Stridor in Children: Introduction
Stridor is a harsh noise produced by turbulent airflow through a partially obstructed airway. It may be inspiratory, expiratory, or both (biphasic). The term stertor is used to describe airway noise originating in the nose, nasopharynx, and oropharynx; therefore, stridor is generally of laryngeal or tracheal origin. As a general rule, inspiratory stridor originates from the supraglottis and glottis, expiratory stridor from the trachea, and biphasic stridor from the subglottis. There is a wide variety of causes of airway obstruction in children (Table 33–1). This chapter describes the more common laryngeal abnormalities that can cause stridor.
| Congenital | Acquired | |
|---|---|---|
| Supralaryngeal |
|
|
| Laryngeal |
|
|
| Tracheal |
|
|
Laryngomalacia
- Intermittent, positional inspiratory stridor (usually mild).
- Gradual worsening of stridor followed by spontaneous resolution.
- Supraglottic collapse on inspiration.
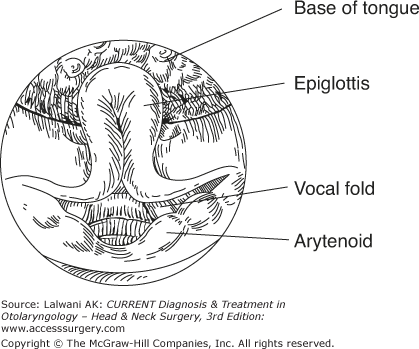
Laryngomalacia is the most common cause of stridor in infants, and is also the most common congenital laryngeal abnormality, accounting for approximately 60% of cases. Stridor occurs as a result of prolapse of the supraglottic structures into the laryngeal inlet on inspiration. The epiglottis is classically described as being omega shaped and folded in upon itself so that the lateral margins lie close to each other (Figure 33–1). The aryepiglottic folds are tall, foreshortened, and thin, and the arytenoids are large with redundant mucosa. Mucosal edema resulting from repeated vibratory trauma to the supraglottis exacerbates the symptoms.
Although most cases of laryngomalacia have a benign course without any long-term sequelae, the most severe cases, in which significant desaturation occurs, can result in significant morbidity, such as pulmonary hypertension and cor pulmonale.
The incidence of synchronous airway lesions associated with laryngomalacia has been reported in 12–45% of cases, although less than 5% of these cases require intervention.
Infants with laryngomalacia usually have no sign of respiratory abnormality at birth. Inspiratory stridor typically develops after a few days or weeks and is initially mild, but over the ensuing months becomes gradually more pronounced, usually peaking at the age of 6–9 months. Spontaneous improvement then occurs and symptoms usually completely resolve by the age of 18 months to 2 years of age. Stridor is not constantly present; rather, it is intermittent and variable in intensity. Typically, symptoms are worse during sleep, stridor being worse when the patient is in the supine position and improved when the patient is prone. Both feeding and exertion tend to result in more pronounced stridor. Although an infant with laryngomalacia usually has a normal cry, stridor may be exacerbated by crying owing to a more forceful inspiratory effort. In most cases, symptoms are mild and self-limiting, but a small proportion of cases have severe stridor, apneic episodes, feeding difficulties, and failure to thrive.
Clinical examination of the patient may reveal no abnormality. If the infant is sleeping or crying, then stridor is more likely to be observed and its associated signs, such as tachypnea and intercostal and subcostal recessions, should be sought. Cyanosis is extremely unusual in laryngomalacia and should raise the suspicion of some other pathology.
The use of a flexible fiberoptic endoscope under local anesthesia is safe and allows a dynamic assessment of the glottis and supraglottis and avoids the risks associated with general anesthesia.
Laryngotracheobronchoscopy is often considered to be an essential study before a definitive diagnosis can be made in order to rule out any synchronous airway pathology.
In severe cases, polysomnography can be performed to detect episodes of hypoxia or hypercapnia. The results of this study can influence the decision to undertake surgical management of the condition.
In most patients, laryngomalacia is a self-limiting condition that does not result in any harm to the patient; therefore, observation is all that is required. In the most severe cases of laryngomalacia, which is encountered in a small percentage of patients, a temporary tracheotomy may be unavoidable.
Surgical intervention is indicated for approximately 10% of patients. The main indications for surgery are severe stridor, apnea, failure to thrive, pulmonary hypertension, and cor pulmonale. A variety of procedures have been described for the treatment of laryngomalacia (referred to as supraglottoplasty), which are largely aimed at reduction of the redundant laryngeal mucosa. These procedures include (1) division of the aryepiglottic folds, (2) excision of a wedge of the aryepiglottic fold with or without trimming the arytenoids or the lateral border of the epiglottis, and (3) suturing of the epiglottis to the base of the tongue. There is disagreement as to whether microdissection or laser surgery is the optimum treatment modality. Physicians who favor laser surgery contend that bleeding is less of a problem compared with microdissection; physicians who favor microdissection maintain that the risk of postoperative scarring is greater with the use of laser.
Complications of supraglottoplasty include bleeding, aspiration, and supraglottic scarring. The risk of supraglottic stenosis is lessened by excising the least amount of supraglottic mucosa to produce an improvement in symptoms. Scarring is particularly problematic in the interarytenoid region; therefore, an island of mucosa must be left in this area.
High rates of reflux have been demonstrated in patients with laryngomalacia, and it has therefore been implicated as a causative factor. However, the relationship remains unproven, hence, the controversy in the antireflux medication for laryngomalacia.
