 Nonneoplastic Conditions That Can Simulate Posterior Uveal Melanoma and Other Intraocular Neoplasms
Nonneoplastic Conditions That Can Simulate Posterior Uveal Melanoma and Other Intraocular NeoplasmsNonneoplastic Conditions That Can Simulate Posterior Uveal Melanoma and Other Intraocular Neoplasms
Several conditions can clinically simulate posterior uveal melanoma (1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24). A list of the various pseudomelanomas is provided in a recent survey from the Oncology Service at Wills Eye Institute (5). Other tumors that can resemble melanoma are discussed in their respective chapters in this book. Almost every fundus tumor described in this book can, at one time or another, have features similar to those of choroidal or ciliary body melanoma. This section covers selected nonneoplasticsimulating conditions that are not discussed elsewhere in this book. The following is a brief outline of some of these pseudomelanomas that are seen in a practice of ocular oncology and are discussed and illustrated.
Vascular and hemorrhagic lesions
Age-related macular degeneration (ARMD; CEHCR)
Peripheral exudative hemorrhagic chorioretinopathy (PEHCR)
Hemorrhagic retinal macroaneurysm
Miscellaneous subretinal and intraretinal hemorrhage
Idiopathic choroidal neovascular membrane
Localized choroidal hemorrhage
Vortex vein varix
Inflammatory and infectious conditions
Nodular posterior scleritis
Uveal effusion
Granulomas (sarcoidosis, tuberculosis, solitary idiopathic choroiditis)
Solitary infectious lesions
Miscellaneous conditions
Bilateral diffuse uveal melanocytic proliferation
Sclerochoroidal calcification
Rhegmatogenous retinal detachment
Scleral buckle after retinal detachment surgery
Bullous degenerative retinoschisis
Ciliochoroidal detachment
Subluxed lens
Globe compression by orbital tumor
Staphyloma
Postsurgical uveal prolapse
Selected References
1. Shields JA, Shields CL. Differential diagnosis of posterior uveal melanoma. In: Shields JA, Shields CL, eds. Intraocular Tumors. A Text and Atlas. Philadelphia: WB Saunders; 1992:137-153.
2. Ferry AP. Lesions mistaken for malignant melanoma of the posterior uvea. Arch Ophthalmol 1964;72:463-469.
3. Shields JA, Zimmerman LE. Lesions simulating malignant melanomas of the posterior uvea. Arch Ophthalmol 1973;89:466-471.
4. Shields JA, Augsburger JJ, Brown GC, et al. The differential diagnosis of posterior uveal melanoma. Ophthalmology 1980;87:543-548.
5. Shields JA, Mashayekhi A, Ra S, et al. Pseudomelanomas of the posterior uveal tract. The 2006 Taylor Smith Lecture. Retina 2005;25:767-771.
6. Gass JDM, Gieser RG, Wilkinson CP, et al. Bilateral diffuse uveal melanocytic proliferation in patients with occult carcinoma. Arch Ophthalmol 1990;108:527-533.
7. Rohrbach JM, Roggendorf W, Thanos S, et al. Simultaneous bilateral diffuse melanocytic uveal hyperplasia. Am J Ophthalmol 1990;110:49-56.
8. Watson PG, Hayreh SS. Scleritis and episcleritis. Br J Ophthalmol 1976;60:163-191.
9. Benson WE, Shields JA, Tasman WS, et al. Posterior scleritis. Arch Ophthalmol 1979;97:1482-1486.
10. Demirci H, Shields CL, Honavar SG, et al. Long-term follow-up of giant nodular posterior scleritis simulating choroidal melanoma. Arch Ophthalmol 2000;118:1290-1292.
11. Arevalo JF, Shields CL, Shields JA. Giant nodular posterior scleritis simulating choroidal melanoma and birdshot retinochoroidopathy. Ophthalmic Surg Lasers Imaging 2003;34:403-405.
12. Gunduz K, Shields CL, Shields JA, et al. Presumed choroidal granuloma with vitreous hemorrhage resembling choroidal melanoma. Ophthalmic Surg Lasers 1998;29:422-425.
13. Shields JA, Shields CL, Demirci H, et al. Solitary idiopathic choroiditis. Richard B. Weaver Lecture. Arch Ophthalmol 2002;120:311-319.
