Granulomatous & Autoimmune Diseases
Granulomatous and autoimmune diseases are characterized by a systemic chronic inflammatory process and a predilection for particular organ systems. Occasionally, patients may present with florid nasal symptoms such as severe crusting, inflammation, and saddle-nose deformity, which raise suspicion early in the evaluation. However, sinonasal manifestations are often nonspecific, including nasal obstruction, rhinorrhea, and recurrent sinusitis. The practitioner must therefore include these diseases in the differential diagnosis of chronic sinonasal symptoms and assess for systemic manifestations in the history and physical examination.
Although obtaining biopsies of suspicious lesions is critical for establishing a diagnosis, specimens often demonstrate nonspecific chronic inflammation and necrosis. Helpful adjunctive tests include inflammatory markers (erythrocyte sedimentation rate and C-reactive protein), complete blood cell count, various autoimmune serologies, chest X-ray, urinalysis, and bacterial and fungal cultures.
The goals of managing the sinonasal manifestations of these diseases are to provide symptomatic relief of nasal obstruction and crusting and to reduce the incidence and severity of secondary sinusitis from ostial obstruction by reducing mucosal edema and facilitating mucociliary clearance. Patients may also require concurrent systemic therapy.
- Severe nasal crusting with friable underlying mucosa, septal perforation, and saddle nose deformity.
- ANCA (antineutrophil cytoplasmic autoantibodies), chest X-ray, and urinalysis.
- Nasal biopsy of suspicious lesions; possible renal biopsy.
Wegener’s granulomatosis is an idiopathic vasculitic and autoimmune process that typically involves the upper and lower respiratory tracts. It occurs in all age groups and predominantly affects white populations. The spectrum of disease presentation ranges from localized to disseminated forms, but the majority of patients have otolaryngologic manifestations. Classically, Wegener’s granulomatosis involves a triad of necrotizing granulomas of the upper and lower airways, glomerulonephritis, and disseminated vasculitis. Upper respiratory tract symptoms may occur in up to 90% of patients, and sinonasal symptoms may be the only systemic manifestation in 30%. The previously undiagnosed patient may present with a pattern of chronic or recurrent sinusitis, managed medically and often surgically with variable clinical improvement.
The more limited, localized form of Wegener’s granulomatosis typically presents with a several-week history of upper respiratory infection symptoms that are unresponsive to standard medical treatment, with the presence of serosanguineous nasal drainage and characteristic pain over the dorsum. Nasal exam is notable for significant bilateral nasal crusting with underlying friable mucosa, particularly over the nasal turbinates, with possible extension to the nasopharynx. Septal perforations may be found with progressive disease, and can lead to saddle-nose deformity due to loss of cartilaginous support and a resultant a dorsal concavity. Other potentially involved head and neck sites are (1) the orbit, with nasolacrimal duct obstruction, orbital pseudotumor, episcleritis, or peripheral ulcerative keratitis; (2) the ear, including serous otitis media, with or without mastoiditis, and possible sensorineural hearing loss; and (3) the larynx and trachea, with subglottic stenosis and tracheal stenosis. Oral cavity ulcerations, gingival hyperplasia, and sialadenitis are rare manifestations of Wegener’s granulomatosis. Systemic symptoms may include weakness, night sweats, and migratory arthralgias. More advanced systemic disease manifests as clinically significant pulmonary and renal pathology, although most patients have renal involvement, even if it is subclinical.
The classification criteria for Wegener’s granulomatosis are the following: (1) oral ulcers and purulent or serosanguineous nasal discharge; (2) abnormal chest X-ray (which may include nodules, cavities, or fixed infiltrates); (3) abnormal urinalysis suggesting renal involvement; and (4) granulomatous inflammation evident on biopsy.
Although the specificity of antineutrophil cytoplasmic antibodies (c-ANCA) for Wegener’s granulomatosis is as high as 98%, the sensitivity varies with disease activity and is 90% in patients with active systemic disease, 60% in patients with localized disease, and 30% for patients in a remission phase. Typically, a positive c-ANCA on immunofluorescence is followed by a confirmatory PR3-ANCA (proteinase 3) on enzyme immunoassay. In a majority of patients, c-ANCA titers parallel disease activity and a titer increase may herald relapse. A positive biopsy characterized by necrotizing granulomata, multinucleated giant cells, and palisading histiocytes is highly suggestive of the diagnosis (Figure 13–1).
The goals of therapy are to induce remission of active disease, maintain remission, and to control adverse effects of disease. The initial goal of therapy is remission induction with cyclophosphamide (2 mg/kg/day) and high-dose glucocorticoids (prednisone 0.5-1 mg/kg/day). Methotrexate may be used instead of cyclophosphamide in more limited forms of the disease. After 1 month of treatment, steroids can be slowly tapered over several months. Cyclophosphamide should be continued for 6–12 months until symptoms disappear and then switched to a less toxic immunosuppressant, such as methotrexate or azathioprine. Investigational therapies include tumor necrosis factor antagonists (etanercept), T-cell inhibitors (lefunomide), and monoclonal antibody therapy (rituximab). Trimethoprim/sulfamethoxazole may have a role for either the limited form of Wegener’s granulomatosis, for pneumocystis pneumonia prophylaxis while on immunosuppressants, or to prevent relapse.
