty.
d. brow lifting.

3. A patient with eyelid ptosis, suspected of having myasthenia gravis, undergoes pharmacologic testing with edrophonium chloride (Tensilon). All of the following are potential side effects of edrophonium testing, except
a. respiratory arrest.
b. tachycardia.
c. vomiting.
d. syncopy.
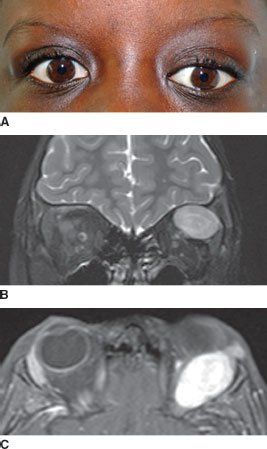
4. Which of the following is the most appropriate imaging study for a patient diagnosed with myasthenia gravis (MG)?
a. MRI scan of the brain.
b. B-scan ultrasonography.
c. CT scan of the chest.
d. carotid Doppler ultrasonography.
5. The patient developed the lesion shown below on the left lower eyelid over the last month. All of the following are true of this condition, except:
a. The central crater is filled with sebaceous material.
b. There is an increased incidence in immunosuppressed individuals.
c. Complete surgical excision is advised.
d. The lesion may involute over the next 3 to 6 months.

6. An 11-year-old patient photographed below presents with a variable position of the left upper eyelid. The observed changes occur with opening and closing of the mouth. The condition is most commonly due to synkinesis of which two cranial nerves?
a. oculomotor and trigeminal.
b. abducens and oculomotor.
c. facial and oculomotor.
d. trochlear and abducens.

7. Eyelid synkinesis can occur in all of the following, except
a. congenital neurogenic blepharoptosis.
b. ocular myasthenia gravis.
c. aberrant nerve regeneration.
d. duane retraction syndrome.
8. A 74-year-old patient had noticed eyelid drooping, which had worsened over the last several years (photographed below). The levator function was 15 mm bilaterally and the extraocular motility was full in both eyes. The patient is seen preoperatively and postoperatively after having undergone ptosis repair. Which of the following is characteristic of this patient’s ptotic eyelids?
a. eyelid lag.
b. supratarsal thickening.
c. difficulty reading.
d. unrelated to cataract surgery.

9. The patient in the figures at the top of the next page is noted to have developed axial proptosis and downward displacement of the left eye over the last 2 weeks. After complete examination, the next most appropriate step is to proceed with which of the following?
a. observation.
b. chemotherapy.
c. bone marrow biopsy.
d. anterior orbitotomy for biopsy.
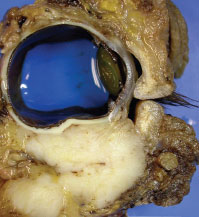
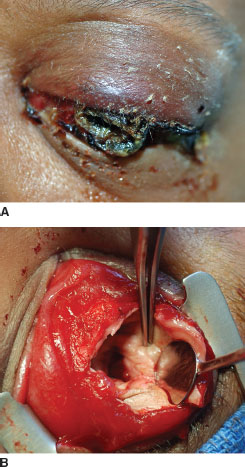
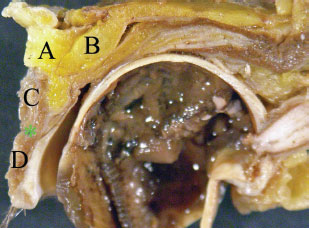
10. The gross examination of tissue following a patient’s surgery is shown below. With regard to the type of surgery performed, all of the following tumors may appropriately be addressed by the type of surgery shown, except
a. sebaceous carcinoma with deep orbital invasion.
b. primary orbital rhabdomyosarcoma.
c. extraocular extension of melanoma without systemic metastasis.
d. orbital phycomycosis.
11. In comparison to benign mixed tumor, all of the following clinical features are more characteristic of adenoid cystic carcinoma, except
a. progression over weeks to months.
b. presence of bone erosion.
c. hypesthesia in temporal region.
d. older age.
12. In comparison to benign mixed tumor, all of the following clinical features are more characteristic of lymphoid tumors of the lacrimal gland, except
a. bony remodeling.
b. absence of globe ptosis.
c. more anterior location.
d. soft to palpation.
13. Where is the peripheral arterial arcade in the upper eyelid located?
a. between the levator aponeurosis and Müller’s muscle.
b. along the anterior surface of the tarsus.
c. 2 mm superior to the eyelid margin.
d. between the orbicularis oculi muscle and levator aponeurosis.
14. Distention of the lacrimal sac superior to the medial canthal tendon is suggestive of which of the following?
a. primary acquired nasolacrimal duct obstruction.
b. canaliculitis.
c. tumor.
d. dacryolithiasis.
15. As the bony nasolacrimal canal runs inferiorly it initially curves
a. medial and anterior.
b. lateral and posterior.
c. medial and posterior.
d. lateral and anterior.
16. The patient shown below was referred in consultation for a malposition of the right lower eyelid. Six years prior, the patient had a basal cell carcinoma of the inferonasal right lower eyelid removed. The postexcision defect had been repaired with a full thickness skin graft to the medial half of the eyelid. Appropriate surgical management for the patient’s current right lower eyelid condition includes all of the following, except
a. incision and relaxation of vertical traction.
b. horizontal eyelid tightening.
c. eyelid retractor repair.
d. vertical lengthening of anterior lamella.

17. Which one of the following disorders typically produces downward and lateral displacement of the globe?
a. malignant mixed tumor of the lacrimal gland.
b. squamous cell carcinoma of the maxillary sinus.
c. frontal sinus mucocele.
d. optic nerve sheath meningioma.
18. All of the following disorders typically present with a rapid onset, except
a. benign mixed tumor of the lacrimal gland.
b. ruptured dermoid cyst.
c. rhabdomyosarcoma.
d. orbital cellulitis.
19. A 42-year-old patient presents with a left lower eyelid lesion shown in the image at the top of the right column. What is the most appropriate initial step in the management of this patient’s condition?
a. incision and curettage.
b. observation.
c. full-thickness excisional biopsy.
d. incisional biopsy.
20. Compared with botulinum toxin type A, all of the following are true regarding botulinum toxin type B, except
a. more injection discomfort.
b. greater diffusion of the toxin.
c. quicker onset of effect.
d. longer duration of action.
21. All of the following favor the diagnosis of benign essential blepharospasm over hemifacial spasm, except
a. absence of abnormal movements during sleep.
b. no involvement of lower facial muscles along with orbicularis muscle.
c. synchronous contractures of involved muscles.
d. lack of response to neurosurgical decompression of the facial nerve.
22. A 49-year-old patient presents with bilateral upper eyelid ptosis as demonstrated in the photograph below. The patient has been using rigid gas permeable contact lenses for years. The levator function is 16 mm bilaterally and the extraocular motility is full in both eyes. What is the most likely etiology of her condition?
a. involutional attenuation.
b. repetitive eyelid traction.
c. levator muscle dysgenesis.
d. diffuse muscular disease.

23. The most common cause of unilateral proptosis in children is
a. thyroid ophthalmopathy.
b. rhabdomyosarcoma.
c. orbital pseudotumor.
d. orbital cellulitis.
24. The most common location for an orbital meningocele is the
a. supraorbital notch.
b. lateral canthus.
c. lacrimal gland fossa.
d. medial canthus.
25. The patient represented in the photograph below is referred for evaluation of right eye proptosis, chemosis, and tortuous conjunctival vessels, which extend to the limbus. In addition, the right eye has limitation of right lateral gaze and an audible cranial bruit. The patient has a history of severe head trauma. Subsequent CT scan confirms the absence of a mass and shows a dilated superior ophthalmic vein. All of the following are true of the patient’s condition, except
a. elevated orbital venous pressure.
b. direct high-flow fistula.
c. low thyroid stimulating hormone.
d. extraocular muscle enlargement.
26. A 73-year-old woman presents to the ophthalmologist complaining of mild redness and irritation of her left eye for approximately 2 months. She denies any head trauma. Visual acuity is normal bilaterally. There is 3 mm of proptosis on the left with mild tortuosity of the retinal vasculature of the left eye. Intraocular pressure is 12 mm Hg in the right eye and 30 mm Hg in the left eye. Arterialization of the orbit is most likely caused by a disturbance in the
a. central retinal artery.
b. branches of the middle meningeal artery.
c. common carotid artery.
d. intracavernous internal carotid artery.
27. The most common orbital or eyelid finding in the craniosynostosis syndromes is
a. ankyloblepharon.
b. blepharophimosis and ptosis.
c. V-pattern exotropia.
d. hypertelorism and proptosis.
28. The most common risk factor for the development of preseptal cellulitis is
a. recent upper respiratory infection.
b. recent skin trauma.
c. recent orbital fracture.
d. sinusitis.
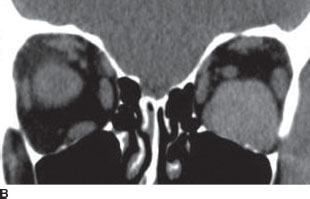
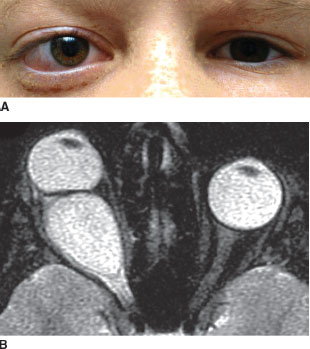
29. A 58-year-old woman presents with a 6-week history of left upper eyelid ptosis as demonstrated in image A at the top of the next page. With lifting of her eyelid she experiences diplopia and has poor extraocular motility of the left eye. Her past medical history is significant for estrogenreceptor–positive breast cancer treated 6 years ago. Orbital imaging (images B and C at the top of the next page) shows a mass of the orbital apex and subsequent biopsy shows an estrogen-receptor– negative breast cancer. Which of the following is true of breast cancer metastatic to the orbit?
a. the majority of orbital metastases in women originate from breast cancer.
b. this patient will likely benefit from hormone therapy.
c. bone metastasis is more common than extraocular muscle involvement.
d. enophthalmos is an expected finding in this patient.
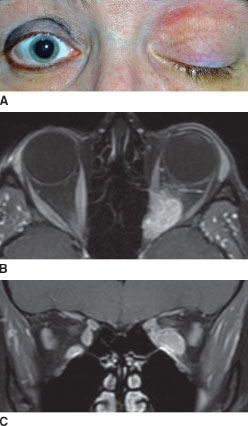
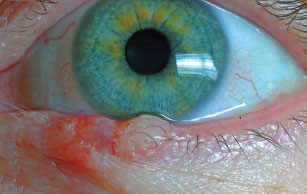
30. The position of the patient’s right upper eyelid in question 29 is best explained by
a. coexistent hyperthyroidism.
b. right facial nerve palsy.
c. left upper eyelid ptosis.
d. metastatic infiltration of right superior rectus/ levator muscle complex.
31. An infant presents with ptosis of the right upper eyelid as pictured below. Which of the following best describes the type of blepharoptosis?
a. aponeurotic.
b. mechanical.
c. neurogenic.
d. myogenic.

