 Questions
Questions
1. At birth, the length of the average infant human eye is
a. 8 to 9 mm.
b. 12 to 13 mm.
c. 16 to 17 mm.
d. 20 to 21 mm.
2. The factor primarily responsible for the shallow anterior chamber in a normal infant eye is:
a. The infant cornea is flatter than the adult cornea.
b. The infant iris is relatively thicker than the adult iris.
c. The infant lens is relatively thicker than the adult lens.
d. There is more positive vitreous pressure in the infant eye than in the adult eye.
3. The reason for relatively miotic pupils in infancy include
a. relative delay in sympathetic innervation of the eye.
b. excessive supranuclear input to the Edinger-Westphal nucleus.
c. increased sensitivity of the light-induced miosis reflex.
d. immaturity of the dilator pupillae muscle.
4. Which of the following gives the least amount of information in regard to estimating visual acuity in the preverbal child?
a. optokinetic nystagmus testing (OKN).
b. preferential looking testing (PLT).
c. visual evoked potentials (VEP).
d. electroretinography (ERG).
5. Congenital colobomas of the eyelids are associated with which systemic syndrome?
a. Goldenhar’s syndrome.
b. Pierre Robin’s syndrome.
c. Hallermann-Streiff syndrome.
d. Stickler’s syndrome.
6. Which of the following is true?
a. Both congenital ectropion and entropion involve the upper lid more frequently than the lower lid.
b. Like congenital entropion, distichiasis generally does not cause significant keratopathy.
c. There are three varieties of epicanthus: palpebralis, tarsalis, and inversus.
d. Telecanthus is synonymous with hypertelorism.
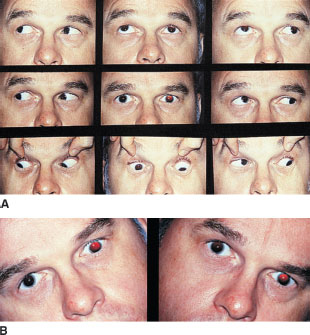
7. Which of the following is not part of the syndrome depicted in the photograph below?
a. simple epicanthus (palpebralis).
b. ptosis.
c. telecanthus.
d. lid phimosis.

8. Which of the following concerning congenital toxoplasmosis is true?
a. Fetal infection earlier in gestation generally results in less severe involvement.
b. The incidence of congenital toxoplasmo-sis, both symptomatic and asymptomatic, is approximately 1 in 10,000 live births.
c. A majority of pregnant women are seronegative (i.e., susceptible to infection).
d. When placental transfer occurs, the infant nearly always develops some obvious manifestation of the infection.
9. Which of the following is not a sign or symptom typical of congenital toxoplasmosis?
a. hepatosplenomegaly.
b. seizures with intracranial calcifications.
c. vomiting and diarrhea.
d. diffuse pigmentary retinopathy.
10. Which of the following medications is not important in the control of ocular toxoplasmosis?
a. folic acid.
b. pyrimethamine.
c. sulfadiazine.
d. prednisone.
11. Which of the following concerning the epidemiology of congenital rubella infection is true?
a. The majority of pregnant women are seronegative (susceptible to rubella infection).
b. Seroconversion of a mother from negative to positive nearly guarantees infection of the fetus.
c. Symptomatic fetal defects are uncommon, even with viremia.
d. Maternal infection during the third trimester rarely leads to fetal infection.
12. The most common clinical finding in infants with congenital rubella syndrome is
a. pigmentary retinopathy.
b. sensorineural hearing loss.
c. mental retardation.
d. cataract.
13. Which two signs of congenital rubella infection are unlikely to be found simultaneously?
a. microphthalmia and congenital cataract.
b. pigmentary retinopathy and congenital cataract.
c. congenital cataract and glaucoma.
d. congenital cataract and a poorly dilating iris.
14. The postoperative course following extraction of infantile cataract associated with the congenital rubella syndrome is distinguished by
a. a higher incidence of retinal detachment.
b. a higher incidence of glaucoma.
c. difficulty tolerating aphakic contact lenses.
d. severe inflammation.
15. The most common congenital infection in humans is
a. toxoplasmosis.
b. rubella.
c. cytomegalovirus (CMV).
d. herpes simplex virus (HSV).
16. The most common ocular manifestation of congenital CMV infection is
a. cataract.
b. microphthalmia.
c. retinochoroiditis.
d. strabismus.
17. Which of the following in regard to pediatric viral infections is true?
a. Most cases of congenital herpes simplex (HSV) infection are due to maternal viremia during gestation.
b. Most cases of congenital CMV infection are due to maternal viremia during gestation.
c. Like congenital CMV infection, congenital HSV infection is frequently asymptomatic.
d. The ocular manifestations of congenital HSV infection resemble those of acquired infections in adolescence and adulthood.
18. Which of the following microorganisms is generally transmitted through an infected birth canal as opposed to a transplacental route?
a. Toxoplasma.
b. CMV.
c. Treponema pallidum.
d. herpes simplex.
19. Hutchinson’s triad, considered diagnostic of congenital syphilis infection, includes
a. peg-shaped teeth, eighth nerve deafness, and interstitial keratitis.
b. rhagades, interstitial keratitis, and hepatosplenomegaly
c. pseudoretinitis pigmentosa, interstitial keratitis, and peg-shaped teeth.
d. pseudoretinitis pigmentosa, eighth nerve deafness, and interstitial keratitis.
20. Each of the following is a valid conclusion of the Multicenter Trial of Cryotherapy for Retinopathy of Prematurity except:
a. Treatment of threshold disease reduces the incidence of retinal detachment relative to no treatment.
b. Treatment of threshold disease reduces the incidence of blindness relative to no treatment.
c. Treatment of threshold disease results in better long-term Snellen acuity relative to no treatment.
d. Treatment benefit is independent of birth weight, race, and number of sectors of stage 3 involvement.
21. Which of the following is not considered a common etiologic agent for conjunctivitis in children?
a. Streptococcus pneumoniae.
b. Hemophilus influenzae.
c. Staphylococcus aureus.
d. Streptococcus pyogenes.
22. Which of the following viral infections is not associated with a pronounced keratitis?
a. herpes simplex (HSV).
b. adenovirus type 3.
c. adenovirus type 8.
d. herpes zoster.
23. Which of the following concerning Parinaud’s oculoglandular syndrome is not true?
a. Histopathology reveals nongranulomatous inflammation.
b. Common etiologic agents include the catscratch fever organism, rickettsiae, Treponema pallidum, and mycobacterial species.
c. Clinically, follicles are prominent with a moderate discharge.
d. Historical features may include contact with animals.
24. The agent most commonly responsible for preseptal cellulitis in children is
a. Staphylococcus aureus.
b. Pseudomonas aeruginosa.
c. Streptococcus pyogenes.
d. Haemophilus influenzae.
25. The agent most frequently associated with orbital cellulitis following bacterial conjunctivitis is
a. Staphylococcus aureus.
b. Pseudomonas aeruginosa.
c. Streptococcus pyogenes.
d. Haemophilus influenzae.
26. The focus of primary infection in most cases of orbital cellulitis is
a. maxillary sinus.
b. ethmoid sinus.
c. frontal sinus.
d. orbital foreign body.
27. Sudden deterioration in ocular motility without a dramatic increase in proptosis suggests which complication of orbital cellulitis?
a. panophthalmitis.
b. meningitis.
c. cavernous sinus thrombosis.
d. subperiosteal abscess.
28. Which of the following concerning vernal conjunctivitis is true?
a. It is primarily a disease of the elderly.
b. It affects girls more frequently than boys.
c. Prominent symptoms include photophobia and itching.
d. The palpebral form of the disease is typically more severe inferiorly.
29. Which of the following is not a corneal manifestation of vernal disease?
a. deep stromal vascularization.
b. superficial punctate keratitis.
c. superior corneal pannus.
d. transverse oval sterile ulceration in the superior cornea.
30. In regard to vernal keratoconjunctivitis and trachoma, which of the following is true?
a. The limbal nodules of vernal keratoconjunctivitis are actually follicles.
b. Horner-Trantas dots and Herbert’s pits are histopathologically indistinguishable.
c. The presence of superior corneal pannus favors the diagnosis of trachoma over vernal conjunctivitis.
d. The shield ulcers of vernal keratoconjunctivitis are primarily due to mechanical abrasion by tarsal papillae.
31. Which of the following is not a diagnostic criterion for Kawasaki’s disease?
a. bilateral uveitis.
b. mucous membrane injection with fissures.
c. strawberry tongue.
d. desquamating rash of the palms and/ or soles.
32. Systemic mortality due to Kawasaki’s disease is most frequently due to
a. stroke.
b. respiratory failure.
c. myocardial infarction.
d. acute renal failure.
33. Which one of the following concerning the anatomy of the nasolacrimal system is false?
a. The canaliculi normally run vertically for 1 or 2 mm before running medially toward the nasolacrimal sac.
b. The medial palpebral ligament straddles the lower one-third of the nasolacrimal sac.
c. The nasolacrimal canal extends downward, posteriorly, and laterally through the lateral nasal wall.
d. The lining of the canaliculi is a stratified squamous epithelium, whereas that of the naso-lacrimal sac and canal is a bilayered columnar epithelium.
34. Which one of the following concerning congenital impatency of nasolacrimal system is false?
a. It may mimic a medial canthal hemangioma.
b. Acute dacryocystitis is uncommon.
c. The defect in canalization is within the intraosseous portion of the nasolacrimal duct.
d. Common symptoms include epiphora and mucus discharge.
35. An infant presents with bilateral findings as demonstrated in the photograph shown at the top of the next page. The intraocular pressure is normal. There is no increase in corneal diameter. What is the most likely diagnosis?
a. congential glaucoma.
b. congential hereditary endothelial dystrophy (CHED).
c. bacterial keratitis.
d. sclerocornea.

36. A 15-year-old boy presents with a 2-week history of malaise, low-grade fever, and headache. Four days prior to presentation, he developed a severe sore throat and bilateral upper eyelid swelling. Examination shows a mildly ill boy with a temperature of 100.1°F, moderately severe pharyngitis, mildly tender cervical lymphadenopathy, mildly tender enlarged lacrimal glands, and a maculopapular rash on all four extremities. A likely etiology for all the findings would be
a. infectious mononucleosis.
b. sarcoidosis.
c. diphtheria.
d. Kawasaki’s disease.
37. Corneal ulceration and scarring seen in familial dysautonomia (Riley-Day syndrome) is secondary to
a. impaired epithelial–stromal adherence.
b. impaired corneal sensation.
c. impaired humoral immune responses.
d. increased lacrimation.
38. Which of the following concerning the epidemiology of infantile glaucoma is not true?
a. Most cases are bilateral.
b. Subsequent offspring of parents with an affected child have approximately a 5% chance of manifesting the condition.
c. A patient with infantile glaucoma has approximately a 5% chance of having a child similarly affected.
d. The incidence of primary open-angle glaucoma in grandparents of an affected patient is elevated.
39. Which of the following is true in regard to infantile glaucoma?
a. Acute ruptures in Descemet’s membrane associated with infantile glaucoma are typically vertical, whereas those associated with birth trauma are typically horizontal.
b. Corneal clouding or tearing is more likely to be the presenting symptom with glaucoma whose onset is before the age of 3 months, whereas corneal enlargement will probably be the presenting finding in older infants.
c. Like optic nerve cupping, an afferent pupillary defect carries little prognostic significance in infantile glaucoma.
d. The upper end of normal IOP for infants and children is felt to be the same as that for adults: 22 mm Hg.
40. Recognized methods for long-term management of infantile glaucoma include all of the following except
a. trabeculotomy.
b. trabeculectomy.
c. goniotomy.
d. oral carbonic anhydrase inhibitors.
41. Systemic evaluation of the neonate with glaucoma should include
a. serum galactose levels.
b. serum antirubella IgG levels.
c. serum phytanic acid levels.
d. urinalysis for proteinuria and aminoaciduria.
42. Which of the following concerning Marfan’s syndrome is true?
a. The majority of cases are sporadic.
b. Only a small percentage of patients with the full syndrome develop ectopia lentis.
c. The average refraction on patients with the syndrome reveals moderate hyperopia.
d. Systemic treatment of the condition may include propranolol and antibiotic prophylaxis before dental procedures.
43. Which of the following concerning homocystin-uria is/are true?
a. This disorder is inherited on an autosomaldominant basis.
b. The majority of patients will develop ectopia lentis.
c. Systemic mortality is due to a coagulopathy with clotting deficiency and bleeding diatheses.
d. The primary defect leading to lens dislocation is a structural deficiency in the capsule.
44. Ectopia lentis associated with mental retardation may be seen in which of the following disorders?
a. Weill-Marchesani syndrome.
b. Sturge-Weber syndrome.
c. Edward’s syndrome.
d. Down’s syndrome.
45. Which of the following types of congenital cataract does not require systemic laboratory evaluation?
a. bilateral cataracts with no family history.
b. monocular cataract with no family history.
c. cataract associated with retinal pigment epithelial abnormalities.
d. anterior lenticonus.
46. Which of the following congenital cataract scenarios mandates the most urgent surgical intervention?
a. binocular posterior lenticonus.
b. monocular lamellar cataract.
c. monocular nuclear cataract.
d. binocular nuclear cataract.
