Fig. 73.1
Michelson Diagnostics VivoSight OCT probe
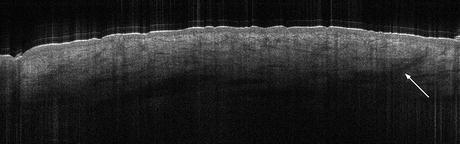
Fig. 73.2
OCT image of healthy skin at the forearm. The first superficial layer is the epidermis. The dermis shows signal poor longish or round structures corresponding to lymphatic and blood vessels. Hair follicles cross the dermis in an oblique way (arrow). Image size 6 × 1.9 mm (This and all other images in this chapter were obtained using a VivoSight OCT scanner)
Also available are the Agfa SKINTELL [9], which has CE mark, and LLTech Light-CT [10], which is aimed at scanning excised biopsy samples. They both feature high-NA objective lenses, potentially enabling visualization of more clinical detail, but at the expense of being quite bulky.
The rapid growth of installed commercial scanners will surely lead to growth in the number of research publications supporting a wide variety of clinical applications.
73.2.3 Polarization-Sensitive OCT
An important constituent of skin tissue is collagen, which is highly birefringent. The collagen fibers themselves are very small and difficult to resolve optically unless very high-NA optics is used. Polarization-sensitive OCT has been studied for possible use in managing burns [21], because heat denatures the collagen, and studying dermal response to cosmetic treatments [22]. A difficulty is that the images are quite hard to interpret visually.
73.2.4 Doppler OCT and Speckle Variance OCT
The use of phase-sensitive OCT for detection and quantification of fluid flow, especially blood flow, has been widely studied. The theory of Doppler OCT is discussed in detail elsewhere in this book. For dermatologists, imaging blood flow has many advantages and potential applications. There are many clinical conditions, and treatments for them, in which inflammation occurs resulting in increased blood supply to the affected region. OCT could be of use to monitor the effects of the treatment by showing the reduction in blood flow.
In addition, some conditions result in abnormal blood vessel growth, such as port-wine stains, rosacea, and, perhaps most importantly, tumors. Thus, there is a clear clinical need to image blood vessels. Although these are visible in “ordinary” OCT images as dark streaks and have some diagnostic value, techniques that can highlight areas of flow and even quantify it would have more clinical value.
Doppler OCT is exquisitely sensitive, and some remarkably detailed images of blood vessel structures in skin have been obtained [11]. However, it suffers from two problems. The first of these is that it is almost too sensitive: even the tiniest motion of the subject with respect to the probe produces a huge background signal. The excellent images produced to date have been obtained by “clamping” the probe to the subject, which is not a clinically useful technique. While some work has been done on motion compensation, oversensitivity has so far prevented use of Doppler OCT in practical clinical instruments. A second problem is that by its nature Doppler OCT measures flow parallel to the interrogating beam, which is normally perpendicular to the skin surface, but most blood flow is at 90° to that. In the worst case, only vertically oriented blood vessels can be seen in the image.
More recently, a technique known as speckle variance OCT has been studied [12]. Here, the intensity variance between consecutive images of the same tissue is calculated, the idea being that stationary tissue produces a stationary invariant speckle pattern, whereas blood produces rapid changes. Very impressive images of the “arboreal” blood vessel structures produced by a basal cell carcinoma have recently been produced [13]. However, this approach also suffers from sensitivity to background subject motion, and more work is required. There is also a problem that unlike Doppler OCT, the rate of flow cannot be easily quantified from the speckle variance signal. This may or may not limit its clinical value.
Despite these limitations, it seems inevitable that with further development, blood-flow imaging with OCT will eventually reach the clinic in practical instruments for routine use, and the clinical benefits are potentially huge.
73.2.5 Elastography OCT
Elastographic OCT has also been studied [14, 15]. Here, a mechanical stimulus is applied to the skin and the response in the OCT image observed, for example, by detecting the change or movement in the laser speckle pattern in the image. Researchers claim that it is thereby possible to distinguish regions of the skin that have different Young’s modulus, and this may have clinical applications.
73.2.6 Gels and Optical Clearing
Due to differences in the refraction between air and skin, the skin surface reflects at 1,300 nm and so there is typically a large “entrance signal” at the skin/air boundary. This is undesirable, because the bright reflection can wash out surface detail such as the thin stratum corneum, can saturate the detection electronics leading to artifacts, and reduces the “light budget” available for probing deeper into the tissue. There are various approaches to addressing this problem. One approach is to use a contact probe, i.e., the probe has a transparent surface that directly contacts the skin, so that there is no air/skin interface. For this to work well, a fluid such as water or ultrasound gel is typically used to ensure an airtight interface and for refraction index matching, because skin has a similar refraction index of about 1.33 compared to water.