14. Silva VB, Brockhurst RJ. Hemorrhagic detachment of the peripheral retinal pigment epithelium. Arch Ophthalmol 1976;94:1295-1313.
15. Morgan CM, Gragoudas ES. Limited choroidal hemorrhage mistaken for a choroidal melanoma. Ophthalmology 1987;94:41-46.
16. Gunduz K, Shields CL, Shields JA. Varix of vortex vein simulating choroidal melanoma. Report of four cases. Retina 1998;18:343-347.
17. Gass JD, Jallow S. Idiopathic serous detachment of the choroid, ciliary body, and retina (uveal effusion syndrome). Ophthalmology 1982;89:1018-1032.
18. Schepens CL, Brockhurst RJ. Uveal effusion. 1. Clinical picture. Arch Ophthalmol 1963;70:189-201.
19. Regillo C, Shields CL, Shields JA, et al. Ocular tuberculosis. JAMA 1991; 266:1490.
20. Demirci H, Shields CL, Shields JA, et al. Ocular tuberculosis masquerading as ocular tumors. Surv Ophthalmol 2004;49:78-89.
21. Phillips W, Shields CL, Shields JA, et al. Nocardia choroidal abscess. Br J Ophthalmol 1992;76:694-696.
22. Hiss PW, Shields JA, Augsburger JJ. Solitary retinovitreal abscess as the initial manifestation of cryptococcosis. Ophthalmology 1988; 96:162-165.
23. Shields JA, Shields CL. Sclerochoroidal calcification. Review. The 2001 Harold Gifford Lecture. Retina 2002;22:251-261.
24. Hong PH, Jampol LM, Dodwell DG, et al. Unifocal helioid choroiditis. Arch Ophthalmol 1997;115:1007-1013.
▪ Age-Related Macular Degeneration Simulating Choroidal Melanoma
Age-related macular degeneration is a very common cause of visual loss in older patients. It often produces hemorrhage that can sometimes simulate clinically a pigmented choroidal melanoma. The patients shown were all referred to the Oncology Service because of suspicion of choroidal melanoma. However, a comparable-sized melanoma would be unlikely to cause extensive hemorrhage. ARMD often shows exudation and fibrous tissue representing resolving blood and proliferation of the retinal pigment epithelium (RPE), findings that would also be unlikely for melanoma.
1. Shields JA, Augsburger JJ, Brown GC, et al. The differential diagnosis of posterior uveal melanoma. Ophthalmology 1980;87:543-548.
2. Shields JA, Mashayekhi A, Ra S, et al. Pseudomelanomas of the posterior uveal tract. The 2006 Taylor Smith Lecture. Retina 2005;25:767-771.
