OVERVIEW
- Neck swellings are common findings that present in all age groups from many causes, ranging from congenital to acquired, from cysts, inflammatory, infective to neoplastic disease, encompassing any neck structures
- In the community, the inflammatory lymph node is most common, whereas in hospital thyroid swelling or goitre is most frequently seen
- It behoves all clinicians to understand the embryology and anatomy to aid with making the correct diagnosis thus allowing for appropriate management
- There are more than 100 lymph nodes in each neck, and other organs or glands are singular!
- Knowledge of patient’s age, associated symptoms and anatomical location of the lump, is key to proceeding to treatment in General Practice, or is an indication for referral for further investigations, including imaging and surgery
- Neck lumps in adults (over 40 years) should be considered malignant or at least have malignancy excluded by examination of the mucosal surfaces of the head and neck region, and a needle sample of lump be examined by a pathologist
Neck swellings are commonly encountered and present at all ages. The differential diagnosis of a neck mass is extensive. In the community inflammatory lymph nodes are most common, while in the hospital environment the thyroid swelling or goiter is most frequently seen. It therefore behoves all clinicians to understand the embryology and anatomy to aid with making the correct diagnosis and following an appropriate management algorithm.
Anatomy of the normal neck
The old surgical aphorism, is never more appropriate than when one contemplates the causes of a lump in the neck.
Clinicians are taught to examine a patients’ neck, its landmarks and contents, early in their undergraduate careers, and for the remainder of their clinical life should never have to reconsider what they have been taught. Patients are untaught, and hence when they get a symptom located to their neck, naturally palpate their own neck and that of others, and consider possible diseases diagnoses and become alarmed with what they can feel!
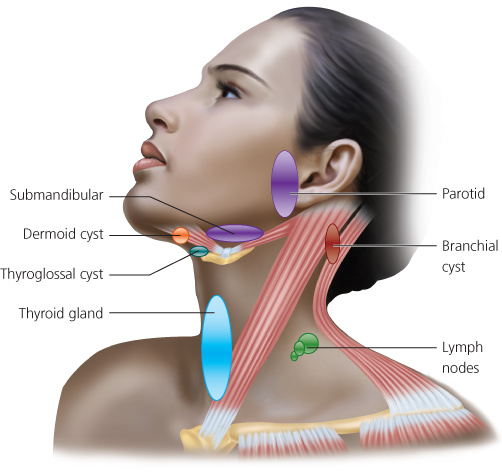
The normal glandular structures are consistent in their location; the thyroid gland is a bilobed structure located along the midline of the neck on either side of the trachea, above the sternal notch, and below the cricoid cartilage. The parotid gland is found in front of the ear or pinna, and extends from the cheek bone (zygoma) above, down and behind to the mastoid tip, below into the upper neck near the hyoid bone and forward onto the cheek for about 2–3 cms. The submandibular gland, is, located below the posterior half of the mandible, but not extending beyond the angle of the mandible, above the hyoid bone (Figure 23.1) (see Chapter 1).
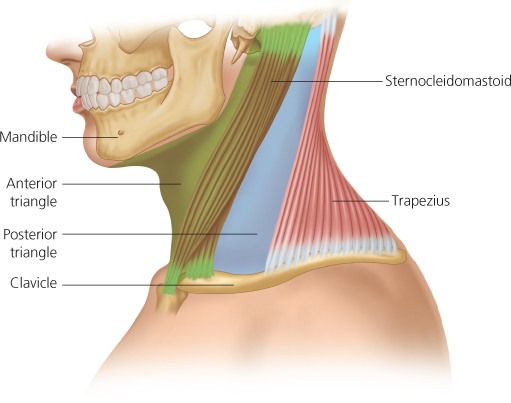
Within each side of the neck there are located more than 100 lymph nodes, usually impalpable, and distributed mainly along the jugular chain, to be found within each of the 5 clinically and anatomically described levels in the anterior neck and in the single but divided level in the posterior neck. The posterior border of the SCM muscle separates the anterior neck from the posterior neck (Figure 23.2). While there are other major structures within the neck, such as nerves, blood vessels, muscles, cartilages and bones, knowledge of their anatomic outline should allow the examiner to consider any such abnormal enlargement or swellings in certain anatomic locations to be included within a differential diagnosis.