32. With varying frequency, all of the following are used in the treatment of the condition in the previous question, except
a. dextromethorphan.
b. propranolol.
c. clobetasol propionate.
d. interferon-a.
33. Which of the following can be associated with multiple large capillary hemangiomas?
a. thrombocytosis.
b. leukocytosis.
c. thrombocytopenia.
d. leukocytopenia.
34. A patient with suspected orbital cellulitis suddenly worsens with a virtually frozen globe, without a measurable increase in proptosis. Corneal sensation is likewise diminished, but visual acuity remains grossly intact. The most likely explanation for these events is
a. cavernous sinus thrombosis.
b. orbital compartment syndrome.
c. meningitis secondary to orbital cellulitis.
d. orbital apex syndrome.
35. A sensitive finding in direct naso-orbital-ethmoid fracture is
a. telecanthus.
b. hypoglobus.
c. infraorbital hypesthesia.
d. epistaxis.
36. All of the following findings are consistent with an isolated inferior orbital wall fracture and soft issue entrapment except
a. subcutaneous emphysema.
b. infraorbital hypesthesia.
c. limitation in ocular motility in all fields of gaze.
d. hypoglobus.
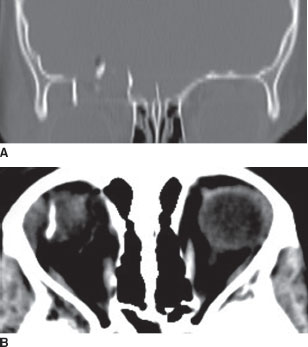
37. A 5-year-old boy fell while riding his bicycle. A CT scan performed in the emergency room is shown at the top of the next page. Which of the following is characteristic of the injury shown in this patient?
a. Fractures of the orbital floor or medial wall are more common.
b. The injury tends to occur in adults.
c. The patient likely fell from a height greater than that of his bicycle.
d. An upper eyelid hematoma is an expected finding.
38. All of the following are recognized causes of enophthalmos, except
a. silent sinus syndrome.
b. orbital varix.
c. medial wall orbital fracture.
d. malar hypoplasia.
39. The nevus flammeus, which may be mistaken for a capillary hemangioma, is seen as a part of what systemic disorder?
a. neurofibromatosis.
b. Treacher Collins’ syndrome.
c. von Hippel’s disease.
d. Sturge-Weber syndrome.
40. Greater than 90% of periocular capillary hemangiomas manifest by
a. 4 to 8 weeks of age.
b. 6 to 8 months of age.
c. 12 to 18 months of age.
d. 3 to 4 years of age.
41. Most capillary hemangiomas reach their peak size at approximately what age?
a. 2 to 3 months.
b. 6 to 12 months.
c. 12 to 24 months.
d. 3 to 5 years.
42. The key clinical feature distinguishing between nevus flammeus and capillary hemangioma is
a. lesion color.
b. presence or absence of blanching with pressure.
c. area of skin affected.
d. extent of skin thickening.
43. Which one of the following most accurately reflects the relative percentages of patients with thyroid eye disease (Graves’ patient percentages)?
a. 96% hyperthyroidism, 1% autoimmune thyroiditis, 3% euthyroid.
b. 93% hyperthyroidism, 1% autoimmune thyroiditis, 6% euthyroid.
c. 90% hyperthyroidism, 1% hypothyroidism, 3% autoimmune thyroiditis, 6% euthyroid.
d. 87% hyperthyroidism, 3% hypothyroidism, 5% autoimmune thyroiditis, 5% euthyroid.
44. Which one of the following signs is considered classic for CT scanning in Graves’ ophthalmopathy?
a. kinking of extraocular muscles.
b. nodular muscle enlargement.
c. fusiform muscle enlargement with sparing of tendons.
d. solitary muscle enlargement.
45. After eyelid retraction, what is the expected order of eyelid findings in patients with Graves’ ophthalmopathy (in order from most frequent to least frequent)?
a. von Graefe’s sign > lid lag > lagophthalmos.
b. lagophthalmos > von Graefe’s sign > lid lag.
c. lid lag > von Graefe’s sign > lagophthalmos.
d. von Graefe’s sign > lagophthalmos > lid lag.
46. Before undertaking surgical correction of strabismus in Graves’ ophthalmopathy, the angle of deviation should be stable for what period of time?
a. 1 month.
b. 3 months.
c. 6 months.
d. 1 year.
47. A 57-year-old woman presents with a blind painful left eye, which has secondarily developed perforation of the cornea. The patient underwent a surgical procedure for her condition (seen below). With regard to this patient, all of the following statements are correct, except
a. The procedure is appropriate even in the setting of endophthalmitis.
b. There is a future risk of developing granulomatous inflammation in the right eye.
c. Posterior incisions in the sclera allow for placing a larger orbital implant.
d. The cornea may be retained provided the epithelium and endothelium are removed.
48. The most common postoperative complication of enucleation is
a. socket contracture.
b. enophthalmos.
c. superior sulcus deformity.
d. extrusion of implant.
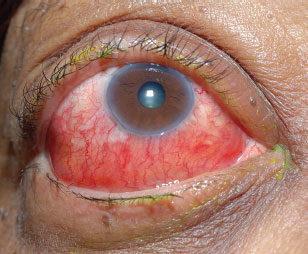
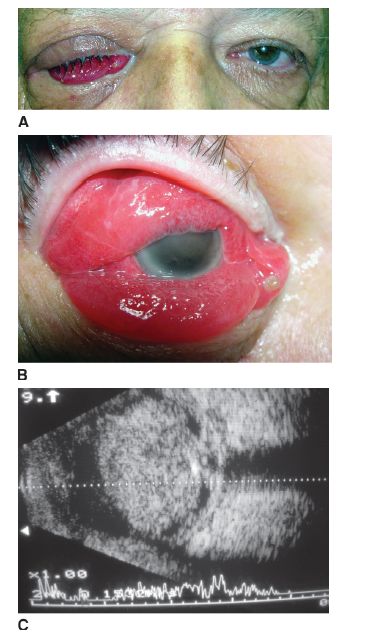
49. A 68-year-old man presents with blind painful right eye, proptosis, and chemosis as photographed below. Which of the following treatments is most appropriate in the management of this patient?
a. enucleation.
b. retrobulbar alcohol injection.
c. evisceration.
d. diode laser cyclophotocoagulation.
50. Which one of the following regarding a biopsy of orbital rhabdomyosarcoma is false?
a. Metastatic workup includes lumbar puncture and bone marrow biopsy.
b. The most malignant variant, alveolar rhabdomyosarcoma, occurs most frequently in the superior orbit.
c. Electron microscopic studies may be used in facilitating the diagnosis, as cross-striations are more apparent on electron microscopy.
d. The embryonal pattern is the most common pathologic variant, accounting for more than 80% of total cases.
51. A patient with known neurofibromatosis presents with pulsating proptosis of long duration. CT scan of the orbit will most likely reveal
a. orbital neurofibroma.
b. abnormality of the sphenoid bone.
c. optic nerve glioma.
d. carotid–cavernous fistula.
52. A 33-year-old patient with type I diabetes mellitus presents with a 2-week history of gradually progressive proptosis, redness, and irritation in the left eye. Visual acuities are 20/20 in the right eye and 20/100 in the left eye. There is an afferent pupillary defect on the left, along with 4 mm of proptosis and moderate conjunctival injection. Ductions are normal on the right and globally reduced on the left. CT scanning reveals left ethmoid and maxillary sinusitis with evidence of orbital involvement. The next step in the proper evaluation of this patient is
a. complete blood count.
b. oral temperature.
c. blood glucose.
d. careful ear, nose, and throat evaluation.
53. Which one of the following papillomatous lesions of the eyelid is considered premalignant?
a. acanthosis nigricans.
b. actinic keratosis.
c. seborrheic keratosis.
d. verruca vulgaris.
54. Which of following papillomatous lesions of the eyelid may be associated with underlying systemic malignancy?
a. acanthosis nigricans.
b. verruca vulgaris.
c. ephelis.
d. actinic keratosis.
55. What preoperative medication is most appropriate for reducing the chance of irreversible scarring in patients prior to undergoing laser skin resurfacing?
a. valacyclovir.
b. prednisone.
c. diphenhydramine.
d. mitomycin-C.
56. Laser skin resurfacing is contraindicated in patients taking which one of the following medications?
a. isotretinoin.
b. hydrochlorothiazide.
c. docetaxel.
d. sildenafil citrate.
57. Elevation of what structure to its previous anatomic position is often used to perform midface rejuvenation?
a. preseptal orbicularis.
b. suborbicularis oculi fat.
c. retroorbicularis oculi fat.
d. medial canthal tendon.
58. All of the following are true regarding sebaceous carcinoma, except:
a. The primary focus may be either eyelid or caruncle.
b. Shave biopsy techniques are adequate.
c. The hallmarks of the histopathology of the condition include skip areas and pagetoid intraepithelial spread of malignancy.
d. Recognition is often delayed due to misdiagnosis as benign eyelid inflammation.
59. All of the following are true regarding malignant melanoma of eyelid skin, except:
a. Lentigo maligna melanoma and nodular melanoma are the most common forms affecting the eyelid.
b. Nodular melanoma is the most rare eyelid melanoma and has the worst prognosis.
c. The factor of greatest prognostic significance is depth of invasion.
d. Like conjunctival melanosis, eyelid melanoma may be controlled with cryotherapy.
60. A 14-year-old patient presents with a left upper eyelid lesion as photographed at the top of the next page. Histopathology of the lesion showed shadow cells and areas of calcification surrounded by basophilic cells. All of the following are true of the patient’s condition, except:
a. Young adults are most often affected.
b. The lesion is epithelial in origin.
c. Surgical excision of the lesion is curative.
d. The eyebrow is also a common site of involvement.