47. Which one of the following statements regarding alterations in surgical strategy for pediatric cataract extraction (relative to adults) is false?
a. Intracapsular surgery is generally avoided in younger patients due to more prominent hya-loideocapsular attachments.
b. Extracapsular nuclear expression is generally avoided because of the small, relatively soft nucleus of the juvenile cataract.
c. Pediatric cataracts are usually soft and can be aspirated entirely.
d. Primary posterior capsulectomy is generally not undertaken due to more prominent hya-loideocapsular attachments in the young eye.
48. Which of the following concerning the five subtypes of JRA is true?
a. With the exception of the pauciarticular, lateonset type (HLA-B27 positive), all of the subtypes of JRA are considerably more common in girls.
b. The group at highest risk of developing anterior uveitis is the pauciarticular early-onset group with rheumatoid factor (RF) negative and antinuclear antibody (ANA) negative.
c. Iridocyclitis is frequently seen as part of the syndrome of systemic JRA (Still’s disease).
d. The joints involved in patients with iridocyclitis are typically the large joints (knee, ankle, elbow).
49. Which one of the following concerning the pediatric uveitis associated with herpes zoster virus (HZV) is false?
a. Typically, the uveitis develops during convalescence from acute varicella infection.
b. The uveitis in (reactivated) zoster ophthalmicus may have both anterior and posterior components.
c. Reactivation disease also may be accompanied by a keratitis, either epithelial or stromal.
d. In the setting of immunosuppression, reactivation disease should be treated with systemic as well as topical corticosteroids.
50. The most common etiology of posterior uveitis in the pediatric population is
a. toxocariasis.
b. toxoplasmosis.
c. syphilis.
d. sarcoidosis.
51. Manifestations of acquired systemic toxoplasmosis include all the following except
a. acute arthritis.
b. meningoencephalitis.
c. influenza-like syndrome.
d. retinitis.
52. Which one of the following concerning ocular histoplasmosis is false?
a. Symptoms consistent with histoplasmosis include a flulike syndrome and malaise.
b. There is a geographic, but not a seasonal, predilection for the development of systemic or ocular histoplasmosis.
c. The vitritis that may accompany the ocular infection may lead to decreased visual acuity.
d. Although skin testing may support the diagnosis, it may lead to worsening of the macular disease.
53. Which of the following concerning toxocariasis is not true?
a. The infectious cycle in humans generally starts with the consumption of fecally contaminated soil.
b. The condition may present as a peripheral granuloma in an otherwise quiet eye.
c. There may be an associated peripheral eosinophilia.
d. The associated uveitis is due to a hyper sensitivity reaction to living organism.
54. Which of the following concerning idiopathic pars planitis is not true?
a. It may have a mild course, with floaters as the only symptom.
b. Peripheral retinal periphlebitis is frequently associated.
c. Infectious etiologies are usually not found.
d. It is usually unilateral.
55. Findings in a patient with known JRA and uveitis that should prompt an increase in topical steroid administration include
a. aqueous cells.
b. worsening cataract.
c. flare.
d. band keratopathy
56. Which one of the following concerning persistent hyperplastic primary vitreous (PHPV) is false?
a. The presence of dense leukocoria in an eye that is abnormally small suggests the diagnosis of retinoblastoma rather than PHPV.
b. In severe cases, fibrovascular overgrowth within the primary vitreous may invade the lens substance itself.
c. A common complication is glaucoma, either secondary to vitreous hemorrhage or secondary angle closure.
d. The condition is typically unilateral.
57. The incidence of retinopathy of prematurity of any stage in premature children weighing <1,250 g at birth is approximately
a. 5%.
b. 25%.
c. 50%.
d. 65%.
58. Which one of the following concerning Coats’ disease is false?
a. True Coats’ disease is a disorder of childhood, more often affecting boys.
b. The condition is more commonly bilateral than unilateral.
c. Diagnosis of Coats’ disease may not be made in the setting of subretinal exudate without obvious abnormal retinal vessels.
d. In up to one-half of untreated cases, the condition may be nonprogressive.
59. Children of diabetic mothers are at increased risk for the development of
a. Coats’ disease.
b. pigmentary glaucoma.
c. pseudotumor cerebri.
d. optic nerve hypoplasia.
60. The most common fundus finding in a patient with acute leukemic oculopathy is
a. choroidal infiltration (creamy elevated subretinal patches).
b. nerve fiber layer hemorrhages.
c. cotton-wool spots.
d. Roth’s spots.
61. Which of the following concerning the gangliosidoses is/are true?
a. The most common is Sandhoff ‘s disease.
b. Inheritance is generally on an X-linked recessive basis.
c. Prominent cherry-red spots are typically seen in Tay-Sachs and Sandhoff ‘s diseases.
d. Patients generally succumb to neurologic deterioration in their late teens or early twenties.
62. Which one of the following concerning the ocu-lorenal syndromes is false?
a. Lowe’s syndrome is inherited on an X-linked recessive basis.
b. Female carriers of Lowe’s syndrome may be detected by punctate cortical opacities of the lens.
c. The most common ocular disorder in Lowe’s syndrome is glaucoma.
d. The most common ocular finding in Alport’s syndrome is anterior lenticonus and/or anterior polar cataract.
63. Which of the following is true in regard to pediatric vitreoretinal disease?
a. In albinism, more ganglion cell fibers decussate at the chiasm than in normal visual pathways.
b. The tyrosinase-negative type of albinism generally has more severe clinical findings than the tyrosinase-positive type.
c. The vitreous is normal in juvenile retinoschisis.
d. Most cases of sector retinitis pigmentosa ultimately progress to macular involvement with a poor visual prognosis.
64. The most common underlying disorder in a patient with a ‘bull’s-eye’ maculopathy is
a. Stargardt’s disease.
b. cone dystrophy.
c. chloroquine retinopathy.
d. Best’s disease.
65. Which one of the following regarding the various forms of congenital stationary night blindness (CSNB) is false?
a. Retinitis punctata albescens is associated with dots deep in the retina.
b. Fundus albipunctatus reveals normalization of the scotopic ERG after prolonged dark adaptation (after 3 to 12 hours).
c. One variety may have a normal scotopic A-wave with no apparent B-wave.
d. Oguchi’s disease displays the Mizuo phenomenon: a golden sheen of the retina returning to normal after several hours of dark adaptation.
66. Which of the following findings is not associated with Leber’s congenital amaurosis?
a. oculodigital sign.
b. keratoconus.
c. high myopia.
d. sensorineural hearing loss.
67. Which of the following is not true?
a. Visual acuity, although usually better in blue cone monochromatism than rod monochromatism, is not reliable for distinguishing between the two.
b. In most cases designated as Stargardt’s disease, the presenting symptom is night blindness.
c. Visual function in the pattern dystrophies of the retinal pigment epithelium (RPE) is usually good.
d. Colobomata involving the optic nerve may be associated with nonrhegmatogenous retinal detachment.
68. All of the following are features of Aicardi’s syndrome except
a. X-linked recessive inheritance.
b. agenesis of the corpus callosum.
c. lacunar chorioretinal degeneration.
d. severe mental retardation.
69. Which of the following findings is not consistent with the tilted disc syndrome?
a. prominence of the superior portion of the disc.
b. an inferior or inferonasal scleral crescent.
c. situs inversus.
d. binasal field defects.
70. Which of the following concerning optic nerve hypoplasia is not true?
a. The condition may be unilateral or bilateral.
b. Visual acuity may vary from normal to no light perception.
c. A classic finding is the double ring sign.
d. The association of optic nerve hypoplasia, absence of the septum pellucidum, midline central nervous system (CNS) anomalies, and hypothalamic–pituitary abnormalities is stronger for unilateral than for bilateral optic nerve hypoplasia.
71. The most common location for optic disc pits is
a. superonasal.
b. superotemporal.
c. inferotemporal.
d. inferonasal.
72. Aids in distinguishing pseudopapilledema with buried drusen from true papilledema include
a. red free photographs.
b. magnetic resonance imaging (MRI).
c. visual fields.
d. ultrasonography.
73. Which one of the following concerning the fibroosseous disorders of the orbit is false?
a. The distinction between fibrous dysplasia and ossifying fibroma is generally made radiologically.
b. Generally, fibrous dysplasia stabilizes after skeletal maturity is attained.
c. The polyostotic variety of fibrous dysplasia may be accompanied by sexual precocity and hyperpigmented skin macules.
d. The most significant visual implication of fibroosseous orbital lesions is optic nerve compression.
74. Which one of the following is false in regard to the lesion depicted in the photograph shown at the top of the next column?
a. They are more common in girls than in boys.
b. They characteristically blanch with pressure.
c. Phlebolith formation is common.
d. Indications for treatment include occlusion amblyopia and/or significant astigmatism.

75. Which of the following concerning lymphangiomas is not true?
a. They are primarily a disorder of the pediatric age range.
b. Superficial lesions may have a bluish or violaceous hue.
c. Classic presenting symptoms include proptosis with crying and following upper respiratory infections, and spontaneous ecchymosis.
d. Surgical intervention is indicated early in the course of the disorder in order to remove the tumor while it is small.
76. Which of the following concerning the epidemiology of rhabdomyosarcoma is not true?
a. It is one of the most common soft-tissue malignancies in children.
b. It is the most common solid malignant tumor of the orbit in children.
c. A common presentation is an orbital cellulitislike picture.
d. The average age at diagnosis is 2 years.
77. Which of the following regarding the histopathology of rhabdomyosarcoma is true?
a. The embryonal type is the least common.
b. The embryonal type has the best prognosis.
c. The alveolar type has the worst prognosis.
d. The differentiated (pleomorphic) type is the second most common.
78. Which of the following concerning the neurilem-moma (schwannoma) is true?
a. The majority of patients with neurofibromatosis will develop at least one.
b. The lesion can be exquisitely tender or painful.
c. Malignant degeneration is common.
d. There are three classic histopathologic patterns.
79. Which of the following concerning neurofibroma is true?
a. The nodular neurofibroma is the most specific for neurofibromatosis.
b. Like schwannomas, neurofibromas grow in close relation to peripheral nerves.
c. Neurofibromas are generally osteosclerotic.
d. The association of neurofibroma with congenital glaucoma is strongest with lesions of the upper eyelid.
80. Which of the following regarding the epidemiology of neuroblastoma is not true?
a. This tumor presents as metastases in over half of the cases.
b. In some pediatric series, the incidence is greater than that of rhabdomyosarcoma.
c. The second most common site of origin is the retroperitoneal sympathetic chain.
d. The site of origin is the adrenal gland in at least half of the cases.
81. Common presentations for neuroblastoma metastatic to the orbit include all of the following except
a. rapidly developing proptosis.
b. enophthalmos.
c. spontaneous ecchymoses.
d. orbital cellulitis.
82. All of the following are features of the histopathology of metastatic neuroblastoma except
a. sheets of indistinct round cells with scanty cytoplasm.
b. areas of tumor necrosis.
c. Homer-Wright rosettes.
d. bony invasion.
83. Which of the following is considered an ominous prognostic factor for metastatic neuroblastoma?
a. bone metastases.
b. liver metastases.
c. age more than 1 year.
d. bone marrow metastases.
84. The paraneoplastic syndrome most commonly associated with metastatic neuroblastoma is
a. photoreceptor degeneration.
b. optic neuropathy.
c. opsoclonus.
d. facial myokymia.
85. Which of the following concerning Ewing’s sarcoma is true?
a. Like neuroblastoma, this tumor may present with an orbital cellulitis-like picture.
b. Invasion of the globe is common.
c. The age at onset is younger than for neuroblastoma.
d. Unlike neuroblastoma, there is no role for radiotherapy.
86. Which one of the following concerning ocular adnexal dermoid cysts is false?
a. The most common location is the superonasal orbital rim.
b. Generally, they do not enlarge after the first year of life.
c. Rupture may lead to an orbital cellulitis-like picture.
d. Radiography of orbital lesions generally demonstrates bony excavation.
87. The epibulbar lesion most commonly seen in children under the age of 15 years is
a. dermoid.
b. dermolipoma.
c. nevus.
d. epithelial inclusion cyst.
88. Which of the following concerning the incidence of retinoblastoma is not true?
a. The most frequent age at diagnosis is 18 months.
b. Ninety percent of cases are diagnosed by the age of 3 years.
c. Almost 95% of newly diagnosed cases will have no family history of retinoblastoma.
d. The most reliable clue to the presence of a new germline mutation is unilateral involvement.
89. A couple gives birth to a child who, at the age of 9 months, is diagnosed with bilateral retinoblastoma. There is no previous family history of the disorder. Which one of the following statements regarding this situation is incorrect?
a. The child most likely carries one abnormal copy of chromosome 13 in each of his cells.
b. The chance of this child having an affected brother or sister is approximately 6%.
c. Either the mother or the father must carry an abnormal copy of chromosome 13 in their germ cells.
d. The child’s life expectancy is less than normal.
90. Two years later, the same couple gives birth to another child who, at the age of 15 months, is diagnosed with bilateral retinoblastoma. When the parents inquire about the probability of their next child developing retinoblastoma, they should be told that the probability is approximately
a. <1%.
b. 6%.
c.25%.
d.40%.
