NEURAL LESIONS
Most lesions of the peripheral nervous system can occur in the upper aerodigestive tract (
Table 8.1).
1 These include neurofibromas, schwannomas, granular cell tumors, neuromas, neurothekeomas, paragangliomas, and malignant peripheral nerve sheath tumors (MPNSTs). Most may occur throughout the upper aerodigestive tract region; however, many occur more frequently at particular sites in well-defined clinicopathologic circumstances. With small biopsy specimens, it is not always possible to distinguish the lesions from one another, as knowing the low-power architecture is sometimes necessary for a definitive diagnosis. In such cases, differential diagnoses can be carried out or more general diagnoses, such as
benign nerve sheath tumor or
benign neural tumor, can be used.
Traumatic neuromas can occur throughout the tract but most frequently arise in the lip, tongue, or mental nerve area.
1,2 They present as small nodules that are often painful to palpation. Like their counterparts throughout the body, they are composed of tangles of neural tissue composed of axons and schwann cells, often accompanied by dense fibrotic
tissue (
Fig. 8.1, e-
Fig. 8.1). Ganglion cells have been reported in some lesions. An immunostain for S100 protein can be used to highlight the neural nature of these lesions.
Mucosal neuromas of multiple endocrine neoplasia type 2B resemble traumatic neuromas and are composed of convoluted neural tissue with numerous axons surrounded by a thickened perineurium.
1,3 These lesions mostly involve the lips and the tongue but can also involve other
oral and nasal sites. The syndrome is associated with familial mutations of the
RET proto-oncogene and the development of medullary thyroid carcinoma and pheochromocytomas.
3,4 It is important to distinguish these lesions from neurofibromas, as the lesions occur in vastly different syndromes and have different risks for subsequent diseases.
Solitary and multiple neurofibromas can also occur throughout the upper aerodigestive tract region and may be associated with neurofibromatosis type 1.
1,5,6 and
7 The distinction of these lesions from other neural tumors is thus important, as the diagnosis can allow for the identification of other stigmata of the disease. Neurofibromas appear either somewhat circumscribed or plexiform (
Fig. 8.2); however, even when they appear circumscribed, the interface of the lesion with the surrounding soft tissue is usually not discrete. Neurofibromas are composed of intermixed spindled cells, with serpentine or wavy nuclei, collagenous fibers, and myxoid matrix (e-
Fig. 8.2). A mixture of S100 protein and CD34 immunoreactive cells can be identified by immunohistochemistry. Neurofibromas can usually be distinguished from other neural tumors because of their classic, rather uniform histology.
Schwannomas or neurilemomas also occur throughout the upper aerodigestive tract.
1,5,8,9 Aside from those that involve the ear, they appear to be most frequent in the sinonasal area. These tumors occur in older adults and usually present as polypoid masses with symptoms secondary to mass effect. Although benign, schwannomas may be associated with the destruction of surrounding bony tissues.
8 When not resected in a piecemeal fashion, the lesions will sometimes appear circumscribed and encapsulated, although this feature seems to be less
common compared with peripheral schwannomas and infiltration into adjacent mucosal epithelium may be seen.
8 Histologically, the tumors are similar to those seen at other sites of the body and are composed of variably cellular areas (cellular Antoni A and looser, less cellular Antoni B areas) (
Fig. 8.3, e-
Fig. 8.3). Nuclear palisading or Verocay bodies can be identified in some cases and hyalinized blood vessels can be found in most examples (e-
Figs. 8.4 and
8.5).
8,9 The tumors show strong and diffuse immunoreactivity with antibodies to S100 protein. Although occasional cells may be immunoreactive with antibodies to CD34, such cells are much fewer in number than in neurofibromas.
8,9
Granular cell tumors occur throughout the body, but the tongue is the most commonly involved anatomic site.
10,11 These lesions usually present as painless submucosal nodules. Frequently, the overlying squamous epithelium will show a significant amount of pseudoepitheliomatous hyperplasia, a well-described pitfall that has led some cases to be erroneously diagnosed as squamous cell carcinomas.