 Figure 11.1. Resolving hemorrhagic disciform lesion simulating melanoma as part of age-related macular degeneration in an 80-year-old man. Note the yellow fibrous tissue resulting from prior hemorrhage. |
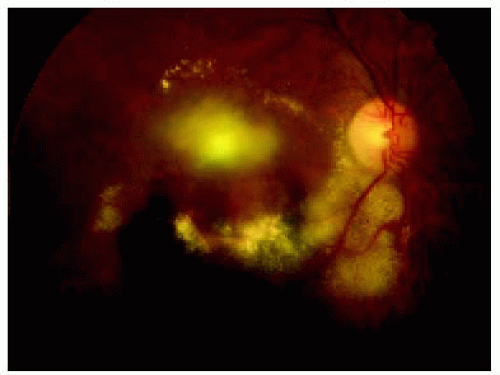 Figure 11.2. Age-related macular degeneration with exudation and hemorrhage in the foveal region and along the inferior arcade. |
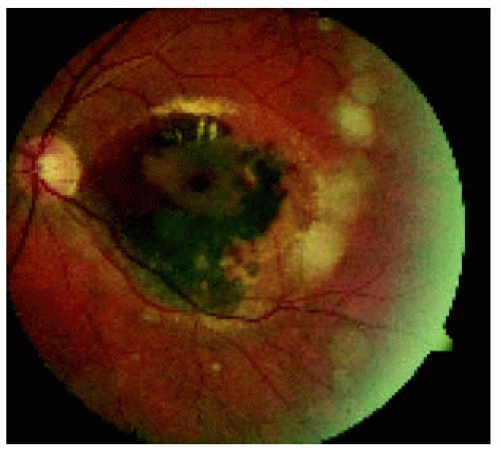 Figure 11.3. Resolving hemorrhagic age-related macular degeneration with secondary hyperplasia of the retinal pigment epithelium, centered in the macular region. Note the yellow intraretinal exudation at the superior margin of the lesion. |
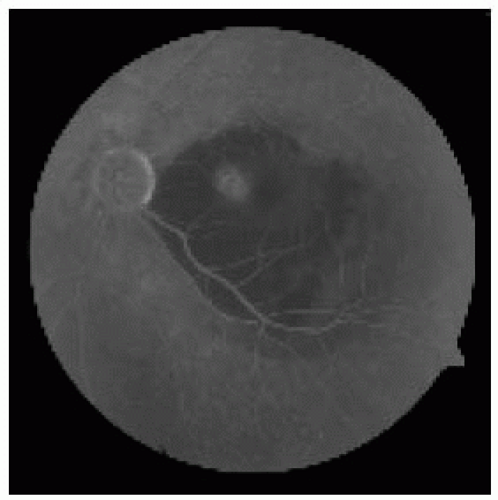 Figure 11.4. Fluorescein angiogram of the lesion in Figure 11.3 in the late recirculation phase, showing hypofluorescence of the lesion. The focus of hyperfluorescence in the papillomacular bundle region represents choroidal neovascularization that led to the hemorrhage. Indocyanine green angiography would demonstrate the choroidal neovascularization more clearly. |
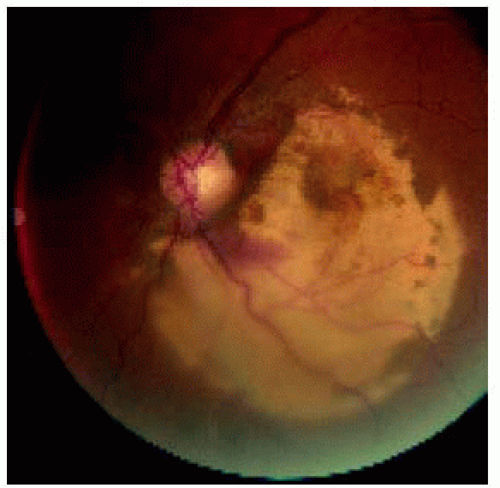 Figure 11.5. Age-related macular degeneration in which the blood had resolved, leaving the yellow-gray fibrous tissue that is typical of prior bleeding. This should not be mistaken for amelanotic melanoma. |
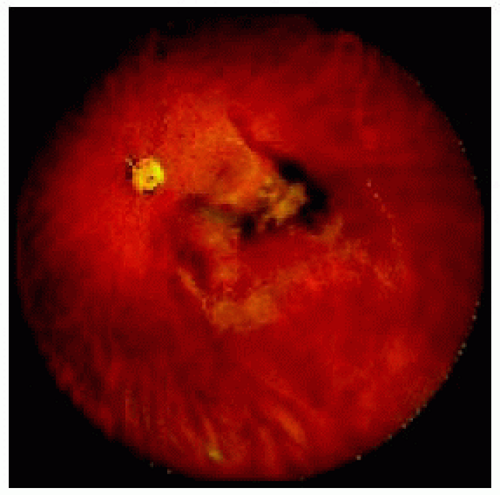 Figure 11.6. Wide-angle image of age-related macular degeneration showing fresh blood, resolved blood, and pigment epithelial detachment and hyperplasia, findings that would be unexpected with melanoma. |
▪ Peripheral Exudative Hemorrhagic Chorioretinopathy Simulating Choroidal Melanoma
Peripheral exudative hemorrhagic chorioretinopathy (PEHCR) is a term we use to define a peripheral condition that is similar clinically to ARMD in the central retina. It is also called peripheral disciform degeneration, eccentric disciform degeneration, or peripheral hemorrhagic detachment of the RPE. Like its central counterpart, it is common in older patients and can simulate a choroidal melanoma. In our most recent series of pseudomelanomas, PEHCR was second in frequency to choroidal nevus among simulating lesions. Wide-angle photographs of this lesion are shown.
1. Shields JA, Augsburger JJ, Brown GC, et al. The differential diagnosis of posterior uveal melanoma. Ophthalmology 1980;87:543-548.