91. Patients who have received radiation therapy for bilateral retinoblastoma are at increased risk for the development of all of the following except
a. choroidal osteoma.
b. osteogenic sarcoma of the long bones.
c. osteogenic sarcoma of the orbital bones.
d. leiomyosarcomas of the eye or orbit.
92. Which of the following is the most common presentation for retinoblastoma?
a. decreased vision.
b. strabismus.
c. incidental finding.
d. leukocoria.
93. Which of the following statements pertaining to retinoblastoma is true?
a. Retinoblastoma that grows into the vitreous in a mushroom or spherical shape is termed “exophytic.”
b. An interesting light microscopic characteristic of retinoblastoma is zonal necrosis of tumor surrounding blood vessels.
c. The genetic implications of retinoma (retinocytoma) are identical to those of retinoblastoma.
d. Case reports of pineal gland neoplasms associated with retinoblastoma probably represent central nervous system metastasis.
94. The blood vessels in a retinoblastoma may absorb released nucleic acids from the necrotic cells and take on what appearance microscopically?
a. eosinophilia.
b. basophilia.
c. fibrinoid necrosis.
d. xanthomatization.
95. Which of the following is the most common site of retinoblastoma spread outside the eye?
a. skull bones.
b. liver.
c. lymph nodes.
d. central nervous system (CNS).
96. Which one of the following regarding the treatment of retinoblastoma is false?
a. For large tumors, treatment generally includes enucleation.
b. In advanced or metastatic cases, chemotherapy is used.
c. Cryotherapy is avoided because it typically leads to dissemination of viable tumor cells within the eye.
d. Cobalt plaque therapy has been used in eyes that have incompletely responded to external beam irradiation.
97. Which one of the following regarding medullo-epithelioma (diktyoma) is false?
a. The cell of origin is probably nonpigmented ciliary epithelium.
b. Like hemangiopericytoma, tumors with benign histopathologic features have a signifi-cant metastatic potential.
c. A teratoid variant exists that may contain cartilage, muscle, or neural tissue.
d. Leukocoria may be the presenting finding.
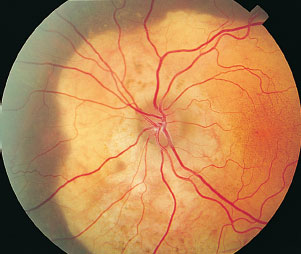
98. A 17-year-old girl undergoes dilated funduscopic examination after being fit for contact lenses. A creamy orange, geographic placoid elevation deep to the retina is noted (photograph below). Ultrasonography reveals a very highly reflective thickening of choroid in the same region. Computed tomography (CT) reveals calcification. The most likely diagnosis is
a. amelanotic melanoma.
b. choroidal hemangioma.
c. choroidal osteoma.
d. choroidal metastasis from an ovarian primary.
99. Which of the following tests is most likely to be normal in severe unilateral optic nerve hypoplasia?
a. visual acuity test.
b. swinging flashlight test.
c. electroretinography.
d. visual evoked responses.
100. Seizures, mental retardation, and facial angiofibroma (as depicted in the photograph below) form the classic triad for
a. neurofibromatosis.
b. tuberous sclerosis.
c. von Hippel-Lindau disease.
d. ataxia–telangiectasia.

101. Which of the following is true in regard to Sturge-Weber syndrome?
a. The complete Sturge-Weber syndrome includes facial hemangioma, ipsilateral glaucoma, and ipsilateral epilepsy.
b. The classic fundus finding in a patient with Sturge-Weber syndrome is the focal choroidal hemangioma.
c. The glaucoma seen ipsilateral to facial hemangioma in Sturge-Weber syndrome is due entirely to elevated episcleral venous pressure (EVP).
d. In Sturge-Weber syndrome, iris neovascularization may complicate the course of retinal angiomatosis.
102. What percentage of patients with capillary hemangiomas of the retina will develop hemangio-blastomas of the cerebellum?
a. 5%.
b. 20%.
c. 50%.
d. 75%.
103. Which of the following disorders is inherited on an autosomal-recessive basis?
a. tuberous sclerosis.
b. Sturge-Weber syndrome.
c. von Hippel-Lindau disease.
d. ataxia–telangiectasia.
104. Potential ocular manifestations of the craniosyn-ostoses include all of the following except
a. optic nerve hypoplasia.
b. papilledema.
c. exposure keratitis.
d. tortuous retinal vasculature.
105. The strabismus most frequently associated with the craniosynostoses is
a. double elevator palsy.
b. Duane’s syndrome.
c. V-pattern exotropia.
d. A-pattern esotropia.
106. Which of the following is not a feature of the Pierre Robin sequence?
a. cleft palate.
b. bird face.
c. glossoptosis.
d. micrognathia.
107. Lower lid colobomas, pronounced antimongoloid slant (downward displacement of the lateral canthus), and orbital rim defects are typical of
a. Hallermann-Streiff syndrome.
b. Treacher Collins’ syndrome.
c. Goldenhar’s syndrome.
d. Waardenburg’s syndrome.
108. Ocular findings in the patient photographed below least likely include
a. optic nerve hypoplasia.
b. hypertelorism.
c. anterior segment dysgeneses.
d. tortuous retinal vessels.

109. Which of the following arises from the annulus of Zinn?
a. superior oblique.
b. levator palpebrae superioris.
c. superior rectus.
d. inferior oblique.
110. The action(s) of the medial rectus muscle with the eye in primary position is/are
a. adduction, elevation, intorsion.
b. adduction, depression, intorsion.
c. adduction and intorsion.
d. adduction.
111. To maximize the elevation generated by the superior rectus, how must the eye be rotated from primary position?
a. adducted 51°.
b. abducted 51°.
c. adducted 23°.
d. abducted 23°.
112. To maximize the depression generated by the superior oblique, how must the eye be rotated?
a. adducted 51°.
b. abducted 51°.
c. adducted 23°.
d. abducted 23°.
113. Which of the following in regard to extraocular muscles is true?
a. Both oblique muscles are characterized by a physical distinction between the anatomic origin and the mechanical origin.
b. The superior oblique tendon passes between the superior rectus muscle and the globe on the way to its insertion.
c. The inferior oblique muscle passes between the inferior rectus muscle and the globe on the way to its insertion.
d. The superior oblique muscle becomes tendinous after turning through the trochlea.
114. The primary intorter of the globe in primary position is the
a. superior oblique.
b. superior rectus.
c. inferior oblique.
d. inferior rectus.
115. The extraocular muscle with the shortest length of active muscle belly is the
a. superior rectus.
b. inferior rectus.
c. superior oblique.
d. inferior oblique.
116. Which of the following changes in lid position are consistent with the muscle surgery described?
a. narrowing of palpebral fissure with superior rectus recession.
b. narrowing of palpebral fissure with inferior rectus recession.
c. narrowing of the palpebral fissure with inferior rectus resection.
d. narrowing of the palpebral fissure with superior oblique tenotomy.
117. Each of the following is a correct match of muscular synergist and antagonist except
a. lateral rectus: synergist, superior oblique; antagonist, medial rectus.
b. superior rectus: synergist, superior oblique; antagonist, inferior rectus.
c. inferior rectus: synergist, superior oblique; antagonist, superior rectus.
d. inferior oblique: synergist, superior rectus; antagonist, superior oblique.
118. Which one of the following constitutes a violation of Hering’s law?
a. cyclic esotropia.
b. dissociated vertical deviation (DVD).
c. Brown’s syndrome.
d. Duane’s syndrome.
119. Which one of the following constitutes a violation of Sherrington’s law?
a. cyclic esotropia.
b. dissociated vertical deviation (DVD).
c. Brown’s syndrome.
d. Duane’s syndrome.
120. The site of origin of neural impulses leading to a rightward saccade is the
a. right frontal lobe.
b. left frontal lobe.
c. right parietooccipital lobe.
d. left parietooccipital lobe.
121. The site of origin of neural impulses leading to a leftward pursuit movement is the
a. right frontal lobe.
b. left frontal lobe.
c. right parietooccipital lobe.
d. left parietooccipital lobe.
122. Which of the following is true?
a. Physiologically, any point not lying on the empirical horopter will be perceived doubly by the human visual system.
b. If simultaneous stimulation of retinal areas in two eyes leads to the perception of one image, normal retinal correspondence is said to exist.
c. For fusion to exist, there must be simultaneous stimulation of corresponding retinal areas with normal retinal correspondence.
d. For fusion to exist, the two retinal images must be similar in size and shape.
123. Which one of the following statements concerning motor fusion is false?
a. Motor fusion is the act by which similar retinal images are made to fall on corresponding retinal areas.
b. A normal convergence amplitude at distance is 14 prism diopters and at near is 38 prism diopters.
c. A normal divergence amplitude at distance is 14 D and at near is 16 D.
d. Normal vertical fusional amplitude varies from 2 to 4 prism diopters and is independent of fixation distance.
124. A vertical slit pattern is projected onto the fovea of the right eye, whereas a horizontal slit pattern is projected onto the fovea of the left eye. The subject perceives rapidly alternating images of each pattern—first one then the other, never simultaneously. This perception is an example of
a. fusion.
b. stereopsis.
c. suppression.
d. retinal rivalry.
125. Which of the following regarding amblyopia is true?
a. The incidence in the general population is approximately 0.2%.
b. The presence of an afferent pupillary defect clearly establishes an organic etiology for visual loss, rather than amblyopia.
c. Patients with amblyopia will frequently perform better with single-symbol acuity test targets than with line targets (crowded stimuli).
d. A neutral density filter placed over an amblyopic eye will generally cause a greater decrement in visual acuity than the same filter placed over an eye with maculopathy.
126. In which of the following types of strabismus is amblyopia least frequently seen?
a. infantile esotropia.
b. esotropia with high accommodative convergence to accommodation ratio (AC/A).
c. alternating esotropia.
d. esotropia associated with Duane’s syndrome.
127. A 7-year-old patient presents to a pediatric ophthalmologist after failing his school vision test. Visual acuity is 20/20 in the right eye and 20/50 in the left eye, tested with patching and Snellen targets. Motility is full, and there is no apparent tropia on cover–uncover testing. The child has stereoacuity with targets disparate by no <60 seconds of arc. Distance Worth four-dot testing reveals fusion. Convergence and divergence amplitudes are normal at distance. The most likely diagnosis is
a. cyclic esotropia.
b. monofixation syndrome.
c. central fixation with anomalous retinal correspondence.
d. factitious visual loss.
128. The patient in question 127 has no history of previous eye surgery. The remainder of his examination is most likely to disclose
a. high axial myopia bilaterally.
b. retraction of the globe on adduction.
c. anisometropia > 2D.
d. esotropia developing sometime within the next 24 hours.
129. The most practical and valuable test to perform next on the patient above would be
a. Lancaster red-green test.
b. afterimage testing.
c. Bagolini glass testing.
d. four-prism-diopter base-out test.
130. A 42-year-old patient presents to the emergency room with a manifest right esotropia. A red glass is placed over the left eye and the patient is asked to fixate at a distant point-light target. In the absence of suppression, and with normal retinal correspondence, the patient should perceive the red light
a. above the white light.
b. below the white light.
c. to the right of the white light.
d. to the left of the white light.
131. Which of the following regarding the afterimage test for retinal correspondence is true?
a. It is best to flash the vertical line into the fixating eye.
b. Regardless of fixation behavior, in the setting of normal retinal correspondence, the patient will perceive a cross with a single central gap.
c. A patient with a right exotropia, central fixation, and harmonious anomalous retinal correspondence will perceive the vertical line flashed into his right eye as being to the left of the horizontal image placed into his fixating left eye (crossed diplopia).
d. To appropriately interpret this test, the patient’s fixation behavior must be determined.
132. During routine examination, an alternate-cover test reveals outward fixation shifts of each eye as the cover is moved. The cover–uncover test reveals no shift of either eye as the cover is placed over either eye. The correct description of the patient’s motility status would be
a. orthophoric, esotropic.
b. orthotropic, esophoric.
c. orthotropic, exophoric.
d. This set of findings is not possible.
133. During a routine examination, the cover– uncover test reveals an outward fixation shift of either eye as the cover is placed over the contralateral eye. The alternate-cover test reveals no shift as the cover is moved back and forth. The correct description of this patient’s motility status would be
a. orthophoric, esotropic.
b. orthotropic, esophoric.
c. orthotropic, exophoric.
d. This set of findings is not possible.
134. Which of the following ocular alignment tests does not require foveal fixation in the deviated eye for quantification of the angle of strabismus?
a. the cover–uncover test with prisms.
b. the alternate-cover test with prisms.
c. the simultaneous prism-cover test.
d. the Krimsky test.
135. A patient with strabismus is asked to fixate a penlight held by the examiner. The examiner notes that the corneal reflex in the right eye is central, whereas that in the left eye is displaced approximately 3 mm temporal to the center of the pupil. Using Hirschberg’s method for estimating the angle of strabismus, the examiner concludes that the patient has a
a. 45-degree esotropia.
b. 45-prism-diopter esotropia.
c. 45-degree exotropia.
d. 45-prism-diopter exotropia.