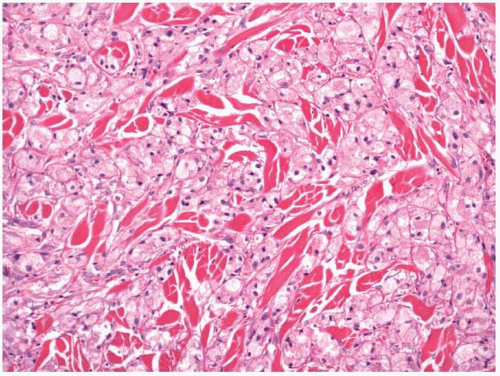
10,11 Granular cell tumors are circumscribed but not encapsulated, and neoplastic cells frequently infiltrate the surrounding soft tissues. The constituent cells are large and polygonal, with abundant granular, eosinophilic cytoplasm (
Fig. 8.4). Ultrastructurally, the granularity is due to the numerous lysosomes filling the cytoplasm.
10 Nuclei are small and centrally located and rare cells may be multinucleated. Mitotic figures are uncommon but occasional typical forms can be identified. Immunohistochemically, the neoplastic cells react strongly and diffusely with antibodies to S100 protein (e-
Fig. 8.6) and other markers of antigens associated with peripheral nerves.
12,13 Not surprisingly, the neoplastic cells react with antibodies to lysozyme and CD68.
14 Rare granular cell tumors are malignant and, as such, are characterized by a larger size, necrosis, increased mitotic activity, and cellular atypia. Distinguishing malignant tumors from multifocal granular cell tumors may be difficult.
It is unclear how
congenital epulis or
congenital granular cell tumor relates to the typical adult granular cell tumor. These tumors present as large polypoid masses attached to the gingiva of newborns, almost always in girls.
15 By conventional hematoxylin-eosin histology, they are identical to adult granular cell tumors (e-
Fig. 8.7). The neoplastic cells do not react with antibodies to S100 protein, however.
16Nerve sheath myxomas and
neurothekeomas are uncommon, benign tumors.
17,18 and
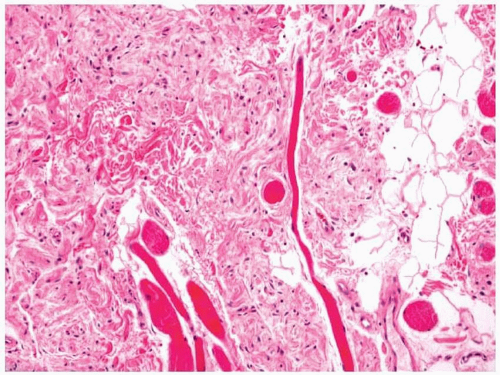
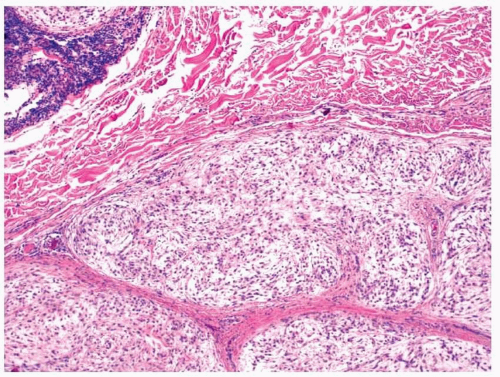
19 Both may involve the head and the neck and when reported in the upper aerodigestive tract, they have almost exclusively involved the mouth. Histologically, nerve sheath myxomas are lobular and well circumscribed, although they do not have a capsule (
Fig. 8.5).
1,18 The lobules are composed of abundant myxoid stroma with intermixed spindled cells and are separated from one another by fibrous connective tissue that resembles perineurium (e-
Fig. 8.8). These lesions show immunoreactivity with antibodies to S100 protein. Neurothekeomas are also typically well circumscribed and grow as lobules of neoplastic cells separated by bands of collagen. Frequently, some degree of myxoid matrix is present. The growth pattern is typically whirled, although some fascicular growth may be present. Tumor cells are spindled and epithelioid with abundant eosinophilic cytoplasm. Only minimal to mild
atypia is present in most cases and mitotic figures are usually infrequent. Osteoclastlike giant cells are sometimes present. Unlike nerve sheath myxomas, these lesions are not immunoreactive with antibodies to S100 protein. They are typically immunoreactive with antibodies to NKI/C3, vimentin, and neuron-specific enolase (NSE). Frequently, they are immunoreactive with antibodies to muscle-specific actin and smooth muscle actin. Recently, some have suggested that these tumors may be related to fibrous histiocytomas.