2. Shields JA, Mashayekhi A, Ra S, et al. Pseudomelanomas of the posterior uveal tract. The 2006 Taylor Smith Lecture. Retina 2005;25:767-771.
3. Silva VB, Brockhurst RJ. Hemorrhagic detachment of the peripheral retinal pigment epithelium. Arch Ophthalmol 1976;94:1295-1313.
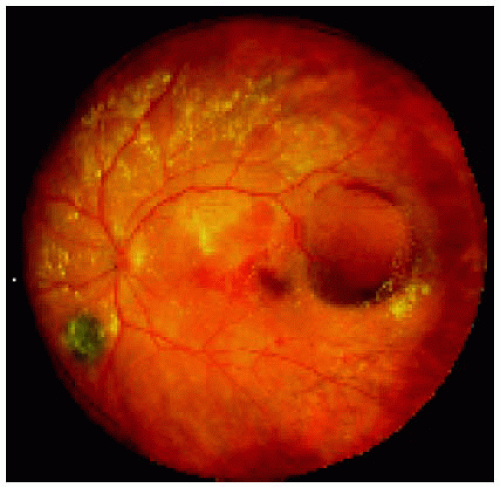 Figure 11.7. Peripheral exudative hemorrhagic chorioretinopathy characterized by a hemorrhagic detachment of the retinal pigment epithelium near the temporal equator in the left eye. |
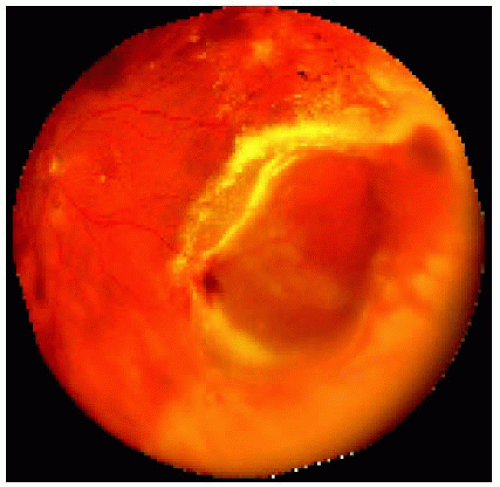 Figure 11.8. Peripheral exudative hemorrhagic chorioretinopathy near the temporal equator, showing superficial and deep retinal hemorrhage and yellow circinate exudation. |
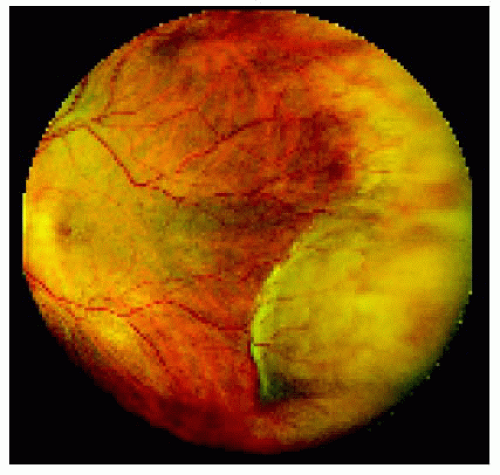 Figure 11.9. Peripheral exudative hemorrhagic chorioretinopathy located inferotemporally in the left eye, showing a localized area of large subretinal hemorrhage that has undergone resolution. |
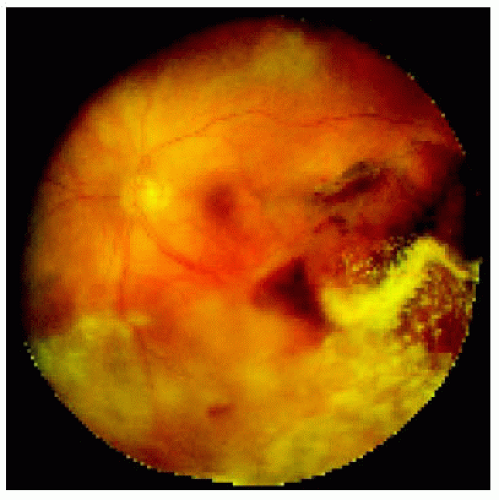 Figure 11.10. Peripheral exudative hemorrhagic chorioretinopathy located inferiorly and temporally in the left eye with more extensive hemorrhage, pigment proliferation, and widespread exudation and an elevated detachment of the retinal pigment epithelium temporal to the macular region. |