61. Typical manifestations of idiopathic orbital inflammation (pseudotumor) include all of the following, except
a. dacryoadenitis.
b. optic perineuritis.
c. periscleritis.
d. peripheral ulcerative keratitis.
62. Compared with adults, all of the following findings are more common in pediatric idiopathic orbital inflammation (orbital pseudotumor), except
a. uveitis.
b. optic disc edema.
c. unilateral presentation.
d. eosinophilia.
63. All of the following disorders may be associated with a clinical presentation indistinguishable from typical inflammatory orbital pseudotumor, except
a. Wegener’s granulomatosis.
b. Churg-Strauss syndrome.
c. sarcoidosis.
d. polyarteritis nodosa.
64. All Le Fort fractures (I, II, and III) must extend posteriorly through what bone?
a. pterygoid plates.
b. maxillary bone.
c. zygomaticomaxillary complex.
d. naso-orbital-ethmoidal.
65. The optimal time for surgical repair of orbital floor fractures is generally considered to be
a. within 24 hours of injury.
b. 1 to 3 days following injury.
c. 2 weeks following injury.
d. 6 weeks following injury.
66. A 76-year-old patient is referred for left upper eyelid ptosis. Examination shows an incomitant strabismus and a lesion of the left lower eyelid, lateral canthus, and conjunctiva (see image below). The patient has a history of prior basal cell carcinoma of the left lower eyelid. A biopsy confirms recurrence of basal cell carcinoma. CT scan shows a mass extending deeply in the lateral orbit. What treatment is recommended?
a. orbital exenteration.
b. full-thickness pentagonal wedge resection.
c. cryotherapy.
d. radiation therapy.

67. Consultation is requested for a patient who sustained massive facial trauma. Which of the following statements accurately characterizes the condition shown in the image below by the metal probe?
a. After surgical repair, stents are left in place for 3 weeks.
b. Direct suturing of the cut ends is required.
c. Irrigation using methylene blue may facilitate intraoperative visualization.
d. Repair of all such injuries is recommended.

68. What is the composition of the crescent-shaped structure of the orbit known as the trochlea?
a. cartilage.
b. fibrous tissue.
c. bone.
d. adipose tissue.
69. The biologic response modifier, rituximab, binds to which of the following targets?
a. CD11a.
b. CD20.
c. CD25.
d. TNF-α.
70. What percentage of infants are born with an imperforate valve of Hasner (distal end of the nasolacrimal duct)?
a. 10%.
b. 20%.
c. 50%.
d. 80%.
71. Which one of the following ganglia serves as the home for cell bodies providing postganglionic efferent innervation to the lacrimal gland?
a. ciliary.
b. sphenopalatine.
c. geniculate.
d. superior cervical.
72. Approximately how many days after birth do infants gain full tear production?
a. 14 days.
b. 21 days.
c. 35 days.
d. 42 days.
73. The most common neoplasm of the lacrimal gland is the
a. adenoid cystic carcinoma.
b. mucoepidermoid carcinoma.
c. benign mixed tumor.
d. adenocarcinoma.
74. The most common malignant neoplasm of the lacrimal gland is the
a. adenoid cystic carcinoma.
b. mucoepidermoid carcinoma.
c. maligant mixed tumor.
d. adenocarcinoma.
75. What anatomic structure divides the lacrimal gland anteriorly into orbital and palpebral lobes?
a. orbital septum.
b. periorbita.
c. superior transverse ligament.
d. levator aponeurosis.
76. A 30-year-old man presents with a 2-year history of gradually progressive proptosis of the right eye. There is no associated pain or inflammation. CT scanning reveals globular enlargement of the lacrimal gland with no extension anterior to the orbital rim. All of the following are true, except
a. Initial approach to the patient should include an incisional biopsy.
b. Histopathology will show the tumor has a pseudocapsule.
c. Definitive treatment will necessitate lateral orbitotomy.
d. The most likely diagnosis is more frequently encountered in men.
77. In evaluating a child with tearing, all of the following are causes of reflex hypersecretion, except
a. encephalocele.
b. glaucoma.
c. trichiasis.
d. epiblepharon.
78. A 3-year-old patient presents with a painless lesion of the lateral left upper eyelid and brow. The lesion is smooth and fixed to the underlying bone. Based on the most likely diagnosis, which of the following general statements is true of these types of lesions (image at the top of the next page)?
a. An eyelid crease incision usually does not provide sufficient exposure.
b. The lesion is classified as a hamartoma.
c. The condition may occur along the superomedial orbital rim.
d. The lesion is lined by nonkeratinizing squamous epithelium with dermal appendages.

79. A patient presents to an ophthalmology emergency room after being struck over the left eye with a baseball bat. Examination reveals a 24-year-old man in acute distress. Visual acuity is 20/20 in the right eye and light perception in the left eye. There is an obvious left afferent pupillary defect. There is taut ecchymosis of the left upper and lower lid, with 3 mm of proptosis on the left. With the left lids tensely pried apart, ductions are normal in the right eye and barely detectable in the left eye. There is hemorrhagic chemosis 360° in the left eye and a microhyphema. Funduscopic examination is normal with the exception of obvious arterial pulsations. Intraocular pressure is 75 mm Hg. The next step to be taken is emergent
a. intravenous methylprednisolone.
b. lateral canthotomy and cantholysis.
c. intravenous acetazolamide and mannitol.
d. exploration of the globe.
80. A patient presents to an ophthalmology emergency room after tumbling off a bicycle and striking his head on the pavement. Examination reveals a 24-year-old man in mild discomfort holding his head. There is a 5-mm abrasion on the left temple. Visual acuity is 20/20 in the right eye and light perception in the left eye. There is an obvious left afferent pupillary defect. There is no periorbital edema, and extraocular movements are full. The slit-lamp examination, fundus examination, and intraocular pressures are normal. Confrontation visual fields are full in the right eye. The next step to be taken is emergent
a. CT scan.
b. lateral canthotomy and cantholysis.
c. oral prednisone.
d. intravenous acetazolamide.
81. The patient photographed below is seen in consultation for facial soft tissue trauma. CT scan shows an absence of fractures. The right lower eyelid is completely avulsed. In addition to cana-licular repair, reattachment of the medial canthal tendon to which of the following structures is necessary for reconstruction of the normal eyelid anatomy?
a. medial orbital tubercle.
b. anterior process of the maxilla.
c. anterior lacrimal crest.
d. posterior lacrimal crest.

82. To allow maximal spontaneous return of function before surgical repair, it is generally wise to observe traumatic ptosis in an adult for what period of time?
a. 4 weeks.
b. 2 months.
c. 6 months.
d. 12 months.
83. A patient sustained a severe motor vehicle accident, which included a tree branch penetrating the left medial orbit. The avulsed globe was found at the site of the accident. The entire length of superior oblique tendon is seen draped along the posterior and inferior aspects of the globe. The optic nerve starts at the 4.9 cm mark and attaches to the back of the eye at the 8.1 cm mark on the ruler. What is the name of the region of optic nerve at the cut (avulsed) end?
a. intraocular.
b. intraorbital.
c. intracanalicular.
d. intracranial.