Simply coating the skin with gel also has some benefit in reducing the entrance signal. On the other hand, a gel could modify the skin or confuse the viewer into thinking it is a feature of the skin itself. It remains to be seen whether clinical users feel that use of gel is worth the effort.
Vargas et al. reported that glycerol or other chemicals can have a beneficial effect in improving the depth penetration [16]. This is attributed to hydration of the tissue resulting in index matching. However, the effect takes time to have a useful effect and is unlikely to be adopted in busy dermatology clinics.
73.3 Image Interpretation
Although some features of the skin can be readily discerned such as sweat ducts, dermal/epidermal junction, etc., understanding of the presentation in OCT images of many common clinically important features is still developing and being studied. This is critical in order for the images to be used in the clinic on a routine basis. For example, it must be clearly understood not only how common pathologies such as basal cell carcinoma (BCC) nests present in the images but also similar but benign growths and variations of the most common types such as sclerodermiform BCCs. More generally, the principles behind how and why given tissue types appear as they do must be researched and understood. This is a topic of very active current study.
In general, OCT images reveal tissue morphology, but not details of individual cells (Fig. 73.2). In skin, we observe the following, based on detailed correlation with histology:
Intensity: Some tissue types appear brighter, others darker. Brighter tissue is more strongly scattering. Darker tissue is more weakly scattering and/or absorbing. Collagen-rich scar tissue is often brighter in appearance. In addition, some features like keratosis or calcification can cast shadows on the tissue below them. Blood and lymphatic vessels are usually dark due to the absorption by water.
Layers: Skin is a layered structure and these layers can often be discerned, especially the dermal/epidermal junction. Distortion of layers or damage to or absence of layer junctions can be strongly indicative of disease.
Shapes: Dermatological appendages such as hair follicles and sebaceous glands can be identified by their shape, coupled with intensity. This also applies to diseased tissue. For example, basal cell carcinomas typically present as dark ovoid features with a slightly darker rim, whereas cysts are typically circular with a bright wall. Vessels appear as dark streaks.
Texture: Different tissue types exhibit characteristic textures. Cancerous tissue is usually devoid of texture; healthy tissue is often mottled in appearance. Scar tissue has a swirly appearance.
Location: The location of features can also have diagnostic value. Dark streaks suggestive of blood vessels located unusually near the surface and close to an ovoid structure may well indicate a tumor.
These and other indicative features have been documented in an “OCT Manual” published by Michelson Diagnostics with contributions from leading dermatologists and freely available on the Internet [17].
73.4 Applications of OCT in Dermatology
73.4.1 Publications
The availability of practical commercial products with CE and FDA clearance for clinical use is rapidly driving up the publication of research papers in dermatology. Figure 73.3 shows the number of papers referencing “optical coherence tomography” and “skin” indexed by PubMed [18] in a search on 30th December 2013 and categorized by the authors based on choice of publication journal, paper title, and abstract. Papers were categorized as follows:
1.
“Technology” papers – the primary subject of the paper is OCT technology itself: engineering, theory, and analysis of the OCT images. These papers are mostly published in technical journals. Only papers that specifically reference skin as the target end user application have been included in the analysis, and papers that merely used skin as a convenient test subject for a new OCT development were excluded.
2.
General/nonclinical dermatology papers – the primary subject of the paper is the research into skin and skin properties using OCT as a tool. This includes papers studying the structure and properties of normal skin and also nonclinical applications such as cosmetics research and research into drug delivery.
3.
Clinical dermatology papers – the primary subject of the paper is research into skin pathology and/or the application of OCT to diagnosis, mapping, or monitoring of treatments of skin pathologies. These papers are all published in clinical journals.
Fig. 73.3
OCT publications in dermatology by year of publication and type
73.4.2 Analysis
In total, 247 papers were indexed since 1997, and the number is continuing to grow at an encouraging rate. This is a larger number than in most other clinical specialties except ophthalmology and cardiovascular (see also Chap. 84, “OCT Technology Transfer and the OCT Market” by Eric Swanson in this book) and is an indication that OCT is gaining acceptance as a practical and useful imaging modality by dermatologists.
The first papers, published in 1997 and 1998 by Welzel and coworkers, describe the appearance of healthy skin in OCT and show some exemplary images of diseased skin [1, 2]. This was followed by papers in 2000 [19] in which Knuttel and coworkers described the use of OCT to measure skin parameters such as the thickness of the stratum corneum and scattering coefficient of tissue layers. In 2001 enough data had been collected to enable J. Welzel to publish a review paper mentioning potential clinical applications including diagnosis of skin diseases and monitoring of treatment effects [20].
