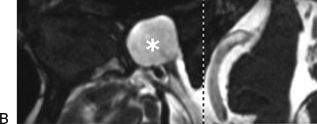
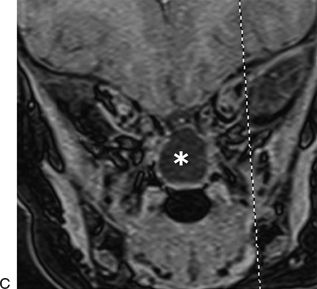
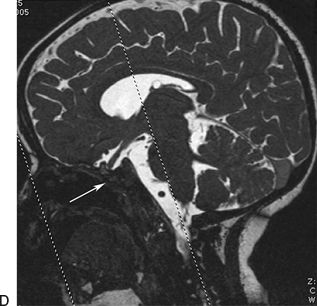
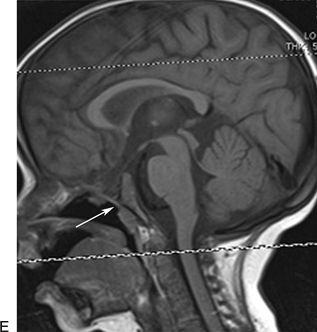
Figure 41.1 The multidisciplinary approach among otolaryngologist, neurosurgeon, maxillofacial surgeons, and reconstructive surgeons allows for proper management of complex cases. A 3-year-old patient with multiple malformations underwent a surgical reconstruction of the cleft lip and palate, combined with the endoscopic endonasal skull base reconstruction of a large meningoencephalocele (asterisk in the figures). A. Preoperative CT scan in sagittal view. B. Preoperative MR scan T2 weighted in sagittal view. C. Preoperative MR scan T1 weighted in coronal view. D. Postoperative MR scan in sagittal view in sequence T2 weighted, showing the skull base reconstruction (white arrow). E. T1 weighted, showing the skull base reconstruction (white arrow).
INDICATIONS
Every case of a dural defect with or without cerebrospinal fluid (CSF) leak must be repaired. Reconstructions strive to recreate a separation of the cranial cavity from the sinonasal cavity, to prevent CSF leak, pneumocephalus, and intracranial infection. Small defects in the skull base can be reconstructed using different types of free grafts with a high rate of success (>95%) (Castelnuovo, 2001). However, larger dural defects should be reconstructed by means of vascularized flaps. Among these, the nasoseptal flap is the preferred choice (Harvey, 2009; Patel, 2010). Personally, I consider every patient a candidate for a nonvascularized reconstruction, unless bone edges are not present. The absence of these bone edges prevents the proper positioning of the inlay grafts, the first intracranial intradural, and the second intracranial extradural (in a sort of “epidural pocket”), and so the risk of postoperative leakage is significantly increased. In this respect, most of the defects of the anterior cranial fossa are amenable to this reconstruction, while for defects of the middle and posterior cranial fossa, the percentage decreases significantly. Anatomically speaking, when dealing with the anterior cranial fossa, the surgeon can extend the intracranial supraorbital dissection without any risks. The same consideration is not appropriate for the middle and posterior cranial fossa. In these cases, the presence of the optic chiasm/pituitary stalk and the abducens nerve makes intracranial dissection very dangerous and not advisable.
CONTRAINDICATIONS
Given the necessity to have bone edges to support the inlay graft (second layer), their absence represents the most important contraindication to a standard multilayer technique with nonvascularized grafts. With regard to the anterior cranial fossa, almost every case can be managed with the nonvascularized graft technique. In this respect, surgeons need to be aware that the roof of the orbit is still present, even in complex cases of congenital malformations or in difficult revision cases, so that it can be used to support the graft. The same considerations are not always true in the middle and posterior cranial fossa, where, after wide resection of bone and dura, really limited edges of bone and dura are present. In some of these cases, we perform a sort of “gasket seal” technique (Lenz, 2008) usually using some type of elastic material such as septal or conchal cartilage to fix the connective tissue inside the dural defect. Furthermore, I am personally convinced that most cases of high-flow CSF leaks can be well managed with this technique if the inlay graft or the gasket seal technique is well conducted. Nevertheless, in some selected cases, especially when dealing with posterior cranial fossa and complex pituitary CSF leaks, I prefer to adopt a hybrid technique in which the multilayer technique is associated with a vascularized flap.
PREOPERATIVE PLANNING
Most of the large dural defects are the result of a resection for sinonasal malignancy. In those cases, resection of the dura is tailored to the needs of the patient and so can be extended from orbit to orbit and from frontal sinuses to planum sphenoidale. Thus, in every case I approach, a large dural defect is anticipated and reconstruction is planned. In this respect, especially when intradural work is anticipated, preoperative imaging is critical in order to evaluate the intracranial relationship of the lesions, mostly with respect to blood vessels (Fig. 41.2). Particular sequences of MR, not limited to anterior cranial fossa but extended to evaluate the entire skull base, are of paramount interest in the detection of suspicious areas, especially in cases of malformations (Fig. 41.3).