136. When used with prisms, which of the following is best suited for quantification of a tropia only, with no contribution from a phoria?
a. cover–uncover test.
b. alternate-cover test.
c. Maddox rod testing.
d. simultaneous prism-cover test.
137. When tested with a Maddox rod held over the affected eye with its cylinders running horizontally, a patient with new-onset excyclotropia will perceive
a. a horizontal line.
b. a vertical line.
c. an oblique line running superotemporal to inferonasal.
d. an oblique line running superonasal to inferotemporal.
138. An adult with a right esotropia due to an acquired right abducens paresis is tested with the Lancaster red-green test. He wears the goggles with the red glass over his right eye and the green glass over his left. An examiner holds the green light central on the chart and gives the patient the red light. The patient is then instructed to superimpose his red light on the examiner’s green light. To the examiner
a. the red light will appear to the left of the green light.
b. the red light will appear above the green light.
c. the red light will appear to the right of the green light.
d. the lights will be superimposed.
139. To the patient described above in question 138:
a. the red light will appear to the left of the green light
b. the red light will appear above the green light.
c. the red light will appear to the right of the green light.
d. the lights will be superimposed.
140. The same patient described in question 139 is retested with the goggles reversed, that is, the green lens over the right eye and the red lens over the left eye. The examiner holds the green light as a fixation target centrally, and patient moves the red light. This time, the examiner will observe
a. the red light to the left of the green light at the same distance between the two as before.
b. the red light to the left of the green light at a larger distance between the two than before.
c. the red light to the right of the green light with the same distance between the two as before.
d. the red light to the right of the green light at a larger distance than before.
141. Broad nasal bridges with abnormally large angle kappa may lead to an error in the diagnosis of strabismus with which of the following methods?
a. alternate-cover tests.
b. Maddox rod testing.
c. cover–uncover testing.
d. Hirschberg testing.
142. To accurately quantify an esodeviation, prism is most appropriately placed over either eye
a. base up.
b. base out.
c. base down.
d. base in.
143. A 31-year-old man with moderate hyperopia presents for routine examination. There is a 10-prism-diopter alternating esotropia at distance. While reading through his distance correction at 20 cm, there is a 35-prism-diopter esotropia. Eye movements are full, and he denies any history of prior surgery. Yo u conclude that
a. He must have amblyopia in one eye.
b. He probably has restrictive strabismus.
c. He probably will note double vision if questioned appropriately.
d. He has a high AC/A ratio.
144. In regard to question 143, the examiner elects to calculate the patient’s AC/A ratio. His interpu-pillary distance is 60 mm, and his near deviation increases to 50 prism diopters when he views an acuity target through a 1.00 D sphere over each eye. By the gradient method, his AC/A ratio measures
a. 5:1.
b. 11:1.
c. 15:1.
d. 25:1.
145. For the patient above, using the heterophoria method the AC/A ratio measures
a. 5:1.
b. 11:1.
c. 15:1.
d. 25:1.
146. In the patient shown below, what is the most likely diagnosis?
a. right superior oblique palsy.
b. left superior oblique palsy.
c. right superior rectus palsy.
d. left superior rectus palsy.
147. A patient undergoes left orbital exploration for biopsy of a suspicious infiltrate on computed tomography (CT) scanning. Postoperatively, the patient is noted to have a widely dilated pupil and poor vision at near in the left eye. He also complains of binocular diplopia. You note an inability to elevate the eye when it is adducted. What findings would you expect on the three-step test?
a. a right hypertropia worse in right gaze and left head tilt.
b. a left hypertropia worse in left gaze and right head tilt.
c. a right hypertropia worse in right gaze and right head tilt.
d. a left hypertropia worse in right gaze and left head tilt.
148. Atropine is relatively contraindicated in all of the following groups except
a. albinos.
b. neonates.
c. patients with Down’s syndrome.
d. patients with heart block.
149. Systemic manifestations of cycloplegic intoxication include all of the following except
a. flushing.
b. agitation.
c. bradycardia.
d. somnolence.
150. Which of the following concerning the patient represented in the photograph at the top of the right column is most likely true?
a. Although it is typically seen in isolation, these findings may be associated with neurologic abnormalities.
b. Amblyopia will likely develop as the child cross-fixates.
c. Characteristically, the esotropia is small (<25 prism diopters).
d. There is never an accommodative component found in this clinical scenario.

151. Findings commonly associated with infantile esotropia on examination include all of the following except
a. latent nystagmus.
b. high AC/A ratio.
c. overaction of the inferior obliques.
d. disassociated vertical divergence (DVD).
152. Appropriate options for initial surgical intervention in infantile esotropia include all of the following except
a. bimedial recession.
b. bilateral resection.
c. ipsilateral medial rectus recession and lateral rectus resection.
d. bimedial resection.
153. Parents bring their 3-year-old boy for examination after they note the development of “cross-eyes.” Upon closer review, the parents report that they originally noted the deviation to be present throughout the day at age 2. A brief “glance” at the child makes a constant moderate-angle esotropia obvious. Which of the following is most likely true?
a. Amblyopia is highly unlikely.
b. With further careful questioning, it may be possible to document that the deviation was originally intermittent.
c. The child should be able to perceive the wings of the Titmus fly in three dimensions.
d. It would be surprising to find a family history of a similar disorder.
154. As part of the comprehensive examination of the patient in question 153, a cycloplegic refraction is performed and reveals +8.50 D in both eyes. Which of the following is/are true?
a. There may be unilateral amblyopia.
b. The deviation will certainly be greater at near than at distance.
c. +3.00 D lenses are likely to have little effect on the distance deviation.
d. The deviation at distance is likely to measure >50 prism diopters.
155. The initial step in management of the patient above must be
a. penalization with atropine bilaterally.
b. full correction of the cycloplegic refractive error.
c. bifocals.
d. bimedial recession.
156. Parents bring their child to the ophthalmologist after noting “cross-eyes.” On further questioning, they report that they noted the deviation to be present throughout the day since approximately age 2. A quick glance at the child reveals an obvious intermittent moderate-angle esotropia. It seems to be larger when the child plays with an object in his hands. Cycloplegic refraction reveals +1.50 D in both eyes. Which of the following is likely false?
a. The deviation at distance is not likely to be large.
b. The deviation at near is likely to be moderate (20 to 30 prism diopters).
c. The deviation at near is likely to be lessened with +3.00 D lenses over each eye.
d. The AC/A ratio is likely to be <5.
157. Which of the following regarding the treatment of esotropia is true?
a. Accommodative esotropia is more likely to require surgical intervention than infantile esotropia.
b. Bifocals are most helpful in the management of patients with refractive accommodative esotropia.
c. If refractive correction fails to solve the problem, the only solution is surgical.
d. Accommodative esotropia may progress over the first 5 to 7 years of life and should be monitored carefully.
158. Clinical features of esotropia that are predictive of the need for future surgical intervention include all of the following except
a. presence of overaction of the inferior obliques.
b. large-angle esotropia (>50 prism diopters).
c. age of onset between 2 and 3 years.
d. low hyperopia or myopia.
159. Which of the following regarding the treatment of accommodative esotropia is true?
a. No improvement of esotropia with miotic therapy rules out the possibility of an accommodative component.
b. Delay in refractive correction of an accommodative esotropia increases the probability of a permanent residual esotropia after full correction is given.
c. It is important to attempt surgical realignment before prolonged occlusion therapy.
d. Surgical realignment resulting in a residual esotropia of <20 prism diopters may permit the development of peripheral fusion.
160. In intermittent accommodative esotropia, some ophthalmologists do not prescribe full hyper-opic correction because
a. Distance vision will be blurred.
b. The greater deviation at near will not be fully compensated.
c. The patient may be converted to a constant esotropia without glasses.
d. The patient may become exotropic with full hyperopic correction.
161. Divergence insufficiency resembles lateral rectus palsy except
a. There is typically an esodeviation.
b. The deviation is generally worse at distance.
c. There are commonly no associated neurologic abnormalities.
d. The deviation is comitant.
162. Findings that favor the diagnosis of spasm of the near reflex rather than accommodative esotropia include
a. new hyperopia.
b. esotropia worse at near than at distance.
c. miosis on attempted lateral gaze.
d. no vertical component.
163. The feature least consistent with acquired abducens paresis include all of the following except
a. esotropia.
b. deviation greater at distance than near.
c. amblyopia.
d. head turn toward the side of the paretic muscle.
164. An exodeviation that is greater at distance than at near is known as
a. basic exotropia.
b. divergence excess exotropia.
c. basic exophoria.
e. convergence insufficiency exotropia.
165. To distinguish true divergence excess exotropia from “simulated divergence excess” exotropia,
a. The deviations are remeasured after cycloplegia.
b. The AC/A ratio is calculated by the heterophoria method.
c. The AC/A ratio is calculated by the gradient method.
d. The deviations are remeasured after prolonged (30–45 minutes) monocular occlusion.
166. The most common etiology for constant exotro-pia is
a. decompensated intermittent exotropia.
b. sensory exotropia.
c. third nerve palsy.
d. Duane’s syndrome type II.
167. Clinical features frequently associated with intermittent exotropia include all of the following except
a. variable angle of deviation.
b. high AC/A ratio.
c. reflex closure of one eye in bright light.
d. amblyopia.
168. Useful treatment modalities for intermittent exotropia include
a. plus lenses.
b. phospholine iodide.
c. base-in prism.
d. bilateral rectus resections.
169. Clinical features of convergence insufficiency include all of the following except
a. asthenopia.
b. blurry reading vision.
c. diplopia while reading.
d. exophoria at near.
170. A patient presents for evaluation of “wandering eyes.” On alternate-cover testing, with the left eye covered, the right eye fixes a distance target. As the cover is shifted to the right eye, the left eye moves down to pick up fixation. As the cover is moved back over the left eye, the right eye moves upward to reassume fixation. This set of findings is consistent with
a. right hyperdeviation.
b. left hyperdeviation.
c. overaction of the inferior obliques.
d. dissociated vertical deviation (DVD).
171. A patient presents for evaluation of “wandering eyes.” On alternate-cover testing, with the left eye covered, the right eye fixes a distance target. As the cover is shifted to the right eye, the left eye moves down to pick up fixation. As the cover is shifted back over the left eye, the right does not move in order to reassume fixation. This set of findings is most consistent with
a. right hyperdeviation.
b. left hyperdeviation.
c. overaction of the inferior obliques.
d. dissociated vertical deviation (DVD).
172. A 4-year-old child with a moderate-angle esotropia is noted to have a left hypertropia on right gaze and a right hypertropia on left gaze. When fixing with the left eye in right gaze, there is a right hypotropia, and when fixing with the right eye in left gaze, there is a left hypotropia. The most likely clinical diagnosis is
a. right hypotropia.
b. left hypotropia.
c. esotropia associated with overaction of the inferior oblique muscles.
d. esotropia with DVD.
173. Which of the following features argue for a bilateral rather than a unilateral superior oblique paresis?
a. head tilt.
b. symptomatic excyclotorsion.
c. a pattern esotropia.
d. aggravation of diplopia with right or left head tilt.
174. Surgical strategies for the management of a right superior oblique paresis with symptomatic diplopia include all of the following except
a. right inferior oblique myectomy.
b. right superior oblique tuck.
c. right inferior rectus recession.
d. left superior oblique tenectomy.
175. The surgical procedure of choice in a superior oblique paresis with excyclotorsion only (no vertical diplopia) is the
a. ipsilateral superior oblique tuck.
b. ipsilateral inferior oblique myectomy.
c. recession of the ipsilateral superior rectus muscle.
d. lateral transposition of the superior oblique tendon.
176. In young healthy eyes, anterior segment ischemia becomes a concern after surgery on how many rectus muscles?
a. 1.
b. 2.
c. 3.
d. 4.
177. Of the following acuity tests, which is least likely to lead to an overestimation of actual recognition acuity?
a. single Snellen letters.
b. illiterate E.
c. optotype cards.
d. Allen cards.
178. All of the following are features consistent with double elevator palsy except
a. ptosis.
b. forced ductions indicating inferior rectus restriction.
c. chin-down head position.
d. poor Bell’s phenomenon on the side of the palsy.
179. Which one of the following regarding Brown’s syndrome is false?
a. Both congenital and acquired forms exist.
b. A common manifestation is hypotropia of the involved eye in adduction.
c. Duction and version testing mimic weakness of the ipsilateral superior oblique muscle.
d. Forced duction testing is necessary to confirm the diagnosis.
180. Late clinical findings consistent with an inferior blowout fracture of the orbit include all of the following except
a. proptosis.
b. paresthesia or hypesthesia of the infraorbital region.
c. ipsilateral hypotropia on upgaze.
d. ipsilateral hypertropia on downgaze.
181. Which of the following regarding A and V patterns of horizontal strabismus is true?
a. A patterns must measure at least 15 prism diopters difference between upgaze and downgaze to be considered significant.
b. V patterns must measure at least 10 prism diopters between upgaze and downgaze to be considered significant.
c. These forms of noncomitance are seen in fewer than 5% of horizontal strabismus.
d. All the extraocular muscles (in varying combinations) have been implicated as responsible for these patterns.