84. A patient photographed in the image A below reports the acute onset of left eye proptosis and painful diplopia after prolonged retching following an episode of alcohol binge drinking. CT scan shows a space-occupying mass (see image B at the top of the right column). The patient has decreased vision, a relative afferent papillary defect, elevated intraocular pressure, and optic disc hyperemia. What is the most appropriate management recommendation?
a. aqueous suppressant medications.
b. surgical drainage.
c. observation.
d. anterior chamber paracentesis.

85. The systemic disorder most commonly associated with the blepharophimosis syndrome is
a. diabetes mellitus.
b. primary amenorrhea.
c. hypospadias.
d. coarctation of the aorta.
86. A 45-year-old woman presents with an encapsulated well-circumscribed retrobulbar mass of the left orbit demonstrated in the image below. All of the following are potential diagnoses, except
a. neurilemoma.
b. hemangiopericytoma.
c. lymphangioma.
d. fibrous histiocytoma.

87. Which one of the following regarding dermoid and epidermoid cysts is false?
a. They share a common pathophysiology.
b. The key distinguishing feature between the two is the nature of the wall of the cystic cavity.
c. In adults, nearly all of these lesions are anterior to the orbital septum.
d. Superficial cysts present more often during childhood.
88. An image of a left orbit is shown below. What lettered location best represents the most common site of adherence for a dermoid cyst?
a. location A.
b. location B.
c. location C.
d. location D.
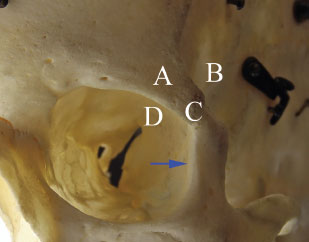
89. In question 88, a blue arrow is seen in the figure. The arrow points to a small palpable structure just inside the orbital rim. All of the following structures attach to the site indicated by the blue arrow, except
a. superior transverse ligament of the orbit.
b. aponeurosis of the levator palpebrae superioris muscle.
c. suspensory ligament of the eyeball.
d. lateral check ligament of the inferior oblique muscle.
90. A patient presents with slowly progressive pro-ptosis of the right eye. Excisional biopsy confirms large cavernous spaces containing erythrocytes (images A,B, and C below). All of the following may be seen in this condition, except
a. accelerated growth of the lesion in a pregnant patient.
b. anterior displacement of the far point plane of the eye.
c. more than one type of optic neuropathy.
d. radiodense phleboliths present on CT scan imaging.
91. What is the expected reflectivity on A-scan ultrasonography of the capsule of the lesion in the previous question?
a. none.
b. low.
c. medium.
d. high.
92. In patients with eyelid ptosis, which of the following is the most important measure in determining the type of surgery to perform?
a. margin reflex distance.
b. eyelid excursion.
c. response to phenylephrine testing.
d. palpebral fissure.
93. If one makes an incision 15 mm above the eyelid margin through the full thickness of the central upper eyelid, what is the correct order of the anatomic structures encountered?
a. skin, orbicularis oculi muscle, orbital septum, orbital fat, levator aponeurosis, Müller’s muscle, conjunctiva.
b. skin, orbital septum, orbicularis oculi muscle, orbital fat, levator aponeurosis, Müller’s muscle, conjunctiva.
c. skin, orbicularis oculi muscle, orbital septum, orbital fat, Müller’s muscle, levator aponeurosis, conjunctiva.
d. skin, orbicularis oculi muscle, orbital fat, orbital septum, levator aponeurosis, Müller’s muscle, conjunctiva.
94. A 2-year-old child presents with bilateral proptosis. Which of the following is the least likely diagnosis?
a. metastatic neuroblastoma.
b. leukemia.
c. capillary hemangioma.
d. orbital pseudotumor.
95. The average distance from lacrimal punctum to nasolacrimal sac is
a. 2 mm.
b. 8 mm.
c. 10 mm.
d. 30 mm.
96. What is the organism that most commonly causes canaliculitis?
a. Nocardia asteroides.
b. Staphylococcus.
c. Candida albicans.
d. Actinomyces israelii.
97. All of the following medications are known to potentially cause canalicular obstruction, except
a. phospholine iodine.
b. 5-fluorouracil.
c. doxorubicin.
d. idoxuridine.
98. What type of epithelium are the lacrimal canaliculi lined by?
a. stratified cuboidal.
b. pseudostratified ciliated columnar.
c. stratified squamous.
d. bilayered cuboidal.
99. An infant with congenital nasolacrimal duct obstruction undergoes lacrimal probing. Starting from the punctum, what distance will the probe travel before reaching the inferior meatus?
a. 12 mm.
b. 20 mm.
c. 24 mm.
d. 30 mm.
100. In adults, the average distance from lacrimal punctum to inferior nasal meatus is
a. 2 mm.
b. 8 mm.
c. 10 mm.
d. 30 mm.
101. What is the most commonly performed clinical test in the evaluation of the adult patient with epiphora?
a. Jones I test.
b. Jones II test.
c. lacrimal irrigation.
d. dye disappearance test.
102. Which one of the following functional tests of lacrimal drainage is most likely to yield a false-positive result?
a. lacrimal scintigraphy.
b. secondary dye test (Jones II test).
c. dye disappearance test.
d. primary dye test (Jones I test).
103. Which one of the following functional tests of lacrimal drainage allows identification of a failure of the lacrimal pump mechanism?
a. Schirmer’s test.
b. primary dye test (Jones I test).
c. dye disappearance test.
d. secondary dye test (Jones II test).
104. A 75-year-old patient is brought in from the nursing home for acute dacryocystitis. Which of the following is the most appropriate initial step in the treatment of this patient?
a. dacryocystorhinostomy.
b. broad-spectrum antibiotics.
c. nasolacrimal duct probing.
d. canalicular irrigation.
105. The most important predisposing factor for acute dacryocystitis is
a. chronic blepharitis.
b. acute bacterial conjunctivitis.
c. dry eye.
d. tear stasis of any etiology.
106. When performing an endoscopic dacryocystorhinostomy, all of the following bones are often removed, except
a. nasal.
b. maxilla.
c. lacrimal.
d. ethmoid.
107. Acute, lancinating pain in the medial canthal region with minimal noninflamed enlargement of the lacrimal sac is most suggestive of
a. impacted dacryolith.
b. acute dacryocystitis.
c. chronic dacryocystitis.
d. Wegener granulomatosis.
108. The most common site of organic obstruction in acquired nasolacrimal obstruction is
a. intraosseous nasolacrimal duct.
b. punctum.
c. valve of Hasner.
d. canaliculus.
109. All of the following may occur in a patient with a palsy of the seventh cranial nerve, except
a. epiphora.
b. keratitis.
c. ectropion.
d. ptosis.
110. An image of a right orbit is shown below. There are two numbered sites. Which of the following series correctly pairs the number with the correct bones of the orbit?
a. (1) zygomatic bone, (2) greater wing of the sphenoid bone.
b. (1) greater wing of the sphenoid bone, (2) lesser wing of the sphenoid bone.
c. (1) zygomatic bone, (2) ethmoid bone.
d. (1) maxillary bone, (2) greater wing of the sphenoid bone.
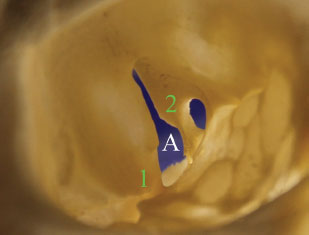
111. An image of a right orbit is shown in question 110. All of the following structures pass through the space depicted by the letter A, except
a. sympathetic nerve fibers.
b. superior ophthalmic vein.
c. trochlear nerve.
d. zygomatic nerve.
112. Which sinus system aerates first?
a. maxillary.
b. frontal.
c. sphenoid.
d. ethmoid.
113. The most common sinus lesion that invades the orbit is the
a. osteoma.
b. inverted papilloma.
c. mucocele.
d. squamous cell carcinoma.
114. The medial aspect of a left orbit is shown below. What bone is depicted by number (1) and what structure originates from the point shown by number (2)?
a. (1) lacrimal bone, (2) medial canthal tendon.
b. (1) lacrimal bone, (2) inferior oblique muscle.
c. (1) maxillary bone, (2) inferior oblique muscle.
d. (1) maxillary bone, (2) medial canthal tendon.