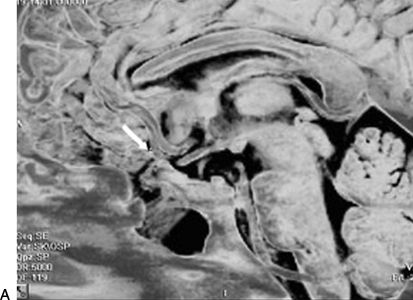
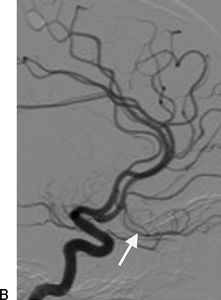
Figure 41.2 Preoperative imaging is critical in order to evaluate the intracranial relationship of the lesions, mostly with respect to blood vessels. A 19-year-old patient previously treated with transcranial surgical approach for posttraumatic pneumocephalus and CSF leak had a history of recurrent meningitis. Before the endoscopic endonasal surgical revision of the skull base reconstruction, an MR scan was performed (A) and angiography (B), which revealed the presence of the medial orbitofrontal artery (MOfA, arrow) inside the scar of the previous surgery, in the same region of the meningoencephalocele. This preoperative finding needs to be carefully evaluated during the surgical procedure, in order to avoid the risk of damaging vascular structures.
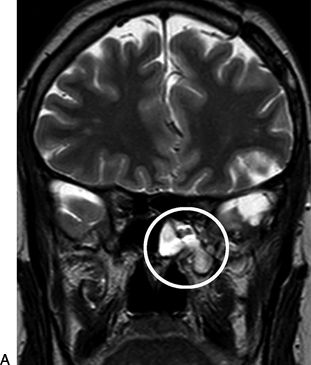
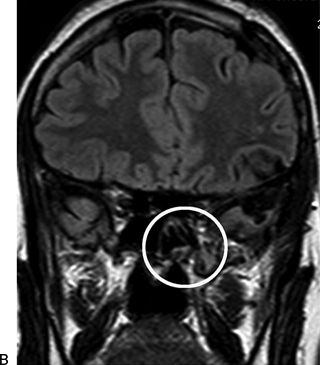
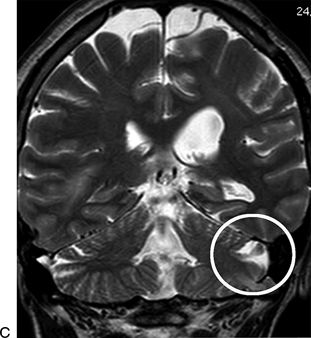
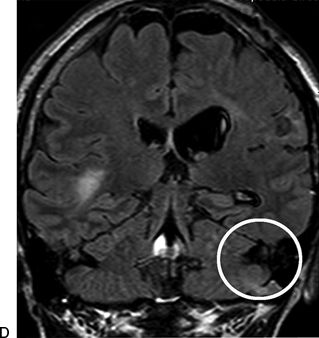
Figure 41.3 Radiologic preoperative evaluation study (CT scan and MR scan) of all the three cranial fossae and petrous bones leads us to a precise location of the defect, excluding the possibility of multiple sites of malformation. By comparing MR scan in T2-weighted sequence (A,C) with T2 FLAIR sequence (B,D), it is possible to appreciate a left sphenoid CSF leak (white circle in A and B) together with an additional site of CSF leak in the left mastoid region (white circle in C and D).
In these latter cases, CT scans demonstrate their utility allowing a precise and accurate evaluation of the bone structures of the sino–orbito–cranial interface. The preoperative understanding of the surgical field allows an accurate identification of the possible “supporting” structures for the reconstruction.
Of not minor importance is the identification, given our first choice for connective tissue of the patient, of previous surgery in the areas typically as donor sites. I personally prefer fascia lata and the iliotibial tract, so any kind of previous surgical procedures or trauma to the legs is evaluated. Possible connective tissue pathology is ruled out by means of history.
Materials: Some Considerations
My choice for autologous material is based on the scientific demonstration of good integration of the connective tissue, and on long-time otologic experience concerning repair of the tympanic membrane. Rarely, there is some extrusion of the heterologous material even some years after surgery, while no similar problems with autologous materials have emerged. As a technical hint, I advise the use of adipose tissue in small pieces for the reconstruction for two main reasons. The first is related to the role of dead space fillers, and the second one is due to the regenerative power of the adipose tissue cells.
I discourage the use of a bone graft for the reconstruction after resection of skull base malignancies, given the frequent need for postoperative radiotherapy, thus removing the risk of sequestration. Furthermore, I do not advise, in this case for oncologic reasons, the use of the nasoseptal flap for the reconstruction after resection of cancer because it may be involved in the disease process.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