20
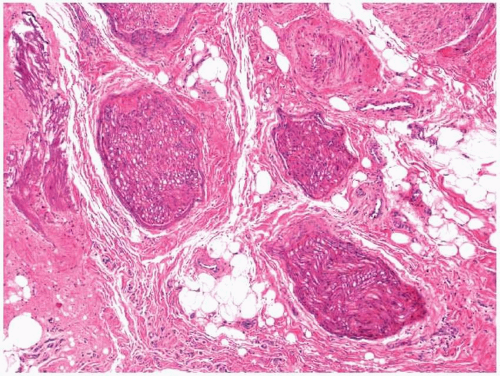
Palisaded encapsulated neuroma, or solitary circumscribed neuroma, is a benign tumor of the peripheral nerve sheath, which mostly occurs subcutaneously but may involve the mouth, especially in the region of the lips, gingiva, and palate.
21,22 and
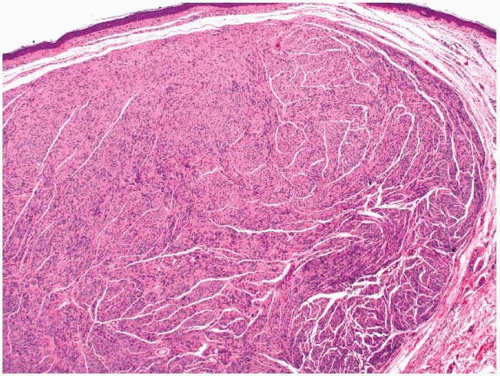
23 These lesions are described as slow growing and painless and are mostly identified in adults. Histologically, they are well circumscribed and partially encapsulated (
Fig. 8.6). Tumors are composed of broad fascicles of spindled cells with little intervening eosinophilic stroma. Although the nuclei can focally appear vaguely parallel, palisading nuclei (Verocay bodies) akin to those in schwannomas are not usually seen with this tumor, in spite of its name.
21,23 Furthermore, hypocellular areas are also not seen. Small vessels are often noted, and hemorrhage and necrosis are not seen. Most tumor cells react with antibodies to S100 protein. Immunostaining for epithelial membrane antigen (EMA) will highlight the perineurium that surrounds the lesions.
21,22
MPNSTs also occur throughout the upper aerodigestive tract region and have been frequently noted in the sinonasal area.
24,25 and
26 These tumors develop in older individuals and most often occur in patients who do not have neurofibromatosis. Unlike schwannomas, MPNSTs are infiltrative
and destructive and, after resection, tend to recur and eventually metastasize.
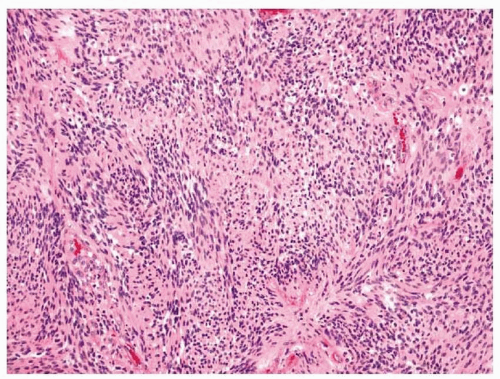
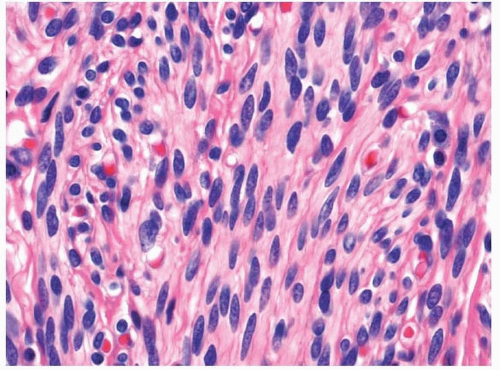
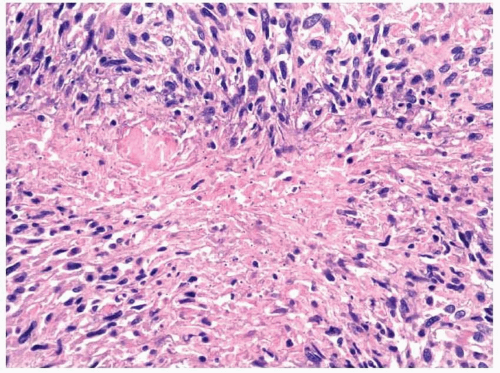
25,26 MPNSTs are usually highly cellular and generally have a histologic pattern reminiscent of a fibrosarcoma, although a prominent herringbone pattern is usually not seen and the nuclei tend to appear more irregular and wavy (
Fig. 8.7).