182. A patient presents with an exotropia measuring 15 prism diopters in primary position. In down-gaze, it diminishes to <5 prism diopters, and in upgaze it increases to >30 prism diopters. There is no significant oblique muscle dysfunction noted. Appropriate surgical intervention might include all of the following except
a. recession of the ipsilateral lateral rectus.
b. resection of the ipsilateral medial rectus.
c. upward transposition of the lateral rectus and downward transposition of the medial rectus.
d. inferior oblique myectomy.
183. A patient presents with a 20-prism-diopter esotropia in primary gaze that increases to 35 prism diopters in downgaze and diminishes to 15 prism diopters in upgaze. There is overaction of the inferior obliques bilaterally. Appropriate surgical intervention might include all of the following except
a. upward transposition of the lateral rectus and downward transposition of the medial rectus muscles ipsilaterally.
b. recession of ipsilateral medial rectus muscle.
c. resection of the ipsilateral lateral rectus muscle.
d. bilateral inferior oblique myectomies.
184. The most common cause of third nerve palsy in the pediatric population is
a. congenital.
b. traumatic.
c. inflammatory.
d. tumor.
185. In adults, the most common cause of third nerve palsy is
a. microvascular.
b. traumatic.
c. aneurysm.
d. tumor.
186. Strabismus surgery for patients with Graves’ ophthalmopathy generally is performed before
a. orbital decompression.
b. orbital radiation.
c. tarsorrhaphy.
d. eyelid surgery.
187. A child’s nystagmus is noted to have equal velocity in all directions and to be symmetric in direction, amplitude, and frequency in each eye. The nystagmus would most appropriately be described as
a. pendular, conjugate.
b. jerk, conjugate.
c. pendular, disconjugate.
d. jerk, disconjugate.
188. Characteristics considered classic for spasmus nutans include all of the following except
a. head nodding.
b. a small-amplitude, disconjugate nystagmus.
c. torticollis.
d. hypertonia.
189. The entity in the differential diagnosis with spasmus nutans that must be ruled out is
a. optic nerve meningioma.
b. parasellar glioma.
c. pontine glioma.
d. cerebellar astrocytoma.
190. Treatment for a patient with congenital nystagmus whose null zone is in right gaze and who has adopted an extreme left head turn might include
a. prism base down in both eyes.
b. prism base in both eyes.
c. prism base in the right eye and base out in the left eye.
d. prism base out in the right eye and base in the left eye.
191. A 3-year-old child presents to the ophthalmologist with parents complaining of “cross-eyes” for approximately 1 year. Examination discloses visual acuity of 20/30 in the right eye and 20/100 in the left eye with Allen cards. There is a 35-prism-diopter esotropia at distance increasing to 45 prism diopters at near. Refraction reveals +3.50 D in both eyes. Initial steps in managing this patient should include
a. bimedial recessions.
b. bilateral resections.
c. prescription of +3.50 in both eyes with add +3.50 in both eyes (bifocals).
d. prescription of +3.50 D in both eyes and patching of the right eye.
192. A 7-year-old boy presents with an exotropia. His deviation measures 30 prism diopters in primary position, 20 prism diopters in right gaze, and 40 prism diopters in left gaze. Near deviation is 15 prism diopters in all directions. Fixation appears to alternate, and visual acuity is 20/20 in both eyes. The patient’s parents strongly desire some form of correction. You recommend
a. addition of -2.00 D to his current distance refraction.
b. bilateral rectus recessions, equal on each side.
c. bilateral rectus recessions with a greater distance of recession on the left.
d. bilateral rectus recessions with a greater distance of recession on the right.
193. A patient presents with symptomatic vertical diplopia from a right hypertropia that is greatest in left eye: left upgaze and left downgaze. Appropriate surgical intervention could include all of the following except
a. right superior oblique tuck.
b. left superior oblique tenotomy.
c. right inferior oblique myectomy.
d. right superior rectus resection.
194. A 1-year-old child is brought to the ophthalmologist by his parents who have noted that “cross-eyes” developed over the previous 6 months. Your examination reveals an approximately 40-prism-diopter esotropia at near that does not seem to diminish significantly when the child fixes at longer distances. The child can maintain fixation with either eye easily. Cycloplegic refraction reveals +1.50 D in both eyes. An appropriate step in the management of this patient might next be
a. prescription of +1.50 D glasses in both eyes.
b. prescription of +1.50 D in both eyes with +3.50 add in both eyes.
c. alternate patching throughout the day.
d. bilateral rectus recession of 8 mm in both eyes.
195. After treating a child with mixed mechanism esotropia for 8 months with full hyperopic correction and occlusion therapy, surgery is undertaken to realign his eyes. Visual acuity measures 20/50 in the right eye and 20/25 in the left eye with HOTV cards. There is an esotropia of 30 prism diopters in all directions of gaze. Appropriate surgical intervention would consist of
a. bimedial rectus recession of 4.5 mm in both eyes.
b. bilateral rectus resection of 7 mm in both eyes.
c. bimedial rectus recession of 7 mm in both eyes.
d. recession of the right medial rectus 4.5 mm and resection of the right lateral rectus 7 mm.
196. A 6-year-old patient presents to an ophthalmologist for the first time after failing a school eye examination. Complete ophthalmic examination discloses a visual acuity of 20/20 in the right eye and 20/100 in the left eye. There is a comi-tant left exotropia measuring 30 prism diopters. Cycloplegic refraction reveals +0.50 D in both eyes. A year of occlusion therapy of the right eye is undertaken, with little improvement in acuity in the left eye. The next step in the management of this patient might be
a. prescription of -1.50 D in both eyes.
b. base-in prism.
c. bilateral rectus recession of 7 mm.
d. recession of the left lateral rectus 7 mm and resection of the left medial rectus 6 mm.
197. Which of the following regarding diplopia after surgery for esotropia is true?
a. Children with acquired strabismus are more likely to suffer from symptoms than adults.
b. Postoperative diplopia is most likely to develop in undercorrection of intermittent exotropia.
c. A trial of preoperative prisms may be helpful in predicting who is likely to suffer from this complication.
d. The complication, if persistent, must be managed with a second surgical procedure.
198. A 2-year-old child undergoes bimedial recession for infantile esotropia. On the first postoperative day, the deviation is measured as <10 prism diopters of residual esotropia, with fairly good versions. At the 1-week visit, there is a prominent right exotropia, which increases in left gaze. Duction testing reveals an inability to adduct the right eye past the midline. The most likely diagnosis is
a. surgical undercorrection.
b. consecutive exotropia due to surgical overcorrection.
c. postoperative third nerve palsy.
d. lost or slipped right medial rectus.
199. Early signs in the development of malignant hyperthermia include all of the following except
a. tachycardia/arrhythmia.
b. elevated body temperature.
c. darkening of the blood in the operative field.
d. trismus.
200. The most common complication of botulinum injections is
a. vertical strabismus.
b. Adie’s pupil.
c. ptosis.
d. perforation of the globe.
 Answers
Answers1. c. Axial length increases most rapidly over the first 4 years of life and more slowly thereafter until age 10 to 12 years.
2. c. The lens is proportionately the largest part of the infant eye.
3. d. The dilator pupillae muscle is immature in infancy.
4. d. Acuity estimates are highest with VEP. OKN and PLT are fairly close. OKN is more cumbersome and difficult to quantify accurately than PLT. ERG measures gross retinal function, but does not give a clear indication of visual acuity.
5. a. The upper lids are more frequently involved. Other features include limbal dermoids, branchial cleft abnormalities, and vertebral anomalies.
6. b. The lower lids are more frequently involved by congenital ectropion and congenital entropion. There are four varieties of epicanthus: (a) palpebralis (simple), broader above; (b) inversus, and broader below; (c) tarsalis, equally broad above and below; and (d) supraciliaris, origin from eyebrow. Hypertelorism implies an abnormally wide distance between medial orbital walls. Telecanthus is an abnormally wide distance between medial canthi. Telecanthus may be isolated (primary) or secondary to hypertelorism.
7. a. This is a classic example of blepharophimosis. Epicanthus inversus is the other component of this tetrad. Ectropion or euryblepharon is seen in some cases, as well. This patient demonstrates pseudoesotropia in addition to many of the other findings.
8. c. Seventy percent of pregnant women are seronegative. Placental transfer of organism is common in the newly infected mother; however, many infected infants will not have systemic manifestations. Fetal infection earlier in gestation results in more severe involvement. The incidence of congenital toxo-plasmosis, both symptomatic and asymptomatic, is approximately 1 in 1,000 live births.
9. d. Microphthalmos and cataracts are rare. Focal chorioretinal lesions are common. Diffuse reti-nopathy is not seen.
10. a. Pyrimethamine and sulfadiazine are antimicrobial agents effective against Toxoplasma. Prednisone reduces inflammatory tissue destruction. Pyrimethamine blocks synthesis of folinic acid, so it must be given as well. Note that folinic acid is synthesized from dietary folic acid, so folic acid administration is not sufficient.
11. d. The later in the course of the pregnancy a mother is infected, the lower is the chance of fetal infection, and if infection occurs, the lower the likelihood of symptomatic defects. Infection early in pregnancy leads to a high rate of abnormalities. Thanks to vaccinations, most mothers in developed countries are seropositive (protected).
12. b. Many cases of “oculoauditory syndrome” are due to rubella.
13. c. Although children with congenital rubella syndrome may develop either cataract or glaucoma, their coincidence in an infant is rare. Live rubella virus may be recovered from an infected infant from conjunctival swabs, urine cultures, pharyngeal swabs, and lens aspirates.
14. d. Excessive rebound uveitis is due to live virus retained within residual lens cortex.
15. c. Approximately 2% of human infants are infected. Most cases are silent.
16. c. The most common ocular manifestation of congenital CMV infection is retinochoroiditis.
17. b. Most neonatal herpes is contracted at the time of delivery due to passage through an infected birth canal. Most cases of congenital herpes declare themselves with vesicular dermatitis, keratoconjunctivitis, pneumonitis, or meningoencephalitis. A posterior inflammatory component is far more common in congenital HSV disease, with severe retinitis and vitritis. This is unusual in acquired disease but may be the cause of some cases of acute retinal necrosis.
18. d. Herpes simplex is generally transmitted at the time of birth as the child passes through an infected birth canal.
19. a. Rhagades, linear scars around the mouth, are characteristic of congenital lues, but not a part of Hutchinson’s triad.
20. c. Treatment clearly reduces the likelihood of a no light perception (NLP) outcome, but the long-term Snellen acuity levels are disappointing. In fact, treated eyes were slightly, albeit not significantly, less likely to retain 20/40 or better than eyes randomized to no treatment.
21. d.Streptococcus pyogenes is an infrequent cause. Staphylococcus aureus, Streptococcus pneumococcus, and Haemophilus influenzae are far more common.
22. b. Pharyngoconjunctival fever (adeno type 3) generally spares the cornea, although subepithelial infiltrates or superficial punctate keratitis may rarely be seen.
23. a. The inflammation in Parinaud’s syndrome is always granulomatous.
24. a. The most common cause of preseptal cellulitis in children is minor skin trauma.
25. d.H. influenzae is the agent most frequently associated with orbital cellulitis following bacterial conjunctivitis.
26. b. Ethmoid sinusitis is the leading risk factor for the development of orbital cellulitis.
27. c. Cavernous sinus inflammation causes cranial nerve dysfunction without proptosis, leading to a sudden worsening of ocular motility without other changes in the examination.
28. c. Boys in their first two decades are more frequently involved than girls, and the upper tarsal conjunctiva is more commonly and more severely involved than the lower.
29. a. Deep corneal vascularization is unlikely in vernal disease. So-called shield ulcers—large oval, central epithelial defects—are classic corneal manifestations of the disease.
30. c. The limbal lesions in vernal keratoconjunc-tivitis are more papilliform because they have a central vascular core. When a central pit full of degenerated eosinophils forms, the term Horner-Trantas dot is applied. Herbert’s pits are depressed, necrotic follicles at the limbus. Many experts have maintained that corneal vernal disease rarely, if ever, leads to vascularization of the cornea. Superficial vascularization is far more common with trachoma, but it has been reported to occur in severe vernal keratoconjunctivitis as well. Debridement of giant palpebral papillae has been tried therapeutically, in an attempt to speed reepithelialization of shield ulcers. Typically, this fails, indicating that some factor other than mechanical irritation is at play. Some experts have suggested that inflammatory factors released by diseased conjunctiva may be responsible.
31. a. Other diagnostic criteria include bilateral conjunctival injection, injected pharynx, edema of upper or lower extremities, nonspecific rash, and lymphadenopathy. Fever for more than 5 days plus four of the other criteria must be present to make the diagnosis.
32. c. The vasculitis may involve the coronary arteries and lead to coronary artery aneurysm or occlusion.
33. b. The medial canthal tendon straddles the superior one-third of the nasolacrimal sac. Thus, dis-tention of the sac due to obstruction presents as a mass below the tendon.
34. c. Dacryocele, or congenital mucocele of the nasolacrimal sac, typically has a bluish-red hue, similar to a hemangioma, and results from chronic obstructive tear stasis. Recurrent conjunctivitis is far more common than dacryocystitis. Obstruction is nearly always at the inferior extreme of the nasolacrimal duct—the valve of Hasner (within the inferior nasal meatus). If it persists beyond 1 year of age, surgical intervention is generally required.