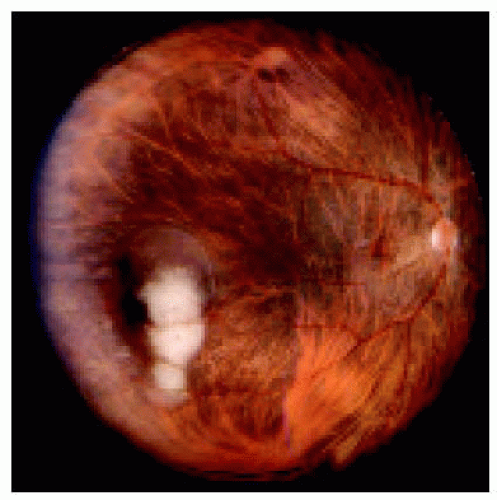 Figure 11.11. Peripheral exudative hemorrhagic chorioretinopathy in the inferotemporal quadrant of the right eye. In this case, the blood has entirely resolved, leaving an irregular white fibrous tissue scar. This appearance is unlike that of a nonpigmented choroidal melanoma. |
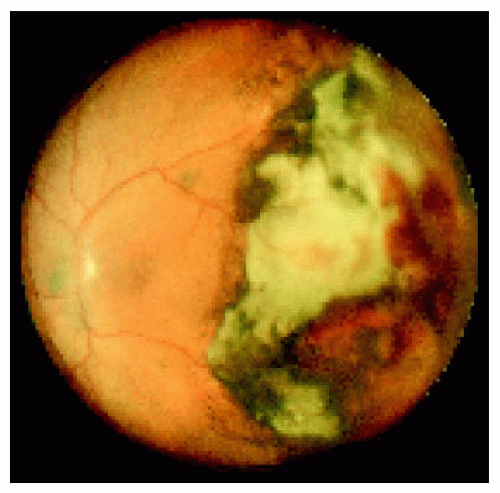 Figure 11.12. Widespread temporal fibrous tissue in the temporal portion of the left fundus, with secondary proliferation of the retinal pigment epithelium. |
▪ Peripheral Exudative Hemorrhagic Chorioretinopathy Simulating Choroidal Melanoma
Additional examples are shown of this important pseudomelanoma.
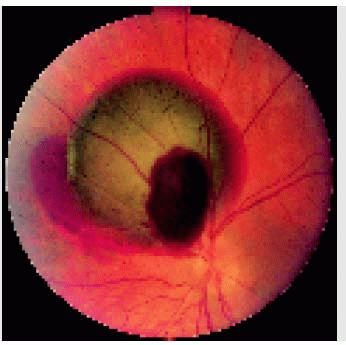
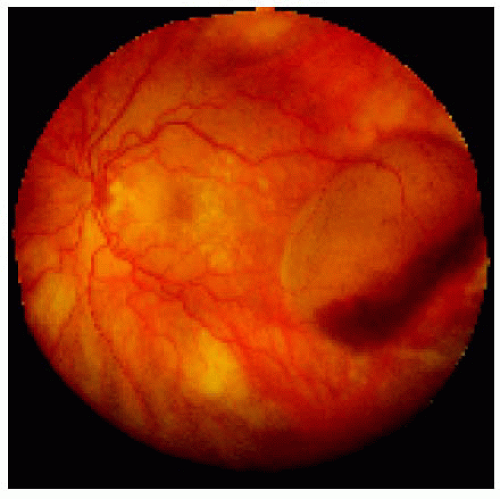 Figure 11.13. Large combined serous and hemorrhagic detachment of the retinal pigment epithelium in the temporal quadrant of the left fundus. Note that the serosanguineous fluid is more superior and the fresh blood is more inferior within the pigment epithelial detachment. |