115. What tissue plane is the temporal branch of the facial nerve located in superior to the zygomatic arch?
a. deep temporal fascia.
b. loose areolar tissue.
c. subcutaneous tissue.
d. temporoparietal fascia.
116. The normal upper eyelid cross-sectional anatomy from the left orbit of a Caucasian cadaver is shown below. The presence of what lettered structure when clinically evaluating a patient with an eyelid laceration should raise the suspicion of a concomitant corneoscleral laceration?
a. structure A.
b. structure B.
c. structure C.
d. structure D.
117. All of the following surgeries may be performed by making an incision at the site of the green asterisk in the image from question 116, except
a. blepharoplasty.
b. internal blepharoptosis repair.
c. lateral orbitotomy.
d. optic nerve sheath fenestration.
118. All of the following are true regarding the levator palpebrae superioris, except
a. It runs from the posterior lacrimal crest medially to the lateral orbital tubercle laterally.
b. Its superficial portion inserts into the orbicularis muscle and subcutaneous tissues.
c. It originates in close proximity to the superior rectus origin, just above the annulus of Zinn.
d. The muscular portion is shorter than the aponeurotic portion.
119. The structure that gives rise to the gray line of the eyelid margin is best represented by
a. meibomian glands.
b. tarsal border.
c. mucocutaneous junction.
d. orbicularis muscle.
120. The capsulopalpebral fascia is analogous to which upper eyelid structure?
a. levator aponeurosis.
b. orbital septum.
c. superior transverse ligament.
d. Müller’s muscle.
121. The normal horizontal extent of the human palpebral fissure is approximately
a. 20 mm.
b. 25 mm.
c. 30 mm.
d. 35 mm.
122. The most likely outcome following inadvertent suturing of the orbital septum into subcutaneous tissues while repairing a partial-thickness eyelid laceration is
a. ectropion.
b. lid retraction in downgaze.
c. entropion.
d. blepharoptosis.
123. All of the following are characteristic of features of blepharochalasis, except
a. lacrimal gland atrophy.
b. excess eyelid skin.
c. blepharoptosis.
d. blepharophimosis.
124. What is the treatment of choice for a patient with an optic nerve sheath meningioma confined to the orbit and with progressive visual loss?
a. observation.
b. surgical excision.
c. chemotherapy.
d. radiation therapy.
125. An 86-year-old patient presents with left eye proptosis, diplopia, and a subconjunctival lesion photographed at the top of the right column. Which of the following is the most appropriate next step?
a. biopsy.
b. B-scan ultrasonography.
c. corticosteroids.
d. orbital imaging.

126. A 7-year-old boy presents with a 3-day history of progressive proptosis, injection, and pain of the left eye. He is systemically well with normal temperature. White blood cell count is normal, and emergent orbital CT scanning reveals superonasal orbital infiltration with bony erosion. The most likely diagnosis at this point is
a. frontal sinus mucocele.
b. rhabdomyosarcoma.
c. bacterial orbital cellulitis.
d. optic nerve glioma.
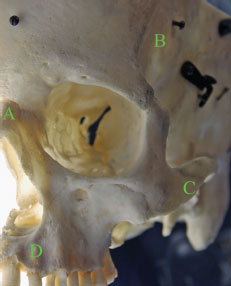
127. An image of a skull centered on the left orbit is shown below. What lettered location indicates a bone that is not part of the orbit?
a. location A.
b. location B.
c. location C.
d. location D.
128. Which one of the following histiocytic disorders is most likely to involve orbital bone?
a. sinus histiocytosis.
b. Hand-Schüller-Christian disease.
c. Letterer-Siwe disease.
d. eosinophilic granuloma.
129. Which of the following is one of the most common mesenchymal tumor of the orbit?
a. hemangiopericytoma.
b. fibrous histiocytoma.
c. osteogenic sarcoma.
d. ossifying fibroma.
130. The most common site of a primary tumor metastatic to the orbit in men is
a. lung.
b. colon.
c. prostate.
d. melanoma.
131. All of the following conditions may present with epiphora secondary to impaired blink function (abnormal blink), except
a. Sjögren’s syndrome.
b. Parkinson’s disease.
c. scleroderma.
d. progressive supranuclear palsy.
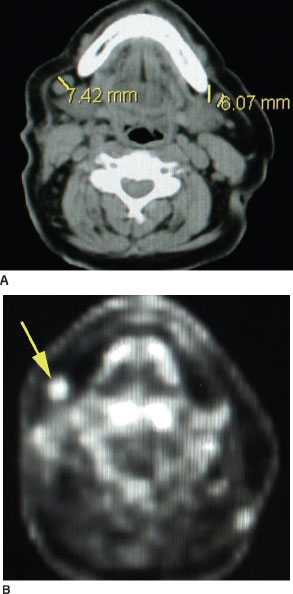
132. A patient with biopsy-proven sebaceous carcinoma of the eyelid presents with positive lymphadenopathy, as seen on PET-CT scans at the top of the right column. Based on both the most likely eyelid affected by sebaceous carcinoma and the involved node, which of the following is most likely to be the location of this patient’s eyelid neoplasm?
a. medial, lower eyelid.
b. lateral, lower eyelid.
c. medial, upper eyelid.
d. lateral, upper eyelid.
133. Components in the evaluation of corneal protective mechanisms prior to ptosis surgery include all of the following, except
a. examination for lagophthalmos.
b. Jones (primary dye) testing.
c. assessment of Bell’s phenomenon.
d. evaluation of corneal sensation.
134. The primary abnormality seen in simple congenital ptosis is in the
a. levator muscle.
b. levator aponeurosis.
c. levator innervation.
d. Müller’s muscle.
135. The primary abnormality seen in ptosis after cataract surgery is in the
a. levator aponeurosis.
b. Müller’s muscle.
c. levator innervation.
d. levator muscle.
136. The procedure of choice in a patient with ptosis following cataract surgery (good levator function and a high or effaced upper eyelid crease) would be
a. levator muscle resection.
b. unilateral frontalis suspension.
c. Müller’s muscle resection.
d. reinsertion of levator aponeurosis.
137. A patient is referred for surgical repair of the bilateral eyelid condition shown in the image below. On examination, he has papillary conjunctivitis and an upper eyelid margin reflex distance (MRD1) of 1 mm bilaterally. What effect will full thickness wedge resection (FTWR) to tighten the eyelids horizontally most likely have on the height of the upper eyelids?
a. A FTWR will slightly raise the eyelid.
b. A FTWR is not expected to affect the eyelid position.
c. A FTWR will slightly lower the eyelid.
d. A FTWR will cause eyelid retraction.

138. Which of the following is characteristic of the histopathology of the eyelid condition shown in question 137?
a. decrease in tarsal elastin fibers.
b. decrease in conjunctival inflammation.
c. decrease in tarsal collagen type I.
d. decrease in tarsal collagen type III.
139. Which of the following extraocular muscles is least likely to be injured during upper or lower blepharoplasty?
a. inferior oblique.
b. inferior rectus.
c. superior oblique.
d. superior rectus.
140. The most significant complication of blepharoplasty is
a. orbital hemorrhage.
b. diplopia.
c. overcorrection.
d. cellulitis.
141. The most common cause of indirect traumatic optic neuropathy is blunt trauma to which bone?
a. maxillary.
b. zygomatic.
c. frontal.
d. temporal.
142. What percentage of tear loss is evaporative in nature in young and elderly patients, respectively?
a. 5% and 10%.
b. 10% and 20%.
c. 15% and 30%.
d. 20% and 40%.
143. Which of the following is least likely to be associated with a zygomaticomaxillary complex (ZMC) fracture?
a. inferior rectus entrapment.
b. trismus.
c. globe ptosis.
d. lateral canthal dystopia.
144. Besides pharmacologic testing with edropho-nium chloride (Tensilon), which of the following is another clinical test specifically used in diagnosing myasthenia gravis (MG)?
a. exercise stress test.
b. ice pack test.
c. thyroid-stimulating hormone (TSH) receptor antibody test.
d. three-step test.
145. An 11-year-old patient in the figures below presents gradually increasing proptosis of the right eye. Based on patient’s most likely diagnosis, which one of the following clinical features would be considered inconsistent with the diagnosis?
a. unilaterality.
b. insidious onset.
c. afferent pupillary defect.
d. pain.
146. The systemic evaluation of a patient with biopsy-proven orbital lymphoma generally includes all of the following except
a. lumbar puncture.
b. bone scan.
c. serum immunoelectrophoresis.
d. bone marrow biopsy.
147. Which of the following answers would be the best treatment option for a localized orbital lymphoproliferative lesion?
a. radiation and systemic corticosteroids.
b. radiation therapy alone.
c. surgical excision combined with chemotherapy.
d. surgical excision combined with radiation.
148. A 5-month-old baby is seen in consultation for the condition shown below. All of the following characteristic of this condition, except
a. autosomal dominant.
b. lower eyelid entropion.
c. lop ears.
d. hypoplasia of the superior orbital rims.