35. b. CHED occurs secondary to a defect of the corneal endothelium and Descemet’s membrane. Although the corneal epithelial edema and thickened stroma may resemble that seen in congenital glaucoma, there is no elevated intraocular pressure or increased corneal diameter. In congential hereditary stromal dystrophy (CHSD), the cloudy stroma is of normal thickness, and the epithelium is normal.
36. a. Lacrimal gland involvement can often occur in acute Epstein-Barr virus infection. The authors suggest it may be far more common than the 20% reported previously. Neither streptococcal nor diphtheritic infections tend to cause dacryoadenitis. Sarcoidosis never causes acute pharyngitis, and the dacryoadenitis is typically painless.
37. b. Corneal ulceration and scarring in familial dysautonomia (Riley-Day syndrome) is secondary to decreased or absent corneal sensation and decreased lacrimation.
38. a. Approximately two-thirds of the cases of infantile glaucoma are bilateral, and approximately two-thirds are boys. An affected parent has about a 5% chance of having a child with infantile glaucoma, and the next subsequent sibling has approximately a 5% chance of being affected. The incidence of open-angle glaucoma in grandparents is no different from age-matched controls. There is controversy regarding the basic pathophysiologic mechanism underlying the cause of infantile glaucoma. Many anomalies in and around the chamber angle have been described.
39. b. Ruptures in Descemet’s membrane associated with infantile glaucoma are usually horizontal, and those associated with birth trauma are usually vertical. Although optic nerve cupping in infants may be reversible, the presence of an afferent pupillary defect carries a poor visual prognosis. Unlike adults, pressures in children over 20 mm Hg are suspicious for glaucoma.
40. d. Medication is used only for preoperative control of intraocular pressure in children. Definitive management consists of surgery.
41. d. Rubella IgM titers might be of value in a neonate, but IgG titers are not diagnostic because they are of maternal origin during the first 3 to 6 months of life. Glaucoma is not a feature of galac-tosemia or Refsum’s disease. Lowe’s syndrome must be considered.
42. d. Autosomal-dominant patterns are most frequently reported, but 15% have no family history. Aortic valvular insufficiency and aneurysm may be life threatening and should be treated with cardiac depressants and/or surgery. Mitral valve prolapse also may be found. Myopia, high astigmatism, or frank keratoconus is seen in association with ectopia lentis in many cases. Up to 60% of patients with rigorously diagnosed Marfan’s syndrome will develop ectopia lentis.
43. b. Homocystinuria is an elastosis and leads to hypercoagulability with thrombotic vascular occlusions. The elastosis also causes defective zonular function and ectopia lentis in 90% of patients. It is inherited on an autosomal-recessive basis.
44. a. Mentation is typically normal in Sturge-Weber syndrome, whereas ectopia lentis is unusual in Down’s and Edward’s syndromes.
45. b. Bilaterality makes a systemic condition more likely. Monocular cataracts rarely herald signifi-cant systemic derangements. Anterior lenticonus may be part of Lowe’s syndrome, but posterior lenticonus is usually isolated. Pigmentary retinopathy raises the possibility of congenital infections.
46. c.Monocular visual deprivation, most likely with nuclear cataract, is the most amblyogenic. Every visually significant infantile cataract should be operated on as soon as it is feasible. A complete systemic evaluation of a patient with bilateral congenital cataracts should rule out congenital rubella infection, hypocalcemia, Lowe’s syndrome, and trisomies.
47. d. Because of the high incidence of capsular opacification, many surgeons advocate primary posterior capsulotomy (at the time of cataract extraction).
48. d. Pauciarticular, early-onset patients are most likely to develop uveitis, but they are generally ANA positive, RF negative. Uveitis is rare in Still’s disease, which is more common in boys.
49. d. In immunocompromised patients, a high risk of systemic spread with severe complications exists and may be more likely if systemic steroids are used. Topical steroids may be used in immu-nocompromised patients.
50. b. Up to 50% of pediatric patients with posterior uveitis have ocular toxoplasmosis.
51. a. Acute arthritis is not a typical finding in acquired systemic toxoplasmosis.
52. c. In ocular histoplasmosis, there is no vitreous inflammation.
53. d. The infectious cycle generally starts with a child consuming sand or dirt contaminated by the feces of a house pet that ingested the organism (dogs more often than cats). A peripheral granuloma with overlying vitreous opacification and chronic uveitis are typical findings in toxocariasis. The uveitis may die down and leave a quiescent peripheral granuloma. The inflammation in the eye often flares after the larva dies, and corticosteroids are the drug of choice in the treatment of this condition.
54. d. Pars planitis is bilateral in about 75% of cases. Tuberculosis, Lyme’s disease, or syphilis may be the underlying cause, but the workup is usually negative.
55. a. The number of aqueous cells in the anterior chamber, and not the amount of flare, should be the basis for treatment with topical steroids. Topical steroids may worsen the cataract and will not reverse band keratopathy.
56. a. PHPV occurs frequently in small eyes, whereas retinoblastoma rarely occurs in association with microphthalmia.
57. d. Studies of the natural history of retinopathy of prematurity show that 65% of premature infants with birth weight <1,250 g will develop some stage of the disease.
58. b. Coats’ disease is more commonly unilateral than bilateral. Abnormal vessels must be present, either by direct examination or fluorescein angiography, to make the diagnosis of Coats’ disease.
59. d. Optic nerve hypoplasia, particularly segmental, is more common in children of mothers with diabetes. Central vision is usually good, but sector or altitudinal field defects are frequently present.
60. b. Flame-shaped nerve fiber hemorrhages are the one most common funduscopic finding. Whitecentered hemorrhages (Roth’s spots), cottonwool spots, optic disc swelling, and perivascular infiltration also may be seen but are less common. Choroidal infiltration is usually not ophthalmo-scopically apparent.
61. c. All of the gangliosidoses are autosomalrecessive diseases. Most patients die in their first decade of life.
62. c. The most common ocular disorder associated with Lowe’s syndrome is a characteristic small, thick, opaque cataract. Unlike Alport’s syndrome, Senior-Loken syndrome features a progressive retinal degeneration with profound visual symptoms.
63. b. It is felt that fewer ganglion cells decussate at the chiasm than in normal subjects. Albino patients with the tyrosinase-negative variety usually have severe photophobia and nystagmus. Visual acuity is usually <20/200. As the name implies, tyrosinase-negative albinos have no tyrosinase enzyme in their hair shafts or skin. Extensive vitreous syneresis, vitreous veils, and strands are common features of X-linked juvenile retinoschisis. Although electrophysiologic testing may show diffuse retinal involvement in sector retinitis pigmentosa, the condition rarely progresses, and the prognosis is good. This is reflected in normal B-wave implicit times.
64. b. Cone dystrophy is the most common bull’seye maculopathy
65. a. Retinitis punctata albescens is not a form of CSNB but is progressive (albeit more slowly than typical retinitis pigmentosa).
66. c. High hyperopia is associated with Leber’s congenital amaurosis. The oculodigital sign refers to a tendency to gouge the eyes with a finger or fist. It is felt that afflicted patients do this to provide entopic stimulation of the neurosensory retina. Five percent to 10% of patients with Leber’s congenital amaurosis have associated hearing loss.
67. b. With complete rod monochromatism, acuity is typically 20/200. With blue cone monochromatism, acuities are 20/40 to 20/200. The presenting symptom in Stargardt’s is usually decreased central visual acuity. Central vision is usually preserved in the pattern dystrophies. Nonrhegmatogenous retinal detachments occur with optic nerve pits, primarily involving the macula.
68. a. Aicardi’s syndrome is limited to females because it is X-linked dominant. It is lethal in male infants or fetuses.
69. d. The visual field defects usually correspond to the area of fundus ectasia (inferior or inferonasal) and are consequently in the upper temporal field. They often cross the midline, unlike chiasmal defects.
70. d. DeMorsier’s syndrome (septooptic dysplasia) is far more common in bilateral optic nerve hypoplasia. Most authorities feel that neuroimaging should be conducted in both unilateral and bilateral optic nerve hypoplasia.
71. c. Optic nerve pits are usually in the inferotemporal quadrant or central part of the disc.
72. d. Both CT scanning and ultrasonography will reveal the presence of disc drusen, if calcified. Red-free photographs are of no value. However, disc drusen do autofluoresce on fluorescein angiography. To elicit this, fluorescein barrier filters must be used with no injection. The visual fields of chronic papilledema and disc drusen may appear similar and are of less value.
73. a. The distinction between fibrous dysplasia and ossifying fibroma is generally made histologically. If osteoblasts are present, then the lesion is called an ossifying fibroma; if absent, the term fibrous dysplasia is applied.
74. c. This is a capillary hemangioma. Blood stagnation and phleboliths are characteristic of cavernous, not capillary, hemangiomas.
75. d. Surgery is not prudent unless absolutely necessary because these tumors are difficult to remove completely and have a propensity to hemorrhage.
76. d. Wilms’ tumor, neuroblastoma, and rhabdomyosarcoma are the three most common solid pediatric malignancies. Leukemia is the most common of all pediatric malignancies. The average age at diagnosis is 7 years old. An unexplained mass in the lids or acquired ptosis in a child should prompt radioimaging to rule out rhabdomyosarcoma.
77. c. Differentiated rhabdomyosarcoma in the least common type but has the best prognosis. The embryonal type is the most common. The initial intervention of newly diagnosed rhabodo-myosarcoma is radiotherapy and chemotherapy. Exenteration is reserved for treatment failures and recurrences.
78. b. A minority of patients with neurofibromatosis (1.5%) will develop a schwannoma. It rarely undergoes malignant degeneration. The two classic histologic appearances are Antoni A (regular arrangement of eosinophilic spindle cells with palisading nuclei) and Antoni B (haphazardly arranged stellate cells in a myxomatous matrix). Perineural spread and compression account for pain.
79. d. Plexiform neurofibroma is most specific for neurofibromatosis. Unlike schwannomas, neurofibromas grow independent of peripheral nerves. In addition, they are generally osteolytic.
80. a. The tumor presents with metastases in about one-third of patients.
81. b. Enophthalmos is characteristically seen with metastatic scirrhous carcinoma of the breast in adult women.
82. c. Homer-Wright rosettes are usually not seen in orbital metastases, being limited to the better differentiated primary tumor.
83. a. Even with metastases to the liver, bone marrow, and spleen, survival may be as high as 84%. Bone metastasis is a poor prognostic factor. Age at onset is the most powerful predictor of survival with age <1 year a poor prognostic factor.
84. c. Opsoclonus (‘dancing eyes’) is the paraneo-plastic syndrome most commonly associated with metastatic neuroblastoma.
85. a. Ewing’s sarcoma is a primary intramedullary malignancy of bone, and periocular metastasis usually presents with proptosis, hemorrhage, and inflammation from tumor necrosis. It occurs in individuals 10 to 25 years of age, older than the population with neuroblastoma. Usually, there is no globe involvement, and treatment is principally chemotherapy, although radiation to remote sites has been used with some success.
86. a. The most common location is the superotemporal orbital rim, in association with the zygo-matic–frontal suture line.
87. c. One study of 302 epibulbar lesions removed from children <15 years of age reported the following frequencies:
Nevus, 29%
Dermoid, 19%
Epithelial inclusion cyst, 11%
Dermolipoma, 10%
Pyogenic granuloma, 6%
88. d. Retinoblastoma occurs in approximately 1 in 20,000 births. Only 6% have a positive family history. The familial tumors appear to be inherited in an autosomal-dominant pattern with 80% penetrance. Thus, the offspring of a patient with bilateral retinoblastoma has approximately a 40% chance of developing a tumor (80% of 50%).
89. c. With no family history and healthy parents, this child probably suffered a germline mutation of chromosome 13. His parents’ copies are probably normal. Again, genetic counseling is complex, but the following generalizations serve as guidelines:
1. Healthy parents with one affected child have a 6% chance of producing more affected children.
2. If two or more siblings are affected, this implies a chromosomal defect in one parent. Thus, each additional child has a 40% chance of inheriting the tumor.
3. A parent with bilateral retinoblastoma has a 50% chance of transmitting the affected chromosome to his or her children. With 80% penetrance, 40% of offspring will be affected phenotypically.
90. d. See answer 89.
91. a. Patients who are postradiation therapy for retinoblastoma are susceptible to many malignancies, most notably osteogenic sarcoma. Life expectancy in patients who develop a second malignancy after treatment for retinoblastoma is markedly diminished.
92. d. Although the presenting symptoms and signs depend on the extent of the tumor, the frequency of some of the presenting signs and symptoms are summarized below, with leukocoria and strabismus presenting the majority of the presentations:
Leukocoria, 60%
Strabismus, 22%
Decreased vision, 5%
Incidental finding, 4%
Orbital cellulitis, 2%
93. c. Growth into the vitreous is termed endophytic (endo-, toward the inner retina). Growth in the direction of the sclera is exophytic (exo-, toward the outer retina). The rapid tumor growth exceeds the blood supply. Necrosis occurs with preservation of cells around blood vessels. Although the course of retinoma is benign, the fellow eye may show a retinoblastoma, and the genetic implications are identical. This relationship between pineal gland neoplasms and retinoblastoma is common enough to be labeled “trilateral” retinoblastoma and likely represents a primary malignancy of the pineal gland.
