14
Normal Glottic Configuration
Glottal configuration and glottal closure are terms often used interchangeably in the literature to describe the spatial characteristics of the vocal folds during phonation when viewed stroboscopically. Glottal configuration is defined as the shape of the glottal aperture during phonation. In describing glottal configuration, one is actually referring to the shape of the glottis. Whereas the term glottis is frequently used when referring to the vocal folds, the true definition of the term glottis is the space between the vocal folds (Fig. 14.1).
Glottal closure refers to the extent of vocal fold closure during the closed phase of phonation. Glottal closure is generally described as complete, incomplete, or inconsistent. The duration of glottal closure, relative to the rest of a single vibratory cycle, normally changes with the mode of vibration. Hirano described three typical vocal fold vibratory modes: falsetto, modal, and fry.1 In falsetto, there is incomplete glottal closure of the vocal folds throughout the cycle (Video Clip 4). During modal phonation, the vocal folds close completely during the closed phase of the vibratory cycle (Video Clip 1). In vocal fry, there is an extended duration of vocal fold closure relative to the rest of the vibratory cycle. The duration of vocal fold opening divided by the duration of the entire glottal cycle is called the open quotient and describes the percentage of time during a single vibratory cycle that the folds are in the open phase. (One minus the open quotient = the percentage of time during a single vibratory cycle that the folds are in the closed phase.) Vocal folds that never completely close, such as during falsetto, have an open quotient of 1. Modal phonation has an open quotient of 0.5. Glottal fry has an open quotient trending toward 0.2
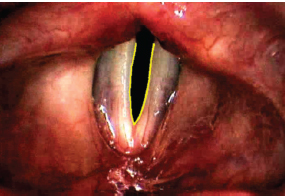
Fig. 14.1 The glottis.
Stroboscopic evaluation of the vocal folds is a frequently used method to assess glottal configuration and closure during phonation. While stroboscopy is the most clinically friendly, cost-effective method of viewing glottal configuration and closure during phonation, several factors must be taken into consideration during the examination. Gender and age have an impact on glottal configuration during phonation. Changes in pitch, loudness, vocal register, phonemic variations, and prosodic emphasis also have an effect on glottal configuration. Technical issues associated with the stroboscopic examination can further play a role in determining glottal configuration and glottal closure.
This chapter will describe (1) normal glottal configuration and the research to date on normal variations in glottal configuration, (2) methods to measure glottal configuration, (3) phonatory behaviors that influence the examination, and (4) technical pitfalls during stroboscopy that can affect an accurate assess ment of glottal configuration.
 Normal Glottal Configuration
Normal Glottal Configuration
Casper et al. wrote the following:
We sometimes think about the normal larynx as if that idealized state of perfection actually exists although we know that the term “normal” does not describe a single condition with set boundaries. Indeed given the opportunity to create the perfectly normal larynx, we probably could not agree on the elements of its design.3
It is generally assumed that normal glottal configuration is marked by complete glottal closure during the closed phase of phonation.4 However, in studies of “normal” larynges, the pivotal finding of most is the variety of glottal configurations identified.5–8 Casper et al. caution that in the absence of vocal fold pathologies, the difference between a normal larynx and one that is thought to be the cause of a voice disorder is indeed difficult to assess with use of stroboscopy alone.3