Publications increased gradually in the following years but have increased more sharply since 2010 as dermatologists started applying OCT in more systematic fashion to both clinical and nonclinical applications. These are discussed in more detail below.
73.4.3 Tissue Engineering
Tissue engineering is concerned with the development of artificially grown sections of tissue for use in the repair of damaged human tissue, for example, bone cartilage. In dermatology, one of the main potential applications is repair of wounds, especially diabetic ulcers, which are a huge burden on the world’s health resources. OCT has potential use both for noninvasively monitoring the growth of the artificial tissue in the biofactories [21–23] and also, potentially, for monitoring the implanted tissue to assess its viability.
73.4.4 Transdermal Drug Delivery
Pharmaceutical companies are very interested in drug delivery mechanisms as alternatives to hypodermic syringes, for example, patches equipped with hollow microneedles filled with a drug. The biomechanical interaction of the microneedles with skin tissue is critical to the correct operation of these devices and is an area where OCT can potentially help, by direct real-time imaging needle implantation process. For example, Donnelly and coworkers at University of Belfast have imaged soluble microneedles [24, 25].
73.4.5 Hair and Alopecia
OCT may have application on studying hair abnormalities and causes of alopecia. Bartels and coworkers showed that OCT can be used to noninvasively measure hair shafts on normal and hair affected by alopecia areata with discrimination [26]. Lademann and coworkers also studied the same technique as a method of screening for doping substances [27]. It is possible to image hair follicles, and OCT may prove to be of interest to companies studying hair shaving and hair removal products.
73.4.6 Tattoos
Tattoos are commonly treated with high-power laser pulses. There is potential for OCT to be used to image the tattooed skin pretreatment, in order to assess the depth of the pigment, so that the laser can be adjusted for maximum effect. This has been studied and considered feasible by Morsy and coworkers [28].
73.4.7 Planning and Monitoring Treatment of Vascular Complaints
Skin vascular conditions such as port-wine stains and rosacea are, like tattoos, commonly treated with pulsed laser. There is interest in using OCT to image the blood vessels pretreatment in order to determine their diameter and depth and then to image posttreatment to validate the effects of the laser therapy [29, 30]. As noted above, it is unlikely that these applications will develop into routine clinical procedures before blood-flow imaging based on Doppler or speckle variance OCT is developed in a commercially available product.
73.4.8 Cosmetic Treatments, Skin Ageing and Wrinkles
OCT has attracted some interest from companies developing cosmetic treatments for “rejuvenating” or temporarily ameliorating the apparent effects of skin ageing. 3D OCT can be used to obtain topographic maps of the skin surface with resolution of 10 μm or better. This is higher than is easily available from commercially available alternatives; however, these are much cheaper to buy and also have much larger field of view than is typically available from an OCT instrument. Of more interest is measurement of epidermal thickness. The epidermis swells when hydrated, reducing wrinkle depth. OCT can be used to accurately measure epidermal thickness over time, thereby offering the researcher a means of quantitatively evaluating both the magnitude of the effect of a cosmetic treatment and how long it lasts.
73.4.9 Actinic Keratosis and Nonmelanoma Skin Cancer
OCT imaging of nonmelanoma skin cancer (NMSC) like squamous-cell carcinoma (SCC) with its precursors actinic keratosis (AK) and Bowen’s disease as well as the most common type of NMSC, basal cell carcinoma (BCC), has been intensively studied. NMSC is a very common disease, mainly affecting elderly patients with pale skin complexion and a history of sun exposure. The lifetime risk for NMSC in this group of persons is about 30 %. The diagnosis by the naked eye is not always easy, because there are no marked changes in skin color or appearance. The skin shows in many cases of NMSC only a slight keratosis and induration. Using dermoscopy, more specific signs like “arboreal” vessels in BCC may lead to a correct diagnosis, but for confirmation or distinguishing from inflammatory skin reactions, it is frequently necessary to take a biopsy. Because sun damage is the main risk factor, the lesions start as solitary plaques but evolving within years into a so-called field cancerization where the whole epidermis within a region like the bald head exhibits malignant cells.
There are several alternatives to surgical treatment of NMSC. In AK, topical treatments for single lesions like laser therapy, cryotherapy, and curettage as well as application of diclofenac gel, imiquimod as an immune modulating agent, or photodynamic therapy for field cancerization are efficient. SCC and BCC can be treated as well with imiquimod or photodynamic therapy, but these noninvasive treatments are restricted to superficial lesions because of the limited penetration depth of the drugs. To choose the most suitable therapeutic regime and for control of clearance, it is imperative to determine the diagnosis, the tumor thickness, and the lateral borders of the lesion.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