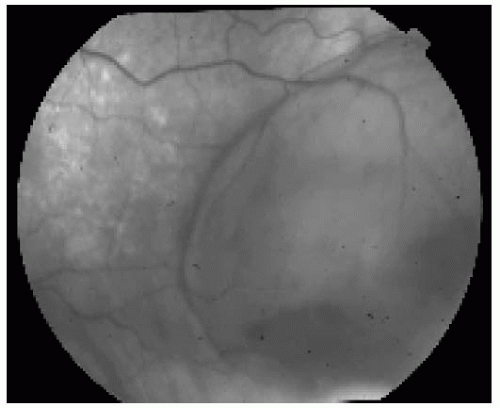 Figure 11.14. Closer view of lesion shown in Figure 11.13 with red-free photography. Note the similarity to a lightly pigmented melanoma. |
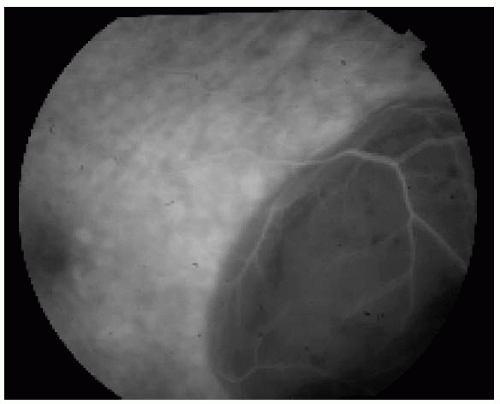 Figure 11.15. Fluorescein angiogram in the recirculation phase, showing hypofluorescence of the lesion. In contrast, a lightly pigmented melanoma would be hyperfluorescent. |
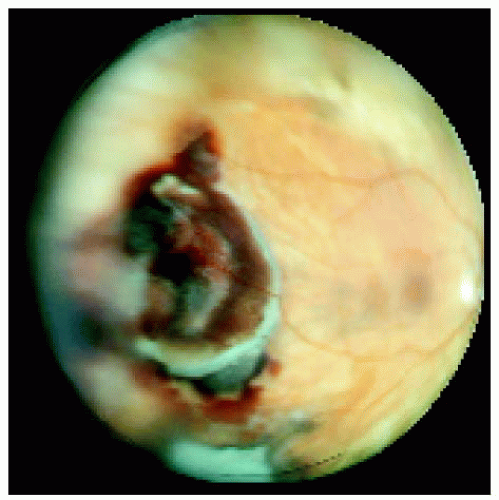 Figure 11.16. Massive peripheral exudative hemorrhagic chorioretinopathy located near the temporal equator of the right eye. |
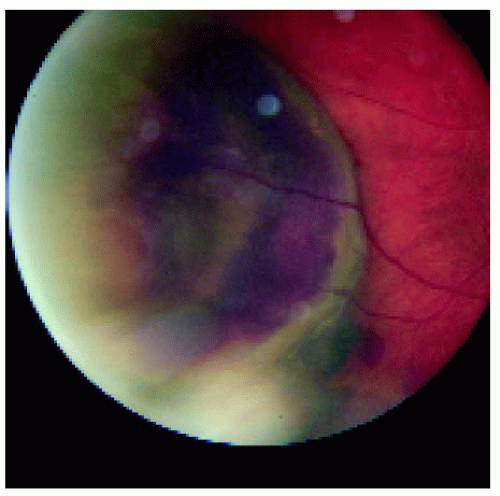 Figure 11.17. Closer view of the lesion shown in Figure 11.16. Note the remarkable similarity to a dome-shaped ciliochoroidal melanoma. |
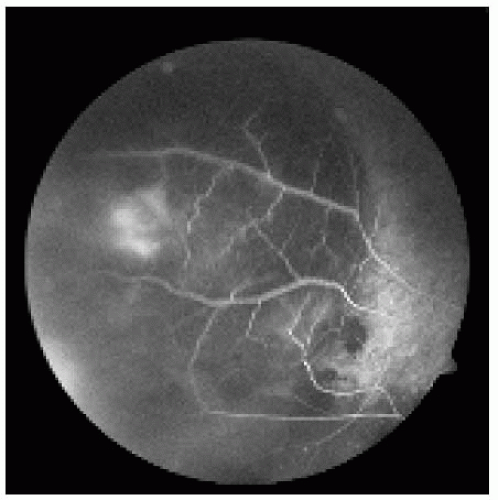 Figure 11.18. Fluorescein angiogram in the late venous phase of the lesion shown in Figure 11.17, demonstrating hypofluorescence of the lesion. The hyperfluorescent focus probably represents a partial view of the neovascular membrane that led to the hemorrhage. In contrast, a melanoma would show more extensive hyperfluorescence.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|