Laryngeal Cysts
Laryngeal cysts are a rare cause of stridor in infants. The two main types of laryngeal cysts are ductal and saccular cysts. Ductal cysts are more common and are thought to originate from obstruction of the submucous glands. They can arise anywhere in the larynx, but are most commonly found in the supraglottis. Saccular cysts arise in the laryngeal ventricle and are usually congenital in infants. Unlike laryngoceles, which usually present in adults, saccular cysts do not communicate with the laryngeal lumen.
Vocal Cord Paralysis
(1) Unilateral Vocal Cord Paralysis
- Hoarse or breathy voice/cry.
- ± Mild dyspnea, stridor, or both.
- ± Aspiration.
- Spontaneous improvement or resolution.
(2) Bilateral Vocal Cord Paralysis
- Severe stridor.
- ± Aspiration.
- Usually requires tracheotomy.
Vocal cord paralysis in infants and children can be either congenital or acquired and either unilateral or bilateral. It is the second most common congenital abnormality of the larynx, accounting for approximately 10% of cases. Congenital vocal cord palsy is slightly more common in males, and is more commonly bilateral.
There are many causes of acquired vocal cord palsy (Table 33–2), although most commonly the paralysis is idiopathic. Central nervous system (CNS) abnormalities usually result in bilateral vocal cord palsy. The most common congenital CNS abnormality resulting in vocal cord palsy is the Arnold–Chiari malformation. Acquired CNS causes of vocal cord paralysis are rare in infants and children, as are acquired peripheral neuropathies. Congenital abnormalities of the heart and great vessels may lead to vocal cord palsy, or the paralysis may result from surgery to correct these abnormalities. In this situation, the left side is more commonly affected because of the longer course of the left recurrent laryngeal nerve through the mediastinum. Rarely, esophageal surgery, such as repair of a tracheoesophageal fistula, can result in a bilateral palsy. Other traumatic causes of vocal cord paralysis include birth trauma, intubation, and head injury. Inflammatory conditions such as encephalopathies and Guillain–Barré usually produce bilateral vocal cord paralysis. Neoplastic causes of vocal cord palsy are rare in infants and children. Familial X-linked vocal cord paralysis has been reported, but is extremely rare.
| Idiopathic |
Central Nervous System Arnold–Chiari malformation Hydrocephalus Encephalocele Syringomyelia or syringobulbia |
Peripheral Nervous System Myasthenia gravis Myotonic dystrophy Charcot–Marie-Tooth disease |
Trauma Surgical Head injury Endotracheal intubation Birth trauma |
Neoplasia Thyroid carcinoma |
Inflammatory Viral Bacterial Granulomatous |
Cardiovascular Anomalies Tetralogy of Fallot Cardiomegaly Patent ductus arteriosus Vascular rings |
The symptoms arising from vocal cord palsy vary from the patient being asymptomatic to having an acute airway obstruction that requires emergency intervention. Patients with unilateral vocal cord palsy do not usually have signs of airway obstruction. The usual presenting features are a hoarse, breathy voice or cry and a weak cough. Feeding problems and aspiration are more likely to occur if the lesion is proximal to the superior laryngeal nerve since this nerve supplies sensation to the supraglottis. Bilateral vocal cord paralysis tends to have more pronounced symptoms such as stridor, apnea, and cyanosis; however, if the vocal cords lie in the intermediate position, then airway obstruction does not occur and aspiration is the primary problem.
If any doubt about the stability of the airway exists, then the patient should be evaluated in the operating room and the airway secured before further investigation is considered.
Although fiberoptic endoscopy can reliably demonstrate vocal cord palsy, the airway needs to be assessed by laryngotracheobronchoscopy for two reasons: (1) the arytenoid cartilage must be palpated to exclude the rare finding of a fixed cricoarytenoid joint; (2) the possibility of synchronous pathology in the airway must be excluded.
If a cause is not apparent, then a magnetic resonance imaging (MRI) scan including the brain, brainstem, neck, and chest (the course of the vagus and recurrent laryngeal nerves) should be performed. In patients in whom aspiration is suspected, a contrast swallow or videofluoroscopy can provide information on deglutition and laryngeal penetration. Functional endoscopy evaluation of swallowing is also used in the pediatric group.
The function of the glottis is to protect the lungs from the aspiration of food while providing an adequate airway. A secondary, though important, function is to provide a voice. Management decisions are influenced by the underlying cause, the severity of symptoms, and the likelihood of spontaneous recovery. Spontaneous recovery occurs more frequently in acquired than in congenital vocal cord palsy, and it is also more likely in unilateral than bilateral vocal cord palsy.
Most children with unilateral vocal cord paralysis have minimal symptoms because the normal vocal cord adopts a more medial position to compensate for the paralyzed vocal cord. If poor voice quality is persistent, then speech therapy is the preferred treatment. In the rare instance in which the airway is significantly compromised, tracheotomy is indicated. Successful decannulation without the need for further laryngeal surgery is usually possible as the larynx develops.
In children with bilateral vocal cord palsy, the vocal cords usually lie in the adducted position, which results in a compromised airway. This circumstance indicates that the majority of cases of bilateral vocal cord palsy will require a tracheotomy to maintain the airway. Once a tracheotomy has been performed, serial endoscopy should be planned to monitor any spontaneous recovery of vocal cord function. It is recommended that irreversible surgical procedures on the larynx are not considered for at least 1 year after a tracheotomy. Some otolaryngologists prefer to wait until the child is old enough to make his or her own decision about further surgery. The aim of surgery for permanent bilateral vocal cord palsy is to produce an airway of sufficient size to allow decannulation without compromising the protective function of the larynx or producing an unacceptable voice quality. Various surgical techniques have been described to accomplish this goal.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