There is a need for a standardized nomenclature to describe glottal configuration. Figure 14.2 demonstrates several glottal configurations often referred to in the literature. It is important to recognize that the assessment of glottal configuration remains perceptual at best and, as such, is subject to interrater differences and confusion, due to the use of multiple terms and multiple descriptive rating systems. The seven most common glottal configurations plus complete glottal closure are listed here:
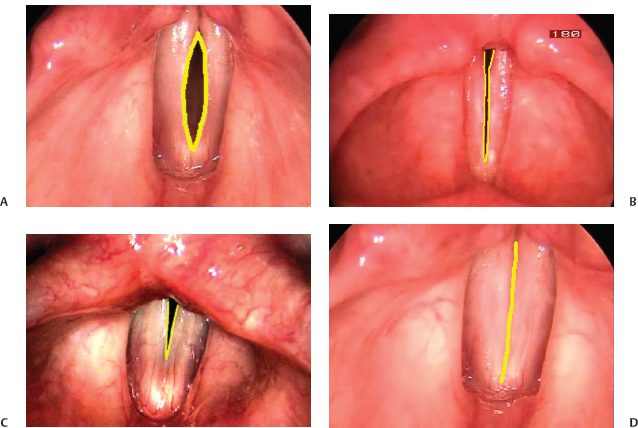
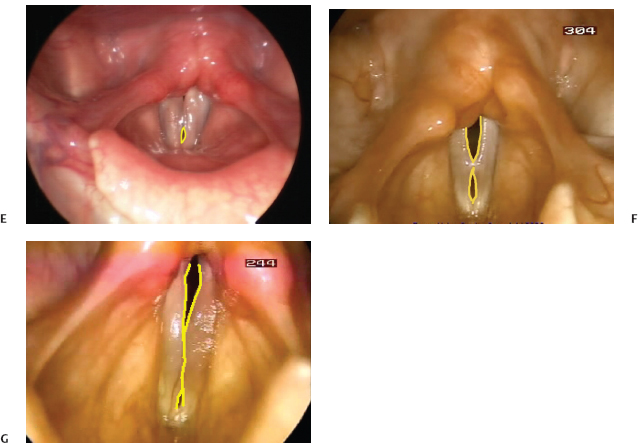
Fig. 14.2 Common glottal configurations: spindle (A), incomplete (B), posterior glottal chink (C), complete (D), anterior glottal gap (E), hourglass (F), irregular (G).
 Complete closure (Video Clip 1)
Complete closure (Video Clip 1)
 Posterior glottal chink (triangular opening from the cartilaginous glottis to the vocal processes that may extend anteriorly into the membranous glottis) (Video Clip 15)
Posterior glottal chink (triangular opening from the cartilaginous glottis to the vocal processes that may extend anteriorly into the membranous glottis) (Video Clip 15)
 Spindle shape (anterior commissure and vocal process closure only) (Video Clips 16 and 17)
Spindle shape (anterior commissure and vocal process closure only) (Video Clips 16 and 17)
 Hourglass configuration (mid-membranous closure only) (Video Clip 18)
Hourglass configuration (mid-membranous closure only) (Video Clip 18)
 Irregular closure (Video Clip 19)
Irregular closure (Video Clip 19)
 Incomplete closure (Video Clip 20)
Incomplete closure (Video Clip 20)
 Anterior glottal chink (Video Clips 3 and 21)
Anterior glottal chink (Video Clips 3 and 21)
Several authors have described glottal configurations seen during stroboscopy, though there is no consensus on nomenclature to describe the glottis, and no universally accepted glottal configuration scale exists to date.9–12 Hirano proposed a rating system that included a description of glottal configuration and glottal closure.1 He recommended that the examiner determine if the glottis is ever completely closed during phonation and, if so, evaluate how long it is closed. His descriptive scale for glottal closure is a rating of the duration of glottal closure as follows: a, very long; b, long; c, fairly long; d, short; or e, very short.
He also recommended that the examiner draw the shape of the glottis during maximum closure.
Bless et al. used seven line drawings of glottal configuration during phonation to develop a clinical evaluation tool to be used to rate the stroboscopic studies.10 The drawings represented frequently encountered glottal configurations and included complete closure; posterior glottal chink; anterior chink; spindle shape; incomplete closure; hourglass closure; and irregular closure patterns. Gelfer and Bultemeyer attempted to test the reliability of this system but included a measure of degree of glottal closure that was based on a three-point rating scale with 1 indicating complete closure and 3 indicating that the vocal folds never closed. They found that intrarater reliability was experience-dependent and perhaps related to the examiner’s visual-spatial skills. Their study also attempted to provide data on vocal fold vibratory patterns in normal adult females. Notably, they found that glottal configuration and glottal closure demonstrated the most intersubject variability of the stroboscopic parameters tested.6
Another system used in the literature to rate glottal configuration and glottal closure is found in studies by Södersten and Lindestad and Södersten et al. using a rating scale for judging vocal fold closure during phonation with line drawings of glottal configuration and scalar points for degree of closing. The six-point scale is as follows:
- Complete closure the full length of the vocal folds.
