Diving Medicine: Introduction
Constantly increasing in number, the recreational and commercial diving community frequently presents with problems poorly understood by the average physician and otolaryngologist unless they have had some training in diving medicine. The consequences of breathing compressed gas mixtures under increasing barometric pressure and subsequent decreasing barometric pressure are confusing unless one understands the physics and physiology of the pressure environment. A well-trained otolaryngologist can be better prepared to treat the conditions that divers encounter by understanding the cause of these conditions.
Diving Physics
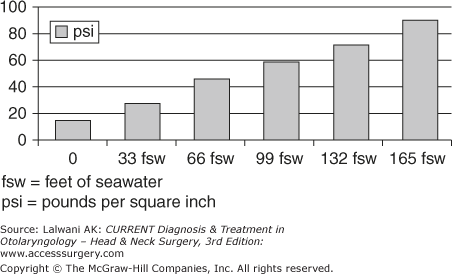
Living at the sea level, our bodies are surrounded by one atmosphere of pressure (eg, 14.7 psi, 760 mm Hg, and 1 bar). The entire earth’s atmosphere exerts this pressure, and it is exerted uniformly against our bodies. Pascal’s principle states that any change in pressure in an enclosed fluid is transmitted equally throughout that fluid. The human body, being to a large extent fluid, pushes out against the ambient pressure with the same force as the surrounding media. For this reason, divers can descend in the water to extreme depths with ease. It is only the air-filled spaces in our bodies that are affected by the changes in pressure. For each 33 ft of seawater (ie, 34 ft of fresh water, or 10 m) through which we descend, we add an additional atmosphere of pressure. The pressure is doubled going from sea level to 33 ft of seawater, but is not doubled again until 99 ft of seawater is reached (Figure 57–1).
Conversely, as one ascends from depth, the pressure is decreased at the same rate. Boyle’s law states that if the absolute temperature remains constant, the volume of a gas varies inversely as the absolute pressure. Because water temperature remains within a small absolute range, as a diver descends in the water, the air-filled spaces decrease in volume proportionately. As the diver ascends, the air-filled spaces increase in volume proportionately. Since we double the pressure from the surface to 33 ft of seawater and not again until 99 ft of seawater, the greatest pressure and volume changes occur closest to the surface. With the exception of decompression sickness, most divers’ problems occur in the shallow depths, even as shallow as 4 ft of seawater.
Dalton’s law of partial pressure states that in a mixture of gases (eg, air), the total pressure exerted by that mixture is equal to the sum of the partial pressures of each gas in the mixture. Both nitrogen and oxygen, composing most of the air we breathe, increase in partial pressure as the ambient pressure increases. Henry’s law of solubility of gases states that as the partial pressure of a gas increases, more of that gas is dissolved in the surrounding liquid until saturation occurs. Since oxygen is utilized in metabolism, nitrogen, which is metabolically inert, is driven into solution in the circulating fluids of the body (eg, blood and lymph) in increasing amounts with increasing ambient pressure. Conversely, as ambient pressure is decreased, the dissolved gas becomes supersaturated and is released as gas bubbles. The latter two laws account for the indirect effects of pressure and are responsible for decompression sickness, or the bends, to be discussed later.
External Ear Disorders
Because divers spend much of their time in the water, they are subject to the same cutaneous problems of the external ear as are swimmers.
External otitis is very common and needs to be treated in the same fashion as external otitis that does not result as a complication of diving. In mild cases of pruritus, which are indicative of atopic external otitis, treatment can be limited to steroid drops both prophylactically and therapeutically. This is more of a chronic problem and treatment can be administered as needed. The more severe forms may require steroid–antibiotic drops with a wick being placed if the ear canal is completely closed. For severe infections, broad-spectrum antibiotics may be added. The prognosis is excellent and prophylaxis may prevent further infections. The use of acid–alcohol drops before diving and after leaving the water may prevent infection. One should wait until all the symptoms have resolved, the ear canal has returned to normal diameter, and hearing is restored. Prophylactic antibiotic drops may be needed for several weeks after the infection has cleared.
Foreign bodies in the external ear canal, including cerumen, can be driven into the ear canal by the increasing water pressure and can either be lodged at the narrow portion of the canal or driven against the tympanic membrane. If they are lodged at the narrow portion of the ear canal and there is an air-filled space between the foreign body and the tympanic membrane, this air space is subject to Boyle’s law, as stated above. The volume of the air space decreases with increasing ambient pressure, producing pain, and hearing loss. There may be hemorrhage in the canal and on the outer surface of the tympanic membrane, and blebs, and edema may be found after the foreign body is removed. Earplugs should never be used while diving unless they have a small vent hole. Treatment is removal of the foreign body and topical antibiotic eardrops.
Although exostoses can occur in divers who are also surfers; those who dive in cold water usually wear a thermal protective hood, which can prevent the formation of exostoses. If they are obstructive, they can be removed surgically.