Figure 23.2 The lateral neck. Anterior triangle is bounded posteriorly by the posterior border of the SCM muscle, and the posterior triangle is between the posterior border of the SCM and the anterior border of the trapezius muscle and the clavicle inferiorly.
Reaching a diagnosis
Reaching a diagnosis obviously requires some knowledge of the potential pathology. It is difficult to present an exhaustive list of the potential causes of a neck swelling, but a simple classification is tabulated below (Box 23.1).
- Congenital: lymphangiomas, dermoids, thyroglossal cysts
- Developmental: branchial cysts, laryngoceles, pharyngeal pouches
- Skin and subcutaneous tissue: sebaceous cyst, lipoma
- Thyroid swellings: multinodular goitre, solitary thyroid nodule
- Salivary gland tumours: pleomorphic adenoma, Warthins tumour
- Tumours of the parapharyngeal space: deep lobe parotid, chemodectoma
- Reactive neck lymphadenopathy: tonsillitis, glandular fever, HIV
- Malignant neck node: carcinoma metastases (unknown primary), lymphoma
In practical terms, the diagnosis is reached from the patients’ age, the history, location and physical examination of the neck (Box 23.2), followed by a thorough examination of the upper aerodigestive tract and the results of appropriate tests and investigations.
- Age
- History
- Location
- Examination of the lump
- Examination of the head and neck
Age
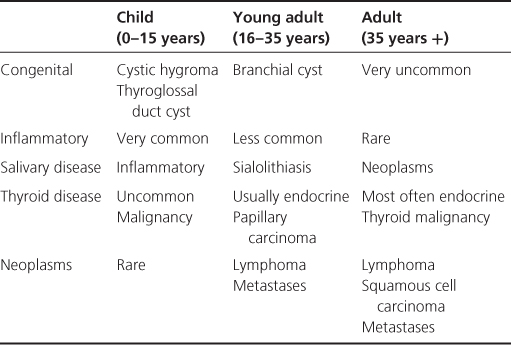
The first consideration should be the patient’s age group (Table 23.1). In general, neck masses in children and young adults are more commonly inflammatory than congenital and only occasionally neoplastic. However, the first consideration in the older adult should be that the mass is neoplastic. The “rule of 80” is often applied as a useful guide. In adults 80% of non-thyroid neck masses are probably neoplastic and 80% of these masses are malignant. This statement probably refers to masses over 2 cm in diameter, in patients over 35 years of age, and for clinicians who are not regularly seeing patients with neck masses. A neck mass in a child, on the other hand, has a 90% probability of being a benign condition of which 55% are congenital.
Table 23.1 Age in relation to possible diagnoses.
History
Onset and duration of symptoms is one of the most important historical points. Inflammatory disorders are usually acute in onset and resolve within 2–6 weeks. Cervical lymphadenitis is often associated with a recent upper respiratory tract infection. In contrast, congenital masses are often present since birth as a small, asymptomatic mass which enlarges rapidly after a mild upper respiratory tract infection. Metastatic carcinoma tends to have a short history with progressive enlargement. Transient post-prandial (after meals) swelling in the submandibular or parotid area is suggestive of salivary gland duct obstruction—a stone or a stenosis. Bilateral diffuse tender parotid enlargement is suggestive of parotitis, most commonly mumps, usually school children, and manifests in local epidemics and can only get the disease once!
One must also be mindful that associated symptoms both specifically to the mass and symptoms suggestive of a systemic process such as fever, night sweats, fatigue or weight loss (consider lymphoma) must be sought and documented (Figure 23.3). Symptoms of sore throat or upper respiratory tract infection may suggest an inflammatory cervical lymphadenopathy. Persistent hoarseness or sore throat, pain on swallowing, cough and sensation of a lump in the throat are risk symptoms of an upper aerodigestive tract malignancy. The symptoms are particularly relevant in patients who are over the age of 40 years and smoke cigarettes. These are the patients who should be referred via the ‘Two week proforma’ to the local ENT service.

Location
While congenital and organ masses are more consistent in their locations, metastatic nodes follow a predictive pattern and help in identifying the primary malignancies (see Chapter 1).
Examination
A full head and neck examination (see Chapter 1) including mucosal surfaces is important, especially when suspecting malignancies (Table 23.2).
Table 23.2 Examination checklist.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