25,26 MPNSTs have also been noted to
have alternating less cellular (e-
Fig. 8.9) areas and rare nuclear palisading. Compared with benign neurogenic tumors, mitotic figures in MPNSTs are usually increased in number and geographic necrosis can sometimes be found (
Fig. 8.8). Immunohistochemistry can be helpful in the diagnosis, especially if the tumor is immunoreactive with antibodies to S100 protein.
25,26 Staining for CD56 is more sensitive but less specific (e-
Fig. 8.10). Importantly, with small biopsy specimens, positive staining with antibodies to S100 protein does not clinch a diagnosis of MPNST and malignant melanoma must be excluded.
25 Also of note, up to 15% of MPNSTs are immunoreactive with antibodies to TLE1, an antibody generally used to diagnose synovial sarcoma.
27Most
paragangliomas of the head and neck arise at the carotid body, the vagal body, or the middle ear. Those that arise in the upper aerodigestive tract usually involve the nasal cavity or larynx.
28,29 and
30 Occasional tumors, likely arising in the vagal body, will present as nasopharyngeal masses. Paragangliomas develop in both the sexes, usually in adults. Those that arise in the head and neck present almost exclusively with mass-related symptoms or other nonspecific symptoms related to their site of presentation (e.g., epistaxis when in the nasal cavity).
28,30 Head and neck paragangliomas almost never produce symptoms secondary to hormone production, especially catecholamine production. Some pheochromocytomas and extraadrenal paragangliomas are familial and can be seen with mutations of the
VHL gene, the
RET proto-oncogene, and the genes encoding for subunits of succinate dehydrogenase.
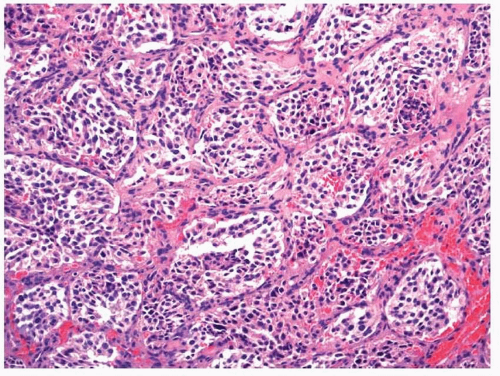
31Paragangliomas have histologic features akin to those of pheochromocytomas of the adrenal gland.
29,30 They tend to be well circumscribed and partially encapsulated. The tumors are composed of nests of epithelioid cells with finely granular, eosinophilic cytoplasm and round to oval nuclei (
Fig. 8.9, e-
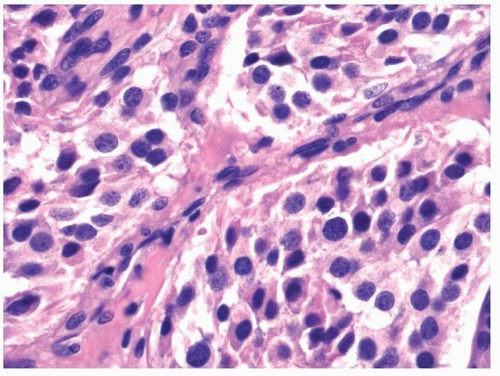
Fig. 8.11). The nuclei may have granular chromatin, and occasional prominent nucleoli may be seen (
Fig. 8.10). Atypia may
be present and should not be considered as a feature suggestive of malignancy. Mitotic figures are rare. Surrounding the nests are slender sustentacular cells and a rich network of capillaries. Immunohistochemically, neoplastic cells will react with antibodies to chromogranin, synaptophysin, and NSE.