Middle Ear Disorders
As the diver descends in the water column, the air-filled space of the middle ear is subject to the effects of Boyle’s law. With increasing pressure, the volume of the gas in the middle ear reduces proportionately and must be equalized by some technique (see equalizing techniques later in the chapter). Frequent equalization is required near the surface as one descends and less so as the diver achieves greater depth. If equalization is not performed, the volume of the middle ear gas is reduced to the point that the tympanic membrane is retracted severely and fluid or blood (or both) is secreted into the middle ear, reducing the volume and equalizing the pressure. Alternately, the tympanic membrane may rupture.
Because of the unique etiology of diving disorders, the treating physician will see the entire spectrum of middle ear disease from eustachian tube obstruction, occurring rapidly, rather than over an extended period. Because this spectrum is caused by pressure changes, and usually on descent, it is referred to as barotrauma.
Occasionally, middle ear barotrauma can occur with ascent. In this case, the middle ear is equalized at depth, or partially so, and the diver ascends with an obstructed eustachian tube due to rebound rhinitis. The air in the middle ear space increases in volume with a decrease in ambient pressure, and if the middle ear is not vented via the eustachian tube, there will be pain and possible rupture of the tympanic membrane into the external ear canal. Descending to a deeper depth can relieve these symptoms; however, the diver is usually ascending because his/her breathing gas supply is low. Swallowing continually and ascending very slowly may partially relieve the symptoms, but if the gas supply is low, returning to the surface is mandatory. The symptoms, findings, and treatment are the same as for barotrauma of descent.
Middle ear barotrauma can be prevented by not diving when there is any condition that might lead to eustachian tube obstruction (including upper respiratory infection or allergy). The diver should be able to easily equalize the middle ear. Prophylactic oral decongestants, short courses of nasal decongestants (no longer than 3 days because of possible rebound rhinitis), and steroid nasal sprays can assist in preventing obstruction.
Symptoms of middle ear barotrauma range from a dull feeling in the ear to pain and hearing loss. If a perforation of the tympanic membrane occurs, there will be vertigo with nausea and vomiting caused by the passage of water that is colder than body temperature into the middle ear; this water stimulates the lateral semicircular canal (a caloric stimulation).
Physical findings can be as simple as retraction, erythema and injection, or hemorrhage in the tympanic membrane. More severe findings include serous otitis, hemotympanum, and perforation of the tympanic membrane. Tuning fork tests and audiograms reveal a conductive hearing loss.
Treatment of middle ear barotraumas consists of oral decongestants, short-term decongestant nasal sprays, and appropriate antibiotics if secondary infection is present. The diver should stay out of the water until the middle ear is healed and the diver can easily equalize the middle ear. If a perforation occurs, one must wait until the perforation heals and the tympanic membrane is intact again. If surgery is required for a nonhealing perforation, the above requirements must be met, usually requiring 3–4 months after surgery.
Divers should not return to diving until all the symptoms and findings have cleared. There should be ease of equalization of both middle ears confirmed by physical examination, tympanometry with a Valsalva maneuver, or both.
There remains controversy among otologists as to if or when divers who have had middle ear surgery can return to diving. The conditions that usually require myringoplasty or tympanoplasty are caused by eustachian tube obstruction. The surgical site and procedure should be completely healed with no evidence of difficulty in equalizing the middle ear. If ancillary conditions (eg, allergy or sinus disease) contributed to the need for middle ear surgery, they should be completely cleared, and if they recur, diving should be avoided.
Inner Ear Disorders
Two mechanisms have been postulated as causing inner ear barotrauma. As the diver descends with difficulty in equalizing the middle ear space and continues to descend, attempting to forcefully equalize the middle ear, there can be a sudden opening of an obstructed eustachian tube with a rush of air into the middle ear space. This can rupture one of the windows between the middle ear and the inner ear–either the fenestra rotundum (ie, round window) or the fenestra ovalis (ie, oval window)–into the inner ear.
Conversely, if the diver descends with difficulty in equalizing the middle ear space and continues to descend, attempting to forcefully equalize the middle ear, and the eustachian tube does not open, the force is transmitted (as in a Valsalva maneuver) via the spinal fluid, through the cochlear aqueduct to the perilymphatic space of the inner ear. The round or oval windows can rupture into the middle ear.
Prevention consists of avoiding situations that require forceful autoinflation of the middle ear, straining, or both.
Both mechanisms that cause inner ear barotrauma produce a perilymphatic fistula. The round window is more commonly affected than the oval window, but occasionally both windows rupture.
Symptoms include tinnitus, vertigo with nausea and vomiting, and hearing loss, which occur usually while descending. There may be pain due to a concomitant middle ear barotrauma. There is usually evidence of middle ear barotrauma, but the tympanic membrane may look perfectly normal. The hearing loss is sensorineural, accompanied by nystagmus and a positive fistula test.