94. b. Given the acidic nature of nuclei acids, they will be basophilic.
95. d. Direct spread into the optic nerve and CNS is most common. Bone metastasis is seen in over half of metastatic cases. Lymph node metastases are the second most common.
96. c. Cryotherapy is as effective as photocoagulation for small tumors difficult to manage with photocoagulation.
97. b. The only medulloepitheliomas associated with significant metastatic risk are those that extend into the orbit.
98. c. This is a classic photo and description of a choroidal osteoma. These tumors are composed of mature bone; they commonly become yellow-white by the late teenage years (secondary to overlying RPE atrophy).
99. c. The photoreceptors should not be affected, and the ERG will be normal.
100. b. Adenoma sebaceum consists microscopically of an angiofibroma and may be confused with acne vulgaris.
101. d. The seizures are contralateral (secondary to the presence of leptomeningeal hemangioma overlying the ipsilateral cerebral convexity). Diffuse choroidal hemangioma is classic, leading to the so-called tomato catsup fundus. Focal choroidal hemangioma is also seen in this disorder but is more frequently isolated. The glaucoma is very likely from elevated episcleral venous pressure, but it has not been shown to be the sole cause (or even a definitive primary cause). Some patients have less elevated EVP with an angle anomaly. Rubeosis may occur later in the disease course, as well. In Sturge-Weber syndrome, the retina overlying a diffuse hemangioma may develop serous detachment or ischemia and provoke neovascularization.
102. b. 20% of patients with capillary hemangiomas of the retina develop hemangioblastomas of the cerebellum.
103. d. The others are autosomal dominant, except for Sturge-Weber syndrome, which is sporadic.
104. a. Optic nerve atrophy—from chronically high intracranial pressure or abnormalities of the optic canal—has been described, but hypoplasia is not a common finding.
105. c. V-pattern exotropia is common among the craniosynostoses. Abnormalities in the development and origins of the extraocular muscles make correction of the strabismus very difficult.
106. b. The findings of this deformity/anomaly are present in a number of specific syndromes.
107. b. These are features of Treacher Collins’ syndrome.
108. b. This is an example of a patient with fetal alcohol syndrome. Primary telecanthus may be seen, but not hypertelorism. Also note the long flat philtrum, midface hypoplasia, and mild ptosis that are characteristic of this syndrome.
109. c. The superior oblique and the levator muscles each arise posteriorly, above the annulus. The inferior oblique arises from the anteromedial orbital floor. The annulus gives rise to the four rectus muscles.
110. d. The horizontal rectus muscles have no torsional or vertical action in primary gaze. In upgaze, they are elevators (weak); in downgaze, they are depressors (weak).
111. d. With the eye abducted 23 degrees, the superior rectus is parallel to the visual axis, and its contraction will result in maximal elevation. For the same reason, in this position the inferior rectus is maximized as a depressor. In primary gaze, contraction of the superior rectus not only elevates the eye, but also intorts and adducts the eye. (The inferior rectus will extort and adduct the eye, as well as depress it, in primary gaze.)
112. a. With the eye adducted 51 degrees, the tendon of the superior oblique is parallel to the visual axis, and its contraction will result in maximal depression. For the same reason, in this position the inferior oblique will be maximized as an elevator. In primary gaze, contraction of the superior oblique not only depresses the eye, but also intorts and abducts the eye. (The inferior oblique will extort and abduct the eye, as well as elevate it, in primary gaze.)
113. b. The inferior oblique’s anatomic and mechanical origins are the same—from the anterome-dial orbital floor. The superior oblique has its anatomic origin at the orbital apex. Its mechanical origin is at the trochlea, since this is where its effective force is generated. The oblique muscles always run below the corresponding rectus muscle. By the time it reaches the trochlea, the superior oblique is already tendinous.
114. a. The superior muscles act as intorters, whereas the inferior muscles act as extorters. The oblique muscles are more important for torsion than the vertical recti. Thus, the primary intorter of the globe in primary gaze is the superior oblique.
115. c. The belly of the superior oblique is approximately 32 mm (the others are 37–40 mm).
116. c. Because the superior rectus is loosely attached to the levator complex, recession will pull the levator back and widen the fissure, whereas resection will pull the levator forward and narrow the fissure. The same relationships apply for the inferior rectus because its sheath gives rise to the capsulopalpebral fascia. Operation on the superior oblique should not affect the palpebral fissure.
117. b. The main synergist of the superior rectus is the inferior oblique (both elevate the globe).
118. b. Hering’s law of yoke muscles states that “yoked” muscles (contralateral) must always receive equal innervational input. Sherrington’s law states that innervation to an (ipsilateral) antagonist decreases as innervation to the agonist increases. In DVD, the affected eye drifts up under cover. When the cover is shifted to the other eye, if Hering’s law is followed, yoke innervation should generate a contralateral hypotropia. This is not seen in DVD for reasons that are unclear.
119. d. In Duane’s syndrome, innervational impulses to the medial rectus are not associated with decreased innervation of the ipsilateral lateral rectus muscles, as Sherrington’s law demands. This is because of anomalous innervation of the lateral rectus, in this case from the oculomotor (III) nerve, which leads to coinnervation of the horizontal rectus muscles, with globe retraction on adduction.
120. b. The impulse originates in the left frontal lobe.
121. d. Note that saccades are generated contralaterally, whereas pursuits are generated ipsilaterally
122. d. Within a certain range around the empirical horopter, that is, Panum’s space, objects will be perceived as one, with stereopsis. Any point on the horopter must be perceived singly. If simultaneous stimulation of two retinal areas leads to perception of one image, then sensory fusion is said to exist. If the two retinal areas have identical topographic locations relative to the fovea, then normal retinal correspondence exists. If abnormal or anomalous retinal correspondence is present, simultaneous stimulation of two areas of retina that do not have the same topographic relation to the fovea (noncoresponding) still leads to perception of one image (sensory fusion). If the two images are sufficiently different, visual confusion will be created.
123. c. Normal divergence amplitudes at distance is 6 prism diopters. At near, this increases to 16 prism diopters.
124. d. This is a classic example of retinal rivalry.
125. c. Approximately 1 in 50 people suffers from amblyopia. The incidence of strabismus, with or without amblyopia, is slightly higher, at 1 in 25 to 30. Afferent pupillary defects may be seen in amblyopia of any cause but should heighten suspicions about an organic lesion. “Crowding” refers to poorer recognition acuities in amblyopia when targets are presented multiply rather than singly. Neutral density filters will not significantly affect vision in amblyopes, unlike patients with maculopathy.
126. c. Amblyopia in Duane’s syndrome is uncommon but is more likely than in alternating esotropia, where each eye shares the visual workload.
127. b. Cyclic esotropia is rarely accompanied by amblyopia. Parafoveal fixation is difficult to assign to factitious etiologies. All of the findings described (mild amblyopia, mildly impaired stereopsis, peripheral fusion, eccentric fixation with a central suppression scotoma) are typical of a microtropia (the tropia is either too small to detect or does not exist due to parafoveal fixation and anomalous retinal correspondence).
128. c. Microtropia is most commonly seen after successful (or nearly so) strabismus surgery, as well as in the setting of anisometropia.
129. d. A weak base-out prism will shift a fixation target nasally. If placed over the microtropic eye, the shift will not move the target out of the suppression scotoma, and no refixation movement is generated. When placed contralaterally, both eyes will shift away from the base of the prism. No fusional convergence will be seen contralaterally because of the central scotoma. In normal eyes, the contralateral eye converges to fuse the fixation images.
130. d. Esotropia gives uncrossed diplopia on red glass testing. Thus, the left light (red) should appear to the left of the right light (white).
131. d. It is better to flash the vertical line into the deviated eye because displacement of a horizontal line may be missed with a suppression scotoma. If there is eccentric fixation, the test is more difficult to interpret. In right exotropia and ARC, the image the patient sees with the right eye (vertical) will be displaced to the right (because it lies on the anatomic fovea, nasal to the “pseudofovea” of ARC).
132. b. There is no manifest deviation (tropia, cover–uncover test) but a latent esodeviation (phoria, alternate-cover test).
133. d. In the setting of an esotropia (detected by cover–uncover test), the alternate-cover test must disclose some strabismus because it detects both tropia and phoria. The cover–uncover test detects only tropia. Most of the normal adult population has a small phoria, more often exophoria.
134. d. The Krimsky test uses prisms over the fixating eye to center the light reflex over the pupil in the deviating eye. Foveal fixation is not required.
135. b. Each millimeter of decentration is 7 degrees of deviation. Each degree is approximately 2 prism diopters. Thus, each millimeter is approximately 15 prism diopters. Three millimeters is 21-plus degrees, or 45 prism diopters. Because the reflex is displaced temporally, the eye must be deviated inward (esotropia).
136. d. As the fixing eye is covered, a prism is simultaneously placed over the deviated eye. When there is no refixation shift, the prism has neutralized the tropia. The alternate-cover test with prisms will neutralize total phoria plus tropia. The cover–uncover test with prisms will neutralize tropia plus part of the phoria.
137. d. In excyclotropia, the superonasal retinal quadrant is rotated vertically toward the 12 o’clock position, and the inferotemporal quadrant is rotated toward the 6 o’clock position. The vertical line from the Maddox rod will run superonasal to inferotemporal on the retina and be perceived the same way.
138. a. In the Lancaster red-green test, the fovea of each eye is isolated with duochrome glasses. The eye under green glass (left) will not see the red light and the eye under the red glass (right) will not see the green light. By holding the green light centrally, the examiner holds the patient’s left fovea centrally. Assuming normal retinal correspondence (NRC), the patient will direct the red light in space along his right visual axis to place the red light on his right fovea and superimpose the foveal images. The patient’s right visual axis (in esotropia) crosses his left visual axis, so the right foveal image will fall to the left of the left foveal image (as seen by the examiner). To the patient, the images appear superimposed (assuming NRC).
139. d. This is true because the strabismus is acquired. In that case, we can assume NRC and central fixation.
140. d. In this case, the deviated right eye is fixing centrally (green glass). The larger secondary deviation, a left esotropia of greater magnitude, will cause the red light (left foveal image) to appear to the right of the green light (right foveal image).
141. d. The first three tests utilize actual fixation behavior and will not fall victim to large angle kappa or facial anomalies. The Krimsky and Hirschberg methods use apparent eccentricity of pupillary reflexes and may be misguided by these factors.
142. b. The base of the prism is always placed opposite to the direction of the deviation.
143. d. A 25-prism-diopter increase in esotropia from distance to near is almost certainly a high AC/A ratio; a patient whose distance esotropia increases by more than 10 prism diopters at near is said to have a clinically high accommodative convergence to accommodation ratio (AC/A).
144. c. By the gradient method, AC/A ratio equals the difference in the deviation induced by a lens divided by the specific accommodative gradient (of an extra lens over the distance correction). Minus lenses stimulate accommodation, whereas plus lenses blunt it. Here, 50-35 divided by 1 = 15:1.
145. b. By the heterophoria method, the AC/A ratio equals the near deviation minus the distance deviation divided by the accommodative demand at near, plus the pupillary distance (PD) in centimeters. Here, this is 35 – 10 = 25, divided by 5 (reading at 20 cm) = 5 plus 6 (PD in cm) = 11:1.
146. a. This patient presents with right hypertropia in primary gaze. Three step testing is presented here. The right hypertropia is worse on left gaze and worse on right head tilt. This maps to a right superior oblique palsy. In straight upgaze, there is a small exotropia or V pattern from the secondary abducting action of the overacting inferior oblique. In gazing down and to the patient’s right, the left eye is slightly lower, reflecting the slight overaction of the normal left superior oblique muscle. This may be caused by a contracted or tight right superior rectus muscle from the chronic, longstanding higher right eye. The overaction of the opposite superior oblique is a common finding in these patients.
147. c. The clinical findings of mydriasis and accommodative paresis indicate damage to the para-sympathetic supply to the globe. These nerves travel with the nerve to the inferior oblique before forming the short root of the ciliary ganglion. The motility findings in this case indicate a probable inferior oblique palsy (inability to elevate the adducted eye). The three-step test should show a left hypotropia (right hypertropia) worsened in right gaze and right head tilt.
148. d. Exaggerated sensitivity to cholinergic blockade has been reported in albinos and patients with Down’s syndrome. Infants are also particularly sensitive. Atropine is a treatment for heart block (acutely) and should not cause arrhythmias in patients with this disorder.
149. c. Atropine’s central nervous system side effects include both alerting/agitation and somnolence. Flushing and tachycardia are particularly common in infants.
150. a. This is a classic example of infantile esotropia. With cross-fixation, amblyopia is less likely to develop because the youngster will use each eye at different times. An accommodative component may be discovered in many cases of infantile esotropia. There is usually a large esotropia measuring more than 30 prism diopters as seen in this clinical photograph.
151. b. Latent nystagmus, overacting inferior obliques, and DVD are such common concomitants that they should be specifically sought in the examination of a child with infantile esotropia. A high AC/A ratio may be seen but is not typical.