149. A patient undergoes placement of hard palate graft for lower eyelid retraction. Which of the following best characterizes the epithelium of the graft?
a. retention of native epithelium.
b. metaplasia into nonkeratinized epithelium.
c. survival of submucosal glands.
d. conjunctivalization of epithelium.
150. A 73-year-old patient in the photograph below is referred in consultation for chronic left eye irritation. He has a snap back test of greater than 6 mm and normal palpebral and forniceal conjunctiva. Based on the patient’s diagnosis, all of the following are true statements regarding the patient’s diagnosis, except
a. no inferior movement of lower eyelid during downgaze.
b. deeper than usual inferior fornix.
c. presence of a white subconjunctival line below the inferior tarsal border.
d. lower than normal position of lower eyelid.
 Answers
Answers1. c. A superficially placed gold weight implant (GWI) is shown in the figure. The concern is that the implant may become exposed. The GWI is commonly placed in a pretarsal location underneath the orbicularis oculi muscle, rather than directly underneath the surface of the skin.
2. c. The periocular concerns of patients with facial nerve palsy include lagophthalmos, paralytic ectropion, and eyebrow ptosis, which are addressed surgically by choices a, b, and d, respectively. Blepharoplasty to correct dermatochalasis is unrelated to the patient’s condition.
3. b. Choices a and d describe potential serious side effects. Other major side effects of edrophonium include bradycardia, bronchospasm, and cholinergic crisis. Besides choice c, a number of minor side effects may occur such as nausea, diaphoresis, salivation, abdominal cramping, and lacrimation.
4. c. A CT scan of the chest is appropriate to rule out thymoma, which occurs in about 10% of patients with MG. Conversely, about a third of patients with a thymoma have MG.
5. a. The lesion shown is classic-appearing example of a keratoacanthoma (KA). KA characteristically erupts rapidly and is considered a subtype of squamous cell carcinoma. The central crater is keratin filled. Of note, KA associated with sebaceous neoplasms may occur as part of the Muir-Torre syndrome (visceral malignancy).
6. a. Marcus Gunn jaw-winking ptosis results from synkinesis of the third and fifth (motor division) cranial nerves.
7. b. Eyelid synkinesis is associated with choices a, c, and d. While not considered synkinesis, a brief eyelid twitch, lasting seconds, may occur in a patient with ocular myasthenia gravis. The twitch, known as Cogan lid-twitch, may be seen when the patient looks from down to upgaze.
8. c. The patient has an age, history, and external examination consistent with involutional ptosis. The patient shown also has dermatochalasis. Involutional ptosis is characterized by normal levator function and a high eyelid crease. In contrast to pediatric ptosis, which exhibits lid lag, involutional ptosis worsens in the reading (downgaze) position. The supratarsal tissues are thinned. Dehiscence of the levator aponeurosis is the most commonly accepted mechanism for ptosis following cataract and other eye surgeries.
9. d. The patient has rhabdomyosarcoma. Incisional biopsy is necessary for making the diagnosis. If the tumor can be safely removed at the time of surgery, then excisional biopsy is more appropriate. Observation does not have a role in this patient’s care. Chemotherapy is used to treat the condition once the diagnosis has been made. Bone marrow biopsy may be coordinated to coincide with biopsy of the orbital mass.
10. b. The gross examination shown is of an exenteration specimen of a patient with sebaceous carcinoma. The appropriate management of primary orbital rhabdomyosarcoma involves radiation therapy and systemic chemotherapy. Although historically, rhabdomyosarcoma was treated with exenteration, currently, such surgery is used only in recurrent cases.
11. d. Choices a–c are related to adenoid cystic carcinoma. Both benign mixed tumor (pleomorphic adenoma) and adenoid cystic carcinoma tend to occur in middle-aged patients.
12. a. Bony remodeling (fossa formation) occurs in benign mixed tumor due to its gradual growth pattern. Bony erosion is seen with infiltrative lesion such as adenoid cystic carcinoma. Lymphoid tumors tend to conform to the shape of the surrounding structures.
13. a. The peripheral arterial arcade lies just above the superior tarsal border between the levator aponeurosis and Müller’s muscle. It is a distinct structure from the marginal arcade, which lies on the tarsal surface of each eyelid margin.
14. c. Lacrimal sac distention above the medical canthal tendon raises the suspicion of a lacrimal malignancy in adults and an encephalocoele in newborn patients, respectively.
15. b. The nasolacrimal drains inferiorly and runs slightly lateral and posterior.
16. c. The patient has a cicatricial ectropion. Choices a, b, and d are appropriate aspects of the surgical management of the condition. Eyelid retractor repair is an important component in the repair of involutional entropion and occasionally involutional ectropion.
17. c. The proptosis of optic nerve sheath meningioma is usually axial. Lacrimal gland malignancies may produce proptosis, which is typically down and medial. Maxillary sinus tumors typically push the eye superiorly.
18. a. The history of proptosis due to benign mixed tumor of the lacrimal gland (pleomorphic adenoma) is characteristically greater than 6 to 12 months.
19. d. The patient’s raised pearly lesion with overlying telangiectatic vessels and madarosis is typical of nodular basal cell carcinoma. Once the diagnosis is confirmed by incisional biopsy, a more invasive full-thickness wedge resection (excisional biopsy) may be undertaken.
20. d. Choices a–c are true of botulinum toxin type B. It is type A that has a longer duration of action.
21. c. Hemifacial spasm is rarely bilateral and is usually due to vascular compression of the seventh cranial nerve at the brainstem and can result in synchronous contractions of the entire side of the face. Along with partial complex seizures and myoclonic epilepsy, essential blepharospasm is effaced by sleep.
22. b. The long-term use of hard contact lenses has been associated with acquired aponeurotic ptosis due to repetitive traction. Involutional attenuation is an age-related condition also associated with dehiscence of the levator aponeurosis. Levator muscle dysgenesis is seen in congenital ptosis. Myogenic ptosis occurs in muscular diseases such as myasthenia gravis, muscular dystrophy, ocu-lopharyngial dystrophy, and chronic progressive external ophthalmoplegia.
23. d. Orbital cellulitis is the most common cause of unilateral proptosis in children. Thyroid eye disease is the most common cause of both unilateral and bilateral proptosis in adults.
24. d. A bluish bulge above the medial canthal tendon is typically a meningocele, whereas one below is typically a dacryocele.
25. c. The patient has a direct (high-flow) carotid cavernous (CC) sinus fistula. Indirect (low-flow) dural cavernous fistulas tend to occur in elderly women, whereas the direct dural cavernous fistulas occur after a basal skull fracture. Arteriography is used to differentiate between the two types of fistula. A cranial bruit is characteristic of a direct CC fistula. Extraocular muscle enlargement may occur due to orbital congestion.
26. b. This is a classic presentation of a cavernous sinus wall–dural shunt, featuring lower arterial flow and an insidious onset.
27. d. The orbits of patients with craniosynostoses are usually shallow and small, with resultant proptosis and exposure. V-pattern exotropia is also common.
28. b. Choices a, c, and d are risk factors for orbital cellulitis. Recent skin trauma is the most common risk factor for preseptal cellulitis.
29. a. Breast cancer is the most common primary source of metastases to the orbit in women. Hormone therapy is used in estrogen-receptor– positive tumors. Extraocular involvement is more common than bony involvement. Although the scirrhous subtype can present with enophthalmos, the majority of patients with metastatic breast cancer present with proptosis. Clinically, the patient in this case had 7 mm of proptosis in the left eye, which is consistent with the radio-graphic appearance of the space occupying mass lesion.
30. c. The patient has complete left upper eyelid ptosis and compensatory right upper eyelid retraction (Hering’s law).
31. b. The patient has a capillary hemangioma, which is causing mechanical ptosis. Although the lesion may involute over time, deprivation amblyopia is an urgent concern in the management of this patient and thus early treatment is warranted.
32. a. Choices b–d have been used in the treatment of capillary hemangioma. Intralesional steroid injection is often the first line approach. However, the use of propranolol is an area of active evolution in the treatment of patients with capillary hemangioma.
33. c. Kasabach-Merritt syndrome is a platelet sequestration disorder associated with multiple large capillary hemangiomas, which results in thrombocytopenia.
34. a. Cavernous sinus thrombosis is one of the most dreaded complications of orbital cellulitis, with a significant increase in systemic morbidity and mortality.
35. a. Telecanthus is defined as an abnormally large distance between medial canthi, regardless of intraorbital distance. Telecanthus and rounding of the medial canthus are characteristic findings in direct naso-orbital-ethmoid fractures.
36. c. Orbital floor fractures usually produce vertical limitations of gaze. Global motility deficits generally indicate blunt trauma with muscle and/or nerve contusion.
37. d. The images show a fracture of the right orbital roof (the most common orbital fracture in young children). The lack of a pneumatized frontal sinus predisposes the early childhood age group to roof fractures. Choice c is incorrect in that the injury can occur in a fall from a height of less than 10 ft. Choice d is characteristic clinical finding associated with roof fractures. Treatment is indicated only for significantly displaced roof fractures; a multidisciplinary approach works best for the minority of patients that require surgery.
38. d. Choices a–c, as well as scirrhous breast carcinoma, are associated with enophthalmos. In contrast, malar hypoplasia may create an appearance of proptosis (relative exophthalmos).
39. d. The nevus flammeus (port-wine stain) is a cavernous hemangioma of the dermis. It can be seen in Sturge-Weber syndrome, Klippel-Trénaunay-Weber syndrome, and as an idiopathic finding. Some pathology references also refer to the lesion as a dermal telangiectasia.
40. a. Although not usually present at birth, the majority of capillary hemangiomas become apparent within the first several weeks of life.
41. b. Capillary hemangiomas generally start to involute spontaneously by 12 months of age. 40% of tumors completely regress by age 4. 80% of tumors completely regress by age 8.