- Incomplete closure of the cartilaginous portion of the folds.
- Triangular incomplete closure extending into the membranous fold past the vocal processes.
- Triangular incomplete closure extending to include the posterior third of the vocal folds.
- Incomplete closure of the posterior two thirds of the vocal folds.
- Incomplete closure the full length of the folds.
There are an additional four descriptions including spindle-shaped closure with closure only at the vocal processes, spindle-shaped closure of the posterior third of the vocal folds with closure at the vocal process, spindle-shaped closure at the anterior third of the vocal folds, and spindle-shaped closure of the anterior third and the posterior third of the vocal folds with mid-membranous closure present.7,12,13
It is important when describing glottal configuration that the assessment of the shape of the glottis is made during the closed phase of the cycle. Glottal configuration changes as the phase of the glottal cycle changes.9 Figure 14.3 demonstrates the changes in glottal configuration and closure as the vocal folds move through the phases of modal phonation.
In the American Speech-Language-Hearing Association (ASHA) consensus document “Knowledge and Skills for Speech Language Pathologists with Respect to Vocal Tract Visualization and Imaging,” the working group suggested vocal fold closure during stroboscopy be rated as complete (open quotient normal, open quotient increased, open quotient decreased) or incomplete (posterior glottal gap, anterior glottal gap, elliptical, hourglass slit, or incomplete).14
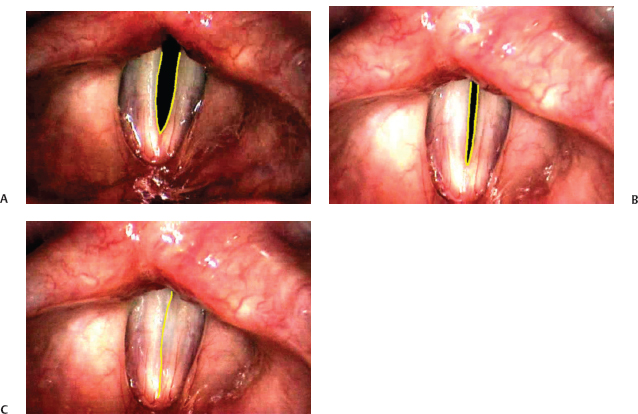
Fig. 14.3 Glottal configuration during glottal cycle in modal phonation: open phase (A), closing phase (B), closed phase (C).
A method to quantitatively measure glottal configuration was described by Secarz et al.15 Frames from the stroboscopic examination that represent the most open glottal width and those representing the most closed glottal width are first identified. A reference mark is made somewhere near the middle of the glottis, and measurements in pixels are made between the reference mark and the glottal edge. Woo used a method of drawing the glottal edge and measuring the glottal area.16 A similar procedure using a laser beam to identify a reference point on the vocal folds to assist with standardizing scope distance from the vocal folds and then using a method to measure glottal width was described by Patel (R. Patel, personal communication, 2008).
 Demographic Factors That Affect Glottal Configuration
Demographic Factors That Affect Glottal Configuration
Gender
Multiple studies in the late 1980s and early 1990s examined the gender differences in glottal configuration during stroboscopy. There was a consensus that there is a difference in the incidence of various glottal configurations between the genders.5,6,12,17 Men demonstrate complete glottal closure more often than women. Women demonstrate a greater incidence of posterior glottal chink, whereas, if present in men, the chink tends to be located toward the mid-membranous or anterior portions of the vocal folds.
Age
Age has an impact on glottal configuration. Biever and Bless found a high incidence of glottal gap in elderly women aged 60 to 77 years, and Linville found a high incidence of glottal gap in elderly women aged 72 to 87 years in a second study.5,18 The shape of the gap varied from a posterior glottal gap to a mid-membranous gap to an anterior glottal gap. In both studies, young women in their twenties were also found to have a higher incidence of posterior glottal gap. Most studies agree that normal age-related changes to the vocal folds are marked by atrophy and a resulting mid-membranous glottal gap. Varying degrees of spindle-shaped gaps are generally described in the aging larynx with a bowed appearance to the vocal folds themselves.