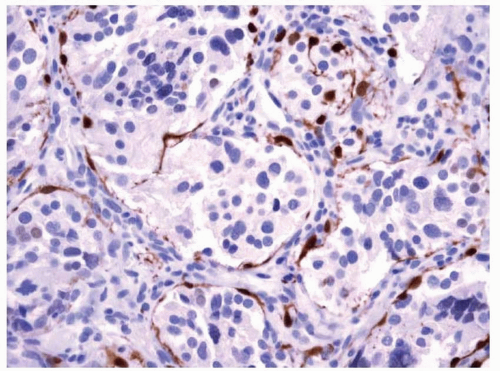
32,33 They do not react with antibodies to cytokeratins. Supporting sustentacular cells will react with antibodies to S100 protein (
Fig. 8.11). Although some tumors will behave in a malignant fashion, histology provides few clues to distinguish between benign and malignant tumors. Some have suggested that lack of sustentacular cells, identified by an absence of S100 protein staining, may help to identify malignant tumors.
34Olfactory neuroblastomas (ONBs) are rare tumors that develop in the upper nasal cavity in the area of the olfactory epithelium.
35,36 and
37 The tumors show a bimodal age incidence and occur most frequently in adolescents and older adults. They do not show a predilection for either sex or race. Patients with these malignancies present with nonspecific symptoms, including nasal stuffiness, epistaxis, nasal discharge, headache, and anosmia. Occasionally visual changes can be present.
The tumors are usually polypoid and occur high in the nasal cavity in the region of the cribriform plate, superior turbinate, and ethmoid sinuses.
35,37 The sharply defined location of the tumor and its phenotypic characteristics have led most to consider it to originate from olfactory epithelium. As biopsy specimens are received piecemeal and as patients are usually treated prior to surgical resection, staging is generally performed
clinically and radiographically, based on the extent of the tumor, according to the method originally described by Kadish (
Table 8.2).
37 Molecular changes are complex, similar to most epithelial malignancies.
38 ONB is not a member of the Ewing sarcoma group of tumors and the typical t(11;22) seen in those tumors is not seen with ONBs, despite an earlier study claiming the contrary.
39,40 and
41 With current multimodal treatments, patients with ONB do quite well and some have reported survival rates at 10 years to be greater than 80%.
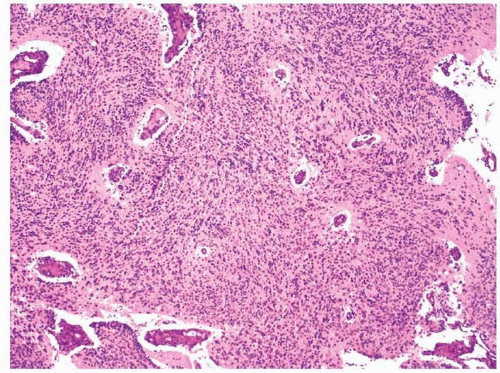
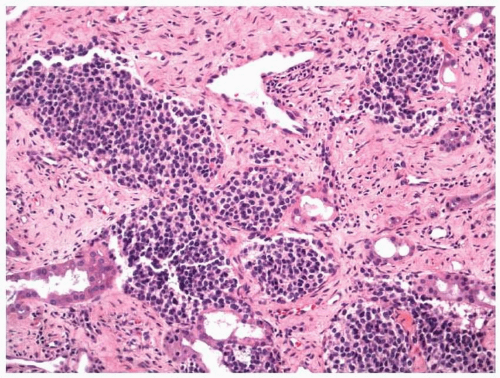
42,43Microscopically, tumor cells grow either diffusely or in discrete, circumscribed nests that are separated by fibrous or edematous stroma (
Figs. 8.12 and
8.13).