42. b. Capillary hemangiomata will blanch with pressure, whereas the nevus flammeus does not. There is considerable overlap between the other features listed.
43. c. Choice correctly identifies the approximate percentages of the different patients with the thyroid eye disease.
44. c. The enlargement generally features smooth contours. Although sometimes only a single muscle is enlarged, this should be considered an atypical finding.
45. d. Eyelid retraction is the most commonly occurring eyelid finding in patients with Graves’ oph-thalmopathy (seen in about 38% of patients). Von Graefe’s sign, lagophthalmos, and lid lag occur in about 36%, 16%, and 8% of patients with Graves’ ophthalmopathy, respectively.
46. c. Waiting for a period of 6 months allows adequate time for stability of the condition to be established, allowing for a more predictable outcome.
47. d. Preoperative and intraoperative images of a patient who underwent evisceration surgery are shown. The cornea should be removed in cases of active corneal disease. Choices a–c are correct.
48. c. A superior sulcus deformity results from inadequate volume replacement when the eye is removed from the orbit.
49. a. The patient has choroidal melanoma. The intraocular mass (with characteristic low internal reflectivity) is seen on the ultrasound examination. Removal of the eye is the most appropriate treatment. Evisceration should never be performed in the presence of an intraocular mass.
50. b. Alveolar rhabdomyosarcoma has a predilection for the inferior orbit. The embryonal variant is more common superonasally. Metastatic workup includes lumbar puncture and bone marrow biopsy, best done under anesthesia.
51. b. Dysplasia or aplasia of the sphenoid bone creates large posterior orbital defects. This leads to pulsating exophthalmos, as brain tissue herniates outward.
52. d. Orbital phycomycosis generally results from invasion by necrotizing fungal sinusitis. Black eschar in the nasal cavity is virtually diagnostic, but is a late finding. (Its absence does not exclude the diagnosis.)
53. b. Acanthosis nigricans is associated with internal malignancy but not transformation. Actinic keratosis is the most common premalignant skin lesion. It is related to ultraviolet (UV) exposure and may develop into squamous cell carcinoma. Although actinic keratoses resolve spontaneously within a year in up to 25% of cases, patients with multiple actinic keratoses have a 12% to 16% risk of developing squamous cell carcinoma.
54. a. Suddenly appearing multiple seborrheic keratoses may in fact be evolving acanthosis nigricans. This is known as the Leser-Trélat sign and is usually associated with a GI malignancy.
55. a. Anti-herpetic medication is given to patients. Oral antibiotic medication is also often prescribed preoperatively.
56. a. Use of isotretinoin (Accutane) within the preceding 12 months is a contraindication for laser skin resurfacing due to impaired ability of reepithelialization.
57. b. Suborbicularis oculi fat (SOOF) elevation provides a youthful midface appearance. It is usually accessed through a transconjunctival or subciliary approach.
58. b. There may be multicentric foci of tumor with skip areas. Negative margins do not necessarily imply complete excision of the tumor. Wide surgical margins should be used, with map biopsies taken over the area surrounding the lesion.
59. d. Cryotherapy selectively destroys melanocytes but is insufficient for cutaneous melanoma and should be considered a palliative treatment.
60. b. A patient with a pilomatricoma of the central, left upper eyelid is shown. The lesion has a characteristic histopathologic appearance (includes shadow cells), which is described in the question stem. It is classified as a benign tumor of hair follicle (i.e., skin adnexal, rather than epithelial) origin. Clinically, the lesion can be mistaken for a cyst.
61. d. Changes in corneal sensation may occur, but frank ulceration—especially peripherally—is unusual.
62. c. Bilateral presentation of orbital pseudotumor is more common in children (occurs in about one-third of cases). Choices a, b, and d are true.
63. c. Sarcoidosis is generally not associated with pain and usually spares orbital soft tissues.
64. a. All Le Fort fractures by definition must involve the pterygoid plates. The Le Fort I fracture is the only one of the three that does not involve the orbit. In actuality, mixed presentations of the three types frequently occur.
65. c. Two weeks provides a chance for orbital swelling and “contusion diplopia” to resolve and yet is early enough to avoid problems with scarring of a significant floor fracture.
66. a. The patient has basal cell carcinoma invasive to the orbit. Exenteration is an appropriate treatment strategy, as long as the tumor has not invaded too deeply that complete resection is not possible.
67. d. The patient has a canalicular laceration. Canalicular involvement should be suspected in any eyelid laceration medial to the corneal limbus. Direct suturing of the ends in not required; however, stenting is necessary. Canalicular stents are ideally left in place for 3 to 6 months (not weeks). While irrigation with fluorescein can be helpful to localize the cut ends of the canaliculus, methylene blue is not recommended as it stains the whole surgical field.
68. a. The trochlea is the only cartilaginous structure in the normal orbit.
69. b. Rituximab is a monoclonal antibody that targets the B cell CD20 receptor.
70. c. About half of newborns are born with an imperforate valve of Hasner. Most (>90%) congenital nasolacrimal duct obstructions resolve within the first 12 months of life.
71. c. The sphenopalatine ganglion receives parasympathetic fibers from the greater superficial petrosal nerve (a division of CN VII).
72. d. Tear production commences by the first 6 weeks of life.
73. c. Benign mixed tumor (pleomorphic adenoma) is the most common lacrimal gland neoplasm.
74. a. Adenoid cystic carcinoma is the most common malignant neoplasm of the lacrimal gland. A
75. d. The levator aponeurosis divides the lacrimal gland into palpebral and orbital lobes.
76. a. The most likely diagnosis is that of benign mixed cell tumor. The male–female ratio is 3:2. The tumor should be approached through a lateral orbitotomy with careful excision to avoid rupture of the tumor’s pseudocapsule. Incisional or incomplete biopsy techniques can lead to infiltrative tumor recurrence and, occasionally, malignant transformation.
77. a. An encephalocele is not associated with reflex hypersecretion.
78. c. A dermoid cyst is an example of a choristoma. The lesion is lined by keratinizing epithelium. The condition most commonly occurs at the lateral brow at the frontozygomatic suture. The superonasal location (e.g., the frontolacrimal and frontoethmoidal sutures) is the next most common location. An eyelid crease incision is frequently used to provide surgical access (including in the patient shown).
79. b. When ocular or optic disc perfusion is severely compromised by an orbital compartment syndrome, immediate canthotomy with cantholysis should be performed to decompress the orbit.
80. a. In cases where the ocular examination suggests optic nerve trauma (afferent pupillary defect, poor vision), neuroimaging is indicated to rule out direct optic nerve injury (e.g., optic canal fracture).
81. d. Reattachment of the posterior crus of the medial canthal tendon to the posterior lacrimal crest is necessary for reconstruction of the normal eyelid contour at the medial canthus. In the setting of a fracture, either transnasal wiring or Y-shaped miniplate fixation is required.
82. c. Traumatic ptosis is repaired after 6 months of observation. Ptosis repair prior to the possible spontaneous return of function may lead to lagophthalmos.
83. c. The intraorbital portion of the optic nerve measures about 28 to 30 mm in length. The avulsed globe shown in the figure has a 32 mm segment of optic nerve attached. Thus the avulsion has occurred at the intracanalicular portion (note in the figure the last 2 mm appear slightly different).
84. b. The patient has an orbital hemorrhage associated with the inferior rectus muscle. The condition may occur spontaneously and complete resolve without intervention. In cases without optic neuropathy, observation is advised. The patient presented has decreased vision and surgical drainage is recommended.
85. b. Primary amenorrhea is the most common condition associated with blepharophimosis.
86. c. A patient has a cavernous hemangioma, which is an encapsulated tumor. Choices a, b, and d are also encapsulated tumors. Lymphangioma, however, is not encapsulated.
87. c. Both types are ectopic epithelial rests created by aberrant “pinching off “ in utero. The variety that is silent until adulthood is generally intraorbital (retroseptal).
88. c. Dermoid cysts are often adherent to suture lines; the frontozygomatic suture (marked location C) is the most common location. Anterior cysts also occur along the frontolacrimal and frontoethmoidal sutures.
89. d. The arrow marks the lateral orbital tubercle of Whitnall, which is a palpable structure about 11 mm below the frontozygomatic suture. In addition to Choices a–c, the lateral canthal tendon and the check ligament of the lateral rectus muscle also attach to Whitnall’s tubercle. Other attached structures include the deep pretarsal orbicularis insertion and an expansion of the superior rectus muscle sheath. During horizontal eyelid tightening surgery (e.g., lateral tarsal strip) the lateral eyelid is reattached to the tubercle.
90. b. The patient has a cavernous hemangioma (CH). The growth of CH may accelerate during pregnancy. CH may exert pressure on the globe (raising intraocular pressure) and optic nerve, leading to glaucomatous and compressive optic neuropathies, respectively. Pressure on the globe can cause hyperopic shift (posterior displacement of the far point of the eye). CT scan may demonstrate radiodense phleboliths in older lesions.
91. d. As described, the lesion is a CH, which generally have high (especially the capsule) reflectively on A-scan.
92. b. The levator function (also known as eyelid excursion) is the critical measurement in guiding the type of ptosis surgery to perform.
93. a. Choice a indicates the correct order of the anatomic structures encountered.
94. c. Choices a, b, and d can commonly present bilaterally.
95. c. The distance is 2 mm down (ampulla), then 8 mm across (canaliculus).
96. d. Actinomyces israelii is most common bacterial cause of canaliculitis.
97. c. Docetaxel (Taxotere) is a chemotherapeutic agent used in the treatment of breast, ovarian, and nonsmall cell lung cancer. The drug is secreted in the tear film and can cause canalicular stenosis. Doxorubicin (Adriamycin) is also a chemotherapeutic agent that is known for cardiac side effects but does not lead to canalicular stenosis. Choices a, b, and d may cause canalicu-lar stenosis.
98. c. The canaliculi are lined by stratified squamous epithelium.
99. b. The total length of the infant nasolacrimal system measures about 20 mm.