152. d. Surgery for esotropia must provide either weakening of the medial rectus muscles (recession) or strengthening of the lateral rectus muscles (resection). Recession always has a greater effect than a resection of the same amount. Thus, bimedial recession is generally performed before bilateral resection. In some cases, however, bilateral resection may be the first procedure (for instance, in esotropia that is greater at distance). Combined medial and lateral resection is an equally effective alternative.
153. b. Amblyopia is certainly possible given the constant esotropia. A large-angle turn might provide cross-fixation, but amblyopia must be ruled out. Given the age of onset, an accommodative component is likely, so an originally intermittent turn is also possible. No patient with manifest strabismus has any stereopsis whatsoever. Certainly, a family history of esotropia of any mechanism is possible.
154. c. This patient probably has refractive accommodative esotropia. Amblyopia is possible bilaterally, given the high ametropia in both eyes. The deviation may be greater at near than distance, but this is not highly likely because patients with refractive accommodative esotropia typically have normal AC/A ratios. In this type of esotropia, the turn is usually moderate (20 to 40 prism diopters), although it may be greater. +3.00 lenses may lessen nonrefractive accommodative esotropia but typically have little effect on this type (with +3.00 lenses, there would still be a residual 5 D of hyperopia).
155. b. In all cases of accommodative esotropia, full hyperopic correction is warranted immediately. Penalization with atropine may be useful in cases of noncompliance with spectacles and/or patching therapy. Bifocals may be of value with high AC/A ratio with a residual turn at near after full correction.
156. d. This is probably a case of nonrefractive accommodative amblyopia (intermittent turn, worse at near, with normal refractive error and high AC/A ratio). +3.00 D lenses for near work will relieve the accommodative demand and prevent accommodative convergence from causing an esotropia.
157. d. Surgery is necessary in virtually all cases of infantile esotropia, whereas many cases of pure accommodative esotropia will resolve with time and refractive correction. Bifocals are generally most helpful in nonrefractive accommodative esotropia, where high AC/A ratios make the esotropia worse at near. If full refractive correction is not the solution, some experts advocate atropine penalization with full correction or pilocarpine treatment to provide accommodation without convergence. These steps frequently fail, however, and are controversial.
158. c. Age of onset between 2 and 3 years makes an accommodative mechanism more likely, with better prognosis for refractive correction. The other findings are consistent with a large-angle, congenital esotropia.
159. b. Persistent esotropia on pilocarpine treatment may be seen in accommodative esotropia, so spectacle correction must always be attempted. Surgical results are much more stable and predictable in the setting of maximal visual acuity (after occlusion therapy). Surgical realignment resulting in a residual esotropia of <10 prism diopters may permit the development of peripheral fusion.
160. c. Correction with full hyperopic prescription may weaken the patient’s fusional divergence, which is the force keeping accommodative esotropia intermittent at its outset. Then, the esotropia may become constant without the “crutch” of the spectacles.
161. d. Divergence insufficiency is indistinguishable from sixth nerve palsy, except it is typically comitant. Sixth nerve palsy is more likely to have an esotropia at near as well.
162. c. New myopia favors the diagnosis of spasm of the near reflex; the myopia may be hard to establish if the spasm is intermittent, but the miosis is detectable and is the diagnostic “clincher.” Also, the angle of turn is highly variable and unpredictable.
163. c. Unless the palsy is acquired early in childhood, goes untreated (with occlusion), and/or does not resolve, amblyopia is highly unlikely. Some children will develop a permanent esotropia after abducens palsy, probably representing a decompensated esophoria. Thus, all cases must be followed to resolution. Although many experts will obtain timely neuroimaging tests (CT/MRI), abducens palsy in a child is a common postviral syndrome and typically resolves uneventfully. The second most common etiology is increased intracranial pressure (central nervous system mass lesions, pseudotumor cerebri).
164. b. Exotropia that is equal at distance and near is basic. If the deviation is greater at near, then it is termed convergence insufficiency exotropia. If it is greater at distance than near, it is termed divergence excess exotropia.
165. d. Divergence excess exotropia may be divided into two subtypes. In some cases of divergence excess exotropia, the turn appears larger at a distance because of enhanced fusional convergence at near related to accommodation. Interrupting fusion with prolonged occlusion (>30 minutes) or relaxing accommodation with plus lenses may cause the deviation at near to increase to a measurement similar to the original distance measurement. This is simulated divergence excess. If these manipulations have no effect (i.e., the distance measurement is still larger), true divergence excess is said to exist.
166. a. Most constant exotropia is intermittent originally.
167. d. High AC/A ratios develop as a fusional mechanism for near work. The turn in intermittent exotropia is highly variable and sensitive to external stimuli. Bright light typically causes reflex closure of the deviating eye. Amblyopia is highly unlikely if the turn is truly intermittent.
168. c. Minus lenses stimulate accommodation and may provide the extra convergence needed for fusion. Base-in prisms may permit fusion but are not advocated by all investigators because they may weaken fusional convergence and convert an intermittent to a constant deviation. Phospholine plays a role in accommodative esotropia, not exotropia. Lateral rectus resections strengthen the lateral rectus and will exacerbate exotropia.
169. c. By definition, convergence insufficiency is a latent deviation, not a manifest one. (This is not the same entity as convergence insufficiency exotropia, which is a manifest deviation.)
170. b. The left eye deviates upward under cover, and the right eye deviates downward under cover. This is a left hyperdeviation or a right hypodeviation.
171. d. DVD simulates a hyperphoria but violates Hering’s law. When covered, the left eye drifts up. When uncovered, the left eye moves down to assume fixation. By Hering’s law, the yoke muscles of the right eye, depressors, should receive equal innervation as the left eye moves down. The right eye should be deviated downward under cover (right “hypo”) and move up to reassume fixation when the cover is shifted back to the left eye. This does not occur, consistent with dissociated vertical divergence. (The dissociation refers to the violation of Hering’s law with dissociation of yoke muscles.) DVD is a frequent concomitant of infantile esotropia and frequently is made manifest only when visual input to the affected eye is interrupted (occlusion, amblyopia, other organic disease). The deviation is highly variable and difficult to measure, making surgery difficult to quantify accurately.
172. c. This set of findings is not particularly unusual in infantile esotropia. There are two potential explanations for the vertical deviation in lateral gaze. The first is overaction of the inferior obliques. In this condition, on lateral gaze, there is hypotropia of the abducted, non-fixing eye. In DVD, in lateral gaze, there is no associated hypotropia, in violation of Hering’s law. In fact, if the DVD is bilateral, there may be hyperdeviation of the abducted, nonfixing eye. The distinction between the two is important for surgical planning.
173. d. Head tilt and excyclotorsion are not uncommonly seen in unilateral cases and are not useful. V, not A, pattern esotropia results from underaction in downgaze and subsequent unopposed adduction in downgaze by the inferior rectus. In unilateral superior oblique palsies, lateral gaze toward the involved side generally relieves the diplopia. Aggravation of diplopia in both directions argues for bilateral involvement, as does aggravation with head tilt in either direction.
174. c. Surgical management of superior oblique underaction is generally aimed at weakening the ipsilateral inferior oblique (myectomy) and/or strengthening the ipsilateral superior oblique. If the hyperdeviation is >35 prism diopters in primary gaze, then strengthening the ipsilateral inferior rectus or weakening the ipsilateral superior rectus may be of value. Contralateral superior oblique weakening also may be useful in certain cases.
175. d. This procedure, the Harada-Ito procedure, increases the force vector for incyclotorsion by moving the lateral half of the insertion of the paretic muscle. It has no effect on vertical eye movement or fusion.
176. c. Two muscles may nearly always be safely removed. Removal of four muscles is highly likely to cause significant ischemia. Removal of three muscles is likely to lead to some degree of ischemia.
177. a. Snellen figures, particularly presented in rows, are the most challenging, and perhaps most relevant, type of acuity test.
178. c. Double elevator palsy may be primarily due to elevator weakness or to restriction of the depressors. Ptosis, hypotropia, and poor elevation in any direction are characteristic. A subset will have positive forced ductions for the inferior rectus. Head position is generally an automatic compensation for the hypotropia, with the chin up.
179. c. In Brown’s syndrome, elevation is limited in adduction, but not in abduction. Duction testing mimics paresis of the ipsilateral inferior oblique.
180. a. Enophthalmos is frequently cosmetically unacceptable. In the acute setting, there may be proptosis, but this usually gives way to enophthalmos as swelling subsides.
181. d. For an A deviation to be significant, the difference in measurements between upgaze and downgaze must exceed 10 prism diopters. For V patterns, the difference must measure 15 prism diopters. Approximately 15% of horizontal strabismus cases have a significant A or V component.
182. d. In V pattern exotropia, one should search for overaction of the inferior obliques or underaction of the superior obliques. If neither is present, then lateral rectus recession and medial rectus resection should be performed with downward transposition (toward the Apex of the V) of the Medial rectus insertion, by one-half the insertion width, and upward transposition (toward the Empty space of the V) of the Lateral rectus insertion, again by half the insertion width. The mnemonic for this is MALE: Medial rectus toward the Apex and Lateral rectus toward the Empty space. This holds for both A patterns and V patterns.
183. a. In V pattern esotropia with overacting inferior obliques, inferior oblique myectomy will cause 15 to 25 prism diopters of esoshift in upgaze. This only makes the deviation more comitant. Thus, the deviation in primary gaze must be addressed with appropriate medial rectus recession and lateral rectus resection. Because oblique surgery is indicated, rectus transpositions are not.
184. a. The etiologies for pediatric third nerve palsy, in descending frequency, are congenital, trauma, inflammation, migraine, and neoplasm.
185. a. The etiologies for adult third nerve palsy, in descending frequency, are microvascular, aneu-rysm, trauma, and neoplasm.
186. d. Because muscle surgery, particularly the vertical muscle surgery often indicated in Graves’ disease, can affect the position of the eyelids, it is generally wise to perform any strabismus surgery before eyelid repositioning. For instance, some of the lid retraction seen in affected patients may be directly attributable to superior rectus overaction (with subsequent lid retraction) attempting to counter inferior rectus contracture.
187. a. Jerk nystagmus has clearly biphasic velocities—fast in one direction and slow in the other. Disconjugate nystagmus has different amplitude and/or frequency in one eye relative to the other. Uniplanar nystagmus is, as its name implies, present in one plane only, usually horizontal.
188. d. The nystagmus of spasmus nutans is typically small in amplitude but characterized by its disconjugate nature. It may appear to be entirely monocular and raise the specter of chiasmal or hypothalamic glioma. The other findings in the triad include head bobbing and torticollis.
189. b. Many pediatric ophthalmologists will obtain neuroimaging tests of children with monocular nystagmus, unless combined with obvious head bobbing and torticollis. Cases of anterior visual pathway glioma associated with head bobbing have been reported.
190. c. This combination of prisms will force the child to gaze to the right in order to see objects straight ahead. This will obviate a head turn, which is typically the end point of treatment.
191. d. This may be a case of partially or totally accommodative esotropia, which will respond nicely to hyperopic correction. Bifocals might be added later if a significant residual esodeviation remains at near with distance correction. Any amblyopia, must be treated aggressively with careful follow-up of the treatment effect on each eye.
192. c. Stimulation of accommodative convergence is unlikely to resolve the problem. Because the parents are determined to correct the cosmetic problem, and because the deviation is greater in left gaze, weakening of both lateral recti, more so on the left, should be undertaken.
193. d. Strengthening the ipsilateral superior rectus will aggravate the right hypertropia. A common approach might be the superior oblique tuck alone (if the deviation is <25 prism diopters) or combined with inferior oblique tenotomy (if >25 prism diopters).
194. a. Although this probably represents a case of basic esotropia, there may be an accommodative component. There is no way to rule this out without a trial of hyperopic correction. Bifocals might be added later if a significant residual esodeviation remains at near with distance correction. Early surgery might be advocated to maximize the retention of fusion, but only the angle of deviation that remains after refractive correction should be addressed. Close follow-up, as always, is critical.
195. d. Because there is asymmetric vision due to amblyopia, a right-eyed procedure should be chosen (to minimize operative risks on the better-seeing left eye). The guidelines for a 30-prism-diopter esotropia are 4.5 mm medial rectus recession and 7 mm lateral rectus resection.
196. d. Monocular surgery is preferable. The guidelines for a 30-prism-diopter exotropia are 6 mm of medial rectus resection and 7 mm of lateral rectus recession.
197. c. Acquired forms of strabismus may be associated with troublesome postoperative strabismus, as images are moved closer but not close enough. In congenital cases, suppression will prevent the complication. The prism adaptation test is indeed valuable for predicting postoperative behavior. Undercorrected intermittent exotropia will be associated with suppression and a quick recurrence of large-angle turns. The most annoying diplopia is frequently due to small-angle residual turns, which are manageable with prisms. Many cases will resolve spontaneously over months.
198. d. Consecutive exotropia due to overcorrection alone should not be associated with striking impairment in adduction.
199. b. Elevated body temperature is a relatively late sign. Careful surveillance for the earlier signs is critical.
200. c. Ptosis is the most common and is seen slightly more frequently in children. Secondary vertical strabismus is the second most common complication.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


