Introduction
Hair is one of the few physical characteristics over which we have voluntary control. The length, the color, and how we style our hair are a reflection of our personality and how we project ourselves to the world. When our hair involuntarily begins to disappear, it is a source of ongoing emotional and psychological stress for many men and women.
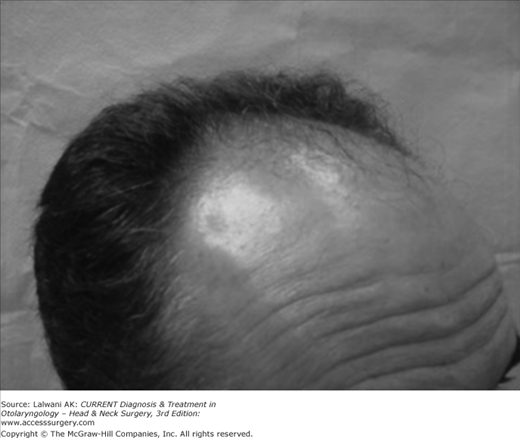
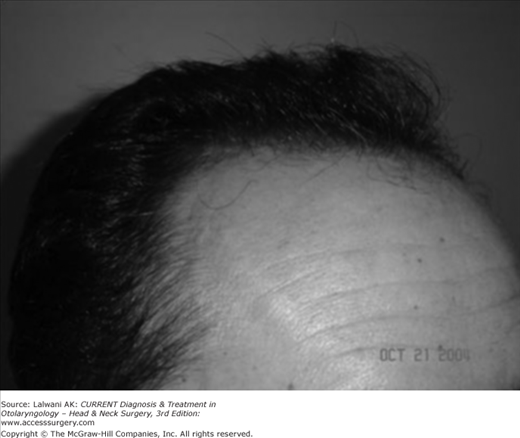
Fortunately, modern techniques in hair transplantation can consistently restore a natural frame of hair around the face (Figures 76–1 and 76–2). The era of large, pluggy, unnatural transplanted hair, which existed from the 1960s until 1990s no longer exists. Currently, the cosmetic standard for transplantation is to create consistently natural appearing transplanted hair for men and women. This chapter will be an overview of state-of-the-art techniques in hair transplantation.
The Consult
As with all surgical procedures, a consultation is vital to the success of the procedure. In addition to a physical examination, a thorough hair loss and medical history should be obtained. Key questions include: How long the hair loss has been going on? What medications have been used to date, and with what success? What is the goal of the patient from the procedure?
On physical exam, the caliber of hair follicles and available donor density are the two most important physical characteristics to determine. Patients with thick caliber, coarse hair and high donor density will be able to create the perception of thick transplanted hair while patients receiving an equal number of fine caliber follicles, with poor to average donor density will appear to have received much less hair.
The physician should review the ongoing nature of male and female pattern hair loss. Patients should be aware that the net perceived density of the procedure equals the number of follicles transplanted minus their ongoing hair loss. For all patients, the role of minoxidil and finasteride for men, and minoxidil for women should be reviewed. Both medications are FDA-approved and are highly effective to help maintain existing hair.
If a patient uses a medication and undergoes hair transplantation, there can be a substantial increase in perceived density, both short and long term. Despite the success of medications, it should also be emphasized that the medications are elective and can be stopped at any time. It is the obligation of the surgeon to plan a transplant anticipating future hair loss. If a patient ever does discontinue the medication and more of their original hair is lost, the transplant should appear natural both short and long term.
The key to success is to create realistic expectations based on each patient’s physical exam, ongoing hair loss, and individual goals.
Donor Harvesting
Hair transplantation is based on the theory of donor dominance, which states that hair transplanted from the posterior scalp and moved to the front of the scalp will maintain its natural genetic destiny and not to be affected by male or female pattern hair loss. The donor ellipse and follicular unit extraction (FUE) are the two techniques for harvesting hair follicles.
Ellipse
Elliptical donor harvesting is performed in the vast majority of patients. It is comparable to any other cutaneous excision, such as for skin cancer removal. The donor hair is trimmed to a length of 1–2 mm (Figure 76–3). The patient is placed in the prone position for optimal ergonomics using a special prone pillow. The skin is infiltrated with local anesthesia. To obtain optimal hemostasis the infiltration should be performed in the dermis rather than the subcutaneous area. The ellipse is removed either with an individual scalpel or utilizing double bladed knives with two #10 blades. The width of the donor ellipse should be kept to 1 cm or less in order to have minimal tension on the donor wound. This should result in a 1–3 mm wide donor scar (Figure 76–4). Also, various techniques exist for minimizing the appearance of the donor scar, so that the underlying hair may “grow through” the scar. The length of the donor ellipse depends on the desired number of hair grafts for the procedure.

Figure 76–4.
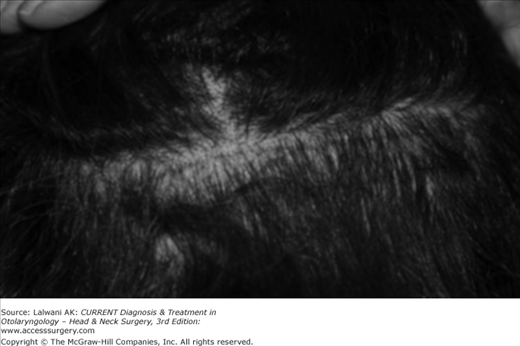
Donor scar 7 days postoperatively.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