 Psychoacoustic Effects on Glottal Configuration
Psychoacoustic Effects on Glottal Configuration
Pitch, mode of phonation, loudness, and register will impact glottal configuration. One must consider muscle activation used to produce differences in phonation. Bonilha and Deliyski noted that glottal width irregularities should be expected when examining the vocal folds in any mode other than modal/habitual phonation even in normal, nondysphonic speakers.2 As an example, when the pitch is raised, the cricothyroid muscle is activated and pulls the thyroid and cricoid cartilage together thus lengthening and tensing the vocal folds. Clinicians generally believe that the result of this cricothyroid muscle activity is to prevent complete adduction during phonation thereby producing a complete mid-line glottal gap during phonation. However, Gelfer and Butlemeyer found glottal configuration was idiosyncratic within subjects at different pitches. They noted complete, incomplete, hourglass, and spindle configuration at high pitch, whereas low pitch was marked by complete, incomplete, and posterior glottal gap configurations.6
Loud phonation is produced by increasing subglottal pressure and glottal closure. It should not be a surprise that glottal closure is increased and glottal configuration tends toward more closed as loudness increases in normal speakers.
Register of phonation, or vibratory mode, has been found to impact glottal closure but not glottal shape.4 This phenomenon has been studied in modal and falsetto phonation. Though it is generally accepted that glottal closure is complete in modal register, incomplete in falsetto register, and extended in vocal fry, glottal configuration during both falsetto and modal varies between speakers.4 Once again, glottal configuration appears to be idiosyncratic.
 Technical Considerations in the Measurement of Glottal Configuration
Technical Considerations in the Measurement of Glottal Configuration
The technology of videostroboscopy limits the assessment of degree of glottal closure. Hapner and Johns write that stroboscopy provides only a two-dimensional view of the vocal folds viewed from above, the bird’s-eye view.19 This limits the ability to perceive three-dimensional contours of normal and pathologic tissue.
The type of scope used in laryngeal videostroboscopy can influence glottal configuration.20 Södersten and Lindestad found that use of a rigid laryngoscope increased the detection of incomplete glottal closure over what was found when using flexible laryngoscopy.12 This study and other studies used a 90-degree rigid laryngoscope, whereas other studies have used a 70-degree rigid laryngoscope.17 Different oral, laryngeal, and upper chest postures are used when examining with a 70-degree versus a 90-degree rigid laryngoscope, and the effects on glottal configuration have yet to be established. Therefore, care must be used when applying the results of the studies to clinical practice unless using the same method of examination.
Videostroboscopy has been found to be useful in determining the outcome of medical, surgical, or therapeutic intervention to correct glottic defects. Serial examinations are used to establish outcomes. The problem is that technical issues associated with stroboscopy make it difficult to compare accurately one examination with a repeat examination. Hibi et al.21 and Peppard and Bless11 proposed a method to increase the reliability of serial examinations by drawing on transparencies overlaid on the video monitor while the monitor displays a chosen image of the vocal folds and using the drawing in a follow-up examination for positioning of the folds on the monitor during the examination.
 Conclusion
Conclusion
Though videostroboscopy remains the most useful clinical tool to examine glottal configuration and glottal closure, care must be taken to avoid common technical pitfalls that impact the results of the examination. Bonilha and Deliyski warn that the extent of irregularity considered to be within normal limits should be determined for each evaluation tool used to assess glottal configuration as it may differ between evaluation tools.2 It is also important to be cognizant of the age and gender of the patient; the pitch, loudness, register, and mode of phonation during the examination; to establish a protocol of phonatory tasks to allow for better reliability in serial examination; and to understand the limitations of the stroboscopic examination.