100. d. Besides the 10 mm distance from lacrimal punctum to sac, the length of the lacrimal sac and nasolacrimal duct adds another 20 to 25 mm. Thus in adults, the total length is 30 mm from lacrimal punctum to inferior meatus.
101. c. The Jones tests are not often performed in the clinical setting. Lacrimal irrigation is most commonly performed in the evaluation of epiphora.
102. d. The Jones I test consists of placing 2% fluorescein in the conjunctival fornices and attempting to recover fluorescein with a swab at the inferior meatus. Unfortunately, one-third of normal patients will have abnormal results with this test.
103. d. The Jones II test is performed after a dye disappearance test or after Jones I indicates blockage. The fornix is irrigated, and the lacrimal sac cannulated and irrigated. If dye is recovered in the inferior meatus, then incomplete blockage of the nasolacrimal duct, patent upper system, and functioning lacrimal pump is indicated. However, if only clear fluid is recovered, then a nonfunctioning lacrimal pump or blocked upper system is indicated.
104. b. The initial management of a patient with acute dacryocystitis includes broad-spectrum antibiotics. Dacryocystorhinostomy is performed once the initial inflammation subsides. Probing does not have a role in the management of adult nasolacrimal disorders. Canalicular irrigation is a treatment for canaliculitis.
105. d. Strictures, narrow or long ducts, and nasal and sinus inflammatory disease may cause tear stasis and lead to acute dacryocystitis.
106. a. The lacrimal and maxillary bones are invariably removed. In some cases, removal of anterior ethmoid air cells is performed to provide access to the lacrimal sac fossa. The nasal bone is not removed.
107. c. This is the ocular equivalent of a kidney stone.
108. a. In congenital obstruction, the blockage is at the valve of Hasner. In acquired cases, the blockage is within the intraosseous nasolacrimal duct. Involutional stenosis is one of the most common causes of acquired nasolacrimal duct obstruction.
109. d. Choices a–c occur with facial nerve palsy. Such patients have impaired eye closure (lag-ophthalmos), not eyelid ptosis.
110. b. The two wings of the sphenoid bone are marked. The two parts: (1) greater wing and (2) lesser wing are correctly labeled in choice b. The sphenoid bone makes up part of the orbital roof and lateral and medial walls of the orbit.
111. d. The marked space (A) is the superior orbital fissure. Choices a–c pass through the superior orbital fissure.
112. a. The maxillary sinus aerates first.
113. c. The most common sinus lesion to invade the orbit is mucocele. The most common neoplasm to invade the orbit is squamous cell carcinoma.
114. c. The lacrimal sac fossa, including the suture line separating the lacrimal and maxillary bones, is shown. The thinner lacrimal bone is seen to the right of the 1. The anterior process of the maxilla is marked (1). Lateral to the fossa, just inside the inferior orbital rim, is the origin (2) of the inferior oblique muscle. The medial canthal tendon attaches to the anterior and posterior crests of the lacrimal sac fossa.
115. d. The temporal branch of the facial nerve runs superficially (in the temporoparietal fascia) superior to the zygomatic arch.
116. b. The labeled structures are as follows: (A) brow fat, (B) preaponeurotic fat, (C) preseptal orbicularis muscle, and (D) pretarsal orbicularis muscle. A complete eye examination is important in all ocular and periocular trauma. Moreover, an eyelid laceration with visible adipose tissue present, specifically fat from the orbit, should raise concern for the possibility of injury to the globe.
117. b. The eyelid crease is marked by the asterisk. The crease occurs at the superior tarsal border in Caucasians. Choices a, c, and d may all be performed through an eyelid crease incision. Choice b is performed through the posterior approach by everting the eyelid.
118. d. The muscular portion is longer than the aponeurotic portion.
119. d. The gray line is an isolated bundle of pretarsal orbicularis muscle also known as the muscle of Riolan.
120. a. The capsulopalpebral fascia is analogous to the levator aponeurosis.
121. c. The normal adult palpebral fissure is 27 to 30 mm horizontally and 8 to 11 mm vertically.
122. b. The patient will have a deficiency of the middle lamella. Incorporation of the orbital septum will lead to lid retraction in downgaze.
123. a. The term blepharochalasis is sometimes confused with dermatochalasis. Blepharochalasis, a rare disorder, is considered a familial type of angioneurotic edema. The condition, characterized by repeated bouts of painless eyelid edema, often presents in children and adolescents. Patients may have prolapse (not atrophy) of the lacrimal gland. Other features include lower eyelid retraction, pseudoepicanthal folds, proptosis, blepharoptosis, blepharophimosis, and atrophic wrinkled excess eyelid skin.
124. d. The tumor may be observed unless there is loss of vision, in which case radiation therapy is advisable.
125. d. A salmon patch subconjunctival lesion is shown. The presence of proptosis and diplopia warrant imaging for an orbital mass, which was present in this patient with orbital lymphoma.
126. b. Orbital cellulitis does not usually cause bony erosion. In addition, the white blood cell count and temperature would be expected to be elevated (unless the child were immunocompromised). Mucocele and glioma are not typically so inflammatory. Rhabdomyosarcoma responds well to treatment and should be promptly diagnosed.
127. a. The labeled bones are as follows: (A) nasal, (B) frontal, (C) zygomatic, and (D) maxillary. The nasal bone is not part of the orbit. The adjacent frontal process of the maxilla lies just to the right of the nasal bone in the figure.
128. d. Eosinophilic granuloma frequently involves the orbital bones. The classic triad of Hand-Schüller-Christian disease consists of proptosis, lytic skull lesions, and diabetes insipidus. Orbital involvement is rare in Letterer-Siwe disease. Prior characterization of histiocytic disorders using these terms is being replaced by the terms diffuse soft tissue histiocytosis and unifocal/ multifocal eosinophilic granuloma of bone.
129. b. Most fibrous histiocytoma are benign (more than 90%), and have a storiform, or matlike, pattern on histopathology. The lesion is usually very firm and can displace other orbital structures.
130. a. An orbital metastasis is more likely to be the mode of presentation for bronchogenic carcinoma than for a breast primary.
131. a. A normal blink is necessary for the pump function of the lacrimal drainage system to work. Choices b–d are conditions with impaired blink function. Sjögren’s syndrome causes a dry eye state.
132. c. The PET-CT scans show a positive submandibular node. The medial eyelid lymphatics drain to the submandibular nodes. In contrast, the lateral eyelid lymphatics drain to the preau-ricular nodes. Sebaceous carcinoma most commonly involves the upper eyelid. The patient shown had a sebaceous carcinoma of the medial right upper eyelid with regional spread to the submandibular nodes.
133. b. Jones testing will give information regarding patency of the lacrimal drainage system. Patients with positive Jones tests will have difficulties with epiphora, which can usually be managed independently.
134. a. Congenital myogenic ptosis results from a maldevelopment of the levator muscle.
135. a. Aponeurotic dehiscence has been blamed on anesthetic injections, lid specula, and bridle sutures. The exact cause is not clear.
136. d. Reinsertion of the levator aponeurosis would best correct the underlying anatomic defect.
137. a. The patient has floppy eyelid syndrome. Unlike in patients without eyelid laxity, patients with eyelid laxity tend to experience a slight elevation in the eyelid height after FTWR.
138. a. There is a decrease in tarsal elastin fibers.
139. d. The inferior rectus and inferior oblique are at risk during lower blepharoplasty The superior oblique is at risk during upper blepharoplasty during excision of nasal fat.
140. a. Injury to orbital fat pads, vessels, or orbicularis may result in retrobulbar hemorrhage that dissects into the posterior orbit and compresses the optic nerve.
141. c. Blunt trauma to the frontal bone is the usual mechanism by which indirect traumatic optic neuropathy occurs.
142. b. Children have less evaporative tear loss than older individuals, 10% and 20%, respectively.
143. a. A ZMC fracture may involve the orbital floor; however, inferior rectus muscle entrapment is not common. Choices b–d may commonly occur.
144. b. The ice pack test is used in diagnosing MG. Testing for MG after exercise may help in confirming a positive result; however, this is not the same as the exercise stress testing, which is used as a method of screening for cardiac health. The three-step test is used for vertical strabismus. Due to the relatively nonspecific patterns of extraocular motility dysfunction in MG, the test has no role in the confirming a diagnosis of MG The acetylcholine-receptor antibody test is related to MG, in that elevated serum values are seen in about 50% to 70% of patients with ocular MG and in 90% of those with systemic MG. Although about 5% of patients with MG. also have thyroid eye disease, the TSH-receptor antibody test is not used to diagnose MG.
145. d. The patient has an optic nerve glioma. Choices a–c are considered typical. Pain would be unusual.
146. a. The central nervous system (CNS) is not routinely surveyed in patients with orbital lym-phoma. This is in distinction to patients with intraocular lymphoma. When CNS involvement is suspected, CT or MRI is the starting point.
147. b. Surgical excision is not recommended, and neither are systemic corticosteroids. Radiation is the treatment of choice for these lesions.
148. b. The patient has blepharophimosis syndrome, an autosomal dominant disorder. The classic triad of epicanthus inversus, telecanthus, and ptosis are all seen in the photograph. Also seen is the characteristic poorly developed nasal bridge. The superior orbital rims are hypoplastic. This patient also had lop ears (cropped from the photograph). Patients with the syndrome may develop lateral lower eyelid ectropion due to anterior lamellar deficiency. Hypertelorism may also occur. Surgical correction must be individualized and may include ptosis repair (frontalis sling if poor levator function), Y- V plasty (or transnasal wiring), ectropion repair, and buildup of the hypoplastic orbital rims.
149. a. Full-thickness mucosal grafts have been shown to maintain their original epithelium after transplantation onto the ocular surface; however, submucosal glands typically do not survive.
150. d. The patient has involutional entropion. Choices a–c are true. In addition, the lower eyelid position is usually higher than normal due to the disinsertion of the lower eyelid retractors. Other features include overriding of the orbicularis oculi muscle, horizontal eyelid laxity, and (more recently) relative enophthalmos.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