35,37 About 25% of cases have definitive Homer Wright rosettes, with annular arrays of neoplastic cells surrounding central, eosinophilic fibrils (
Fig. 8.14, e-
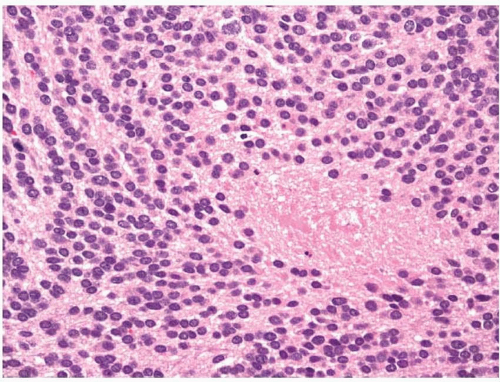
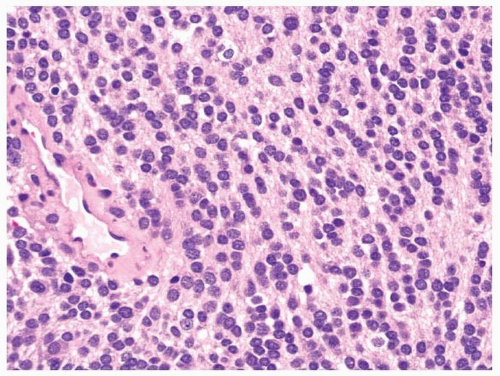
Fig. 8.12). Many more will show more equivocal rosette formations surrounding the fibrillary material and the remainder lack even rudimentary rosettes. An eosinophilic
fibrillary background can be found in most cases (
Fig. 8.15, e-
Fig. 8.13) and calcification will be seen in some examples (e-
Fig. 8.14). Vascular invasion and necrosis, either as single cell apoptosis or as large zones, are often seen. Mature ganglion cells are also identified in some cases (e-
Fig. 8.15). The neoplastic cells are small and usually have minimal
eosinophilic cytoplasm. The nuclei often appear monomorphic and round with delicate granular chromatin. Prominent nucleoli and mitotic figures are usually absent. The tumor can, however, display a wide range of atypia and some cases may show marked variation in nuclear size and shape. Mitotic activity can also vary greatly and some cases have been noted to have more than 10 mitotic figures per high-power field. ONBs have been graded according to the Hyams grading system (
Table 8.3),
which takes into account tumor architecture, nuclear atypia, mitotic activity, necrosis, and the presence or absence of background fibrillary material.
44 There have been mixed reports regarding the utility of this grading system, and it should be noted that it was developed prior to the distinction of other high-grade neuroendocrine tumors of the sinonasal tract, including sinonasal undifferentiated carcinoma (SNUC) (which may have originally been reported as grade 4 ONBs). As a result, most ONBs that we now see would be considered to be grade 1 or 2 neoplasms.
Although many ONBs can be diagnosed based on histology alone, immunohistochemistry is often prudently used for a number of reasons (
Table 8.4).
36,45 The distinction of these lesions from other sinonasal tumors such as SNUCs has significant prognostic value. Furthermore, biopsy specimens are often limited in both tumor quantity and quality, frequently exhibiting marked crush artifact. Most ONBs will show immunoreactivity with antibodies to synaptophysin or chromogranin, as well as with antibodies to less specific markers of neural or neuroendocrine differentiation such as NSE and CD56 (
Fig. 8.16). Although most ONBs do not react with antibodies to cytokeratins, occasional tumors will display focal positivity and thus limited cytokeratin reactivity should not dissuade one from making the diagnosis. In our experience, strong reactivity with antibodies to cytokeratin is very rare with ONBs. S100 protein immunoreactivity, when present, is usually limited to the supporting or sustentacular cells that surround the neoplastic nests (
Fig. 8.17). Occasional tumor cells may show limited reactivity with antibodies to S100 protein; however, staining for other markers of melanoma, such as HMB-45, should not be seen. Finally, membranous reactivity with antibodies to CD99 should not be seen nor should nuclear staining with antibodies to FLI1.