Sinonasal manifestations may be managed medically with low-dose systemic steroids, topical nasal steroids, saline irrigations, and anti-staphylococcal antibiotics when bacterial superinfection is suspected. The role of surgical intervention is limited and may include repair of saddle-nose deformity during a period of remission, septal prosthesis, and conservative endoscopic sinus surgery.
- Chest X-ray (bilateral hilar adenopathy).
- Angiotensin-converting enzyme (ACE) levels positive in 60% of patients with active disease.
- Serum calcium level elevated in 15% of patients.
- Biopsy of suspicious mucosal lesions, labial minor salivary gland, or transbronchial lymph nodes.
The incidence of systemic sarcoidosis is approximately 16.5/100,000 in men and 19/100,000 in women. Approximately 1–4% of patients with sarcoidosis have sinonasal manifestations. The disease is more common in women and in African American and Latin populations, with a peak incidence between the ages of 20 and 40 years and a second peak in women greater than 50.
Sarcoidosis is a chronic granulomatous disease with predominantly pulmonary manifestations, although almost any organ system may become involved. Classic head and neck manifestations include xerostomia and salivary gland enlargement, xerophthalmia, and supraglottic laryngeal lesions causing hoarseness. Other manifestations include lupus pernio (cutaneous sarcoid), neurosarcoidosis, and uveoparotid fever (Heerfordt’s disease), which is the association of uveitis, parotitis, and facial nerve paralysis with sarcoidosis.
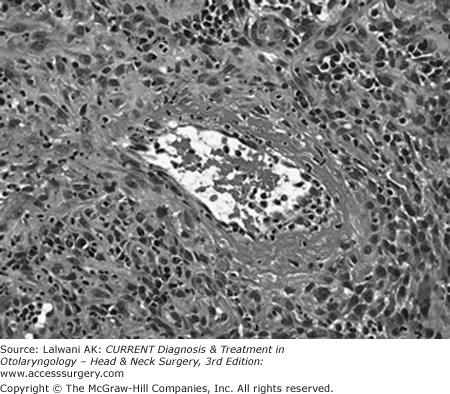
The etiology of sarcoidosis is unknown. The histopathology reveals noncaseating granulomas without necrosis or vasculitis (Figures 13–2A and 13–2B).
Figure 13–2.
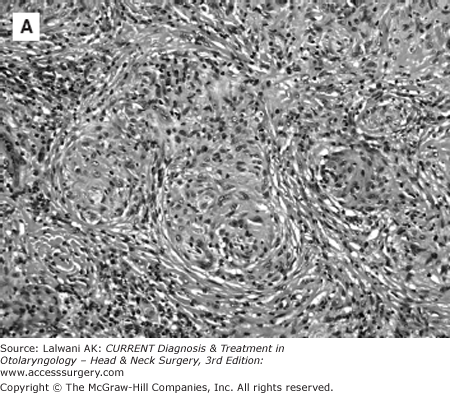

Low-power (A) and high-power (B) H&E stains demonstrating sarcoidosis with confluent non-necrotizing granulomatous inflammation with epithelioid histiocytes. (Contributed by Dr. Syed A. Hoda, Weill Medical College of Cornell University, Department of Pathology and Laboratory Medicine, Anatomic Pathology Division.)
The clinical symptoms associated with sinonasal sarcoidosis are usually nonspecific and include nasal obstruction, chronic crusting, anosmia, epistaxis, postnasal drainage, headache, and recurrent sinus infections. In patients with sinonasal symptoms and coexisting lung disease, sarcoidosis should be in the differential diagnosis. Classic intranasal findings include hypertrophied mucosa and submucosal granulomatous nodules. Other intranasal features suggestive of sarcoidosis include severe nasal obstruction and crusting with friable mucosa, nasal polyps, turbinoseptal synechiae, septal perforation, and external nasal deformity such as saddle nose. A thorough history and head and neck examination may reveal other manifestations. Ultimately, directed intranasal biopsy may be needed to definitively establish the diagnosis. Positive laboratory studies, including elevated ACE and calcium levels, and a chest X-ray, showing bilateral hilar adenopathy are highly suggestive.
Depending on the severity of sinonasal disease, patients may be managed with topical steroids, intralesional steroid injections, or systemic steroids. Nasal irrigation may allow for the mechanical debridement of crusting and thick mucus. Surgical intervention should be avoided when possible but may be necessary for refractory cases of nasal obstruction and chronic sinusitis. For systemic sarcoidosis, oral corticosteroids are the mainstay of therapy. Treatment regimens may also include cytotoxic agents (methotrexate, azathioprine, cyclophosphamide, chlorambucil), anti-malarial drugs (chloroquine and hydroxychloroquine), thalidomide, and TNF-alpha inhibitors (infliximab, adalimumab, etanercept). Overall, therapy should be designed to minimize the use of long-term systemic steroids if the patient’s systemic disease is well controlled.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