Finally, Elias et al. studied stroboscopic variability in normal healthy singers.22 What was particularly interesting is that they found that 58% of the singers had abnormal videostroboscopy examinations, yet none of the singers reported any problems with vocal performance. In the discussion, the authors note that it is imperative for the examiner to remember that normal can occur in the presence of abnormal findings and that care should be taken before implying causality.
No definitive database of normal, nondysphonic vocal fold behavior has been developed, and most of the research into glottal configuration is at a minimum 10 years old. It behooves the examiner to be educated on normal variability in glottal configuration and glottal closure to prevent overdiagnosing abnormal behavior and referring for intervention.
References
1. Hirano M. Clinical Examination of Voice. New York, NY: Springer-Verlag; 1981
2. Bonilha HS, Deliyski DD. Period and glottal width irregularities in vocally normal speakers. J Voice 2008;22:699–708
3. Casper JK, Brewer DW, Colton RH. Variations in normal human laryngeal anatomy and physiology as viewed fiberscopically. J Voice 1987;1:180–185
4. Murry T, Xu JJ, Woodson GE. Glottal configuration associated with fundamental frequency and vocal register. J Voice 1998;12:44–49
5. Biever D, Bless DM. Vibratory characteristics of the vocal folds in young adult and geriatric women. J Voice 1989;3:120–131
6. Gelfer M, Bultemeyer D. Evaluation of vocal fold vibratory patterns in normal voices. J Voice 1990;4:335–345
7. Södersten M, Hertegård S, Hammarberg B. Glottal closure, transglottal airflow, and voice quality in healthy middle-aged women. J Voice 1995; 9: 182–197
8. Kendall KA. High-speed laryngeal imaging compared with videostroboscopy in healthy subjects. Arch Otolaryngol Head Neck Surg 2009;135:274–281
9. Karnell M. Synchronized videostroboscopy and electroglottography. J Voice 1989;3:68–75
10. Bless DM, Hirano M, Feder RJ. Videostroboscopic evaluation of the larynx. Ear Nose Throat J 1987;66:289–296
11. Peppard RC, Bless DM. A method for improving measurement reliability in laryngeal videostroboscopy. J Voice 1990;4:280–285
12. Södersten M, Lindestad PA. Glottal closure and perceived breathiness during phonation in normally speaking subjects. J Speech Hear Res 1990;33:601–611
13. Södersten M, Lindestad PA. A comparison of vocal fold closure in rigid telescopic and flexible fiberoptic laryngostroboscopy. Acta Otolaryngol 1992;112:144–150
14. American Speech-Language-Hearing Association. Knowledge and skills for speech language pathologists with respect to vocal tract visualization and imaging. ASHA Suppl 2004;24:184–192
15. Secarz JA, Berke GS, Arnstein DA, Gerratt B, Navidad M. A new technique for quantitative measures of laryngeal videostroboscopic images. Acta Otolaryngol 1991;117:871–875
16. Woo P. Quantification of videostrobolaryngoscopic findings: measurements of the normal glottal cycle. Laryngoscope 1996;106(3 Pt 2, Suppl 79)1–27
17. Sulter AM, Schutte HK, Miller DG. Standardized laryngeal videostroboscopic rating: differences between untrained and trained male and female subjects, and effects of varying sound intensity, fundamental frequency, and age. J Voice 1996;10:175–189
18. Linville SE. Glottal gap configuration in two age groups of women. J Voice 1992;35:1209–1215
19. Hapner ER, Johns MM. Recognizing and understanding the limitations of laryngeal videostroboscopy. Perspect Voice 2007;17:3–7
20. Pemberton C, Russell A, Priestley J, Havas T, Hooper J, Clark P. Characteristics of normal larynges under flexible fiberscopic and stroboscopic examination: an Australian perspective. J Voice 1993;7:382–389
21. Hibi S, Bless DM, Hirano M. Distortions of videostroboscopy images. J Voice 1988;2:168–175
22. Elias ME, Sataloff RT, Rosen DC, Heuer RJ, Spiegel JR. Normal strobovideolaryngoscopy: variability in healthy singers. J Voice 1997;11:104–107
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


