Essentials of Diagnosis
General Considerations
According to the World Health Organization, the proportion of population that are elderly is increasing at a rapid rate—by 2025, nearly 1.2 billion people will be over the age of 60! Consequently, the prevalence of age-related auditory and vestibular dysfunction will increase. Genetically determined and environmentally affected, the inner ear, like other organ systems, undergoes degenerative changes with aging. These changes result in a variable functional disability. In the United States, hearing difficulty is reported by 25–30% of people in the age group of 65–70 years and by nearly 50% of those over 75 years of age. It has been estimated that between 1.5% and 3.0% of the total population would benefit from hearing aids. Vestibular dysfunction is also common in the elderly, with reported prevalence of vertigo, dysequilibrium, or imbalance to be as high as 47% in men and 61% in women over the age of 70. The incidence of falling in individuals over the age of 65 is between 20% and 40% in those living at home and is twice as frequent for the institutionalized elderly. These falls are associated with significant morbidity and mortality and constitute one of the leading causes of death among the elderly.
The specialized neural cells of the auditory and vestibular systems are nonmitotic and thus cannot undergo replication and renewal. During the course of a lifetime, DNA transcription errors and insoluble pigments accumulate, and protein synthesis becomes increasingly inefficient. In addition, environmental and external factors such as noise trauma, physical trauma, ototoxic substances, and medications contribute to senescence. More recently, the contribution of genetics to age-related hearing loss is being appreciated.
Pathogenesis
Hearing loss in the elderly is multifactorial and is due to the convergence of various risk factors. Presbycusis is the otherwise unexplained, slowly progressive, predominantly high-frequency symmetric hearing loss due to the aging process (Figure 53–1). Progressive high-frequency hearing loss has been clearly documented by numerous studies in populations over the age of 40 (Figure 53–2A). Older patients with presbycusis also have more diminished speech discrimination than younger patients with the same level of pure-tone averages (Figure 53–2B). This suggests that neural processing is affected in addition to end-organ dysfunction.
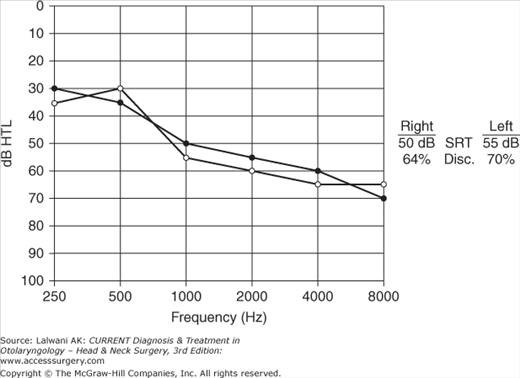
Figure 53–2.
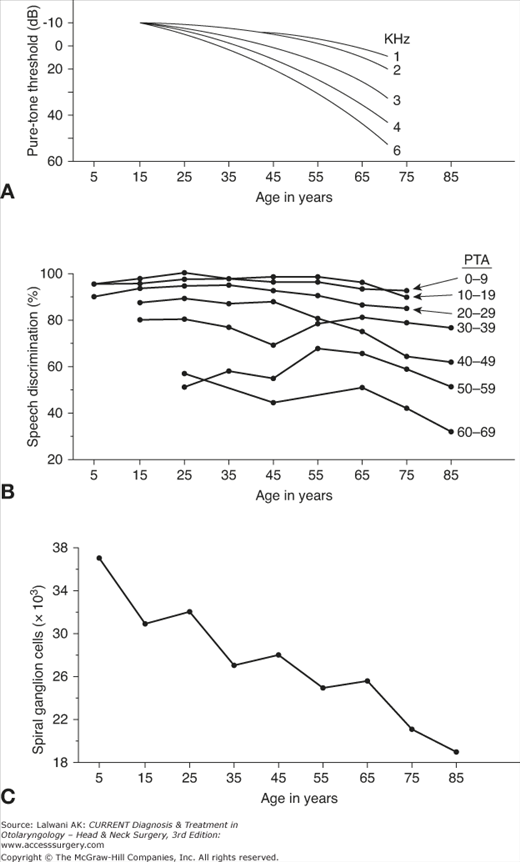
(A) Hearing level as a function of age. Pure-tone hearing level increases with age, and higher frequencies are affected more than the lower frequencies (adapted from Glorig A, Davis H. Age, noise and hearing loss. Ann Otol Rhinol Laryngol 1961;70:5571). (B) Speech discrimination as a function of age. For a given pure-tone hearing loss, the speech discrimination decreases with aging (adapted from Jerger J. Audiologic findings in aging. Adv Otorhinolaryngol 1973;20:115). (C) Total ganglion cell population versus age. There is progressive loss of cochlear neurons as a function of aging (adapted from Otte J, Schuknecht HF, Kerr AG. Ganglion cell populations in normal and pathological human cochleae. Implication for cochlear implantation. Laryngoscope 1978;88:1234).
Central pathology includes increased synaptic time in the auditory pathway, increased information processing time, and decreased neural cell population in the auditory cortex. Thus, the older patient is handicapped by decreased hearing as well as the decreased ability to discriminate between similar words. The ability to discriminate between words further deteriorates in a noisy background. In addition, the ability to identify very small interaural time differences deteriorates. Consequently, there is a decrease in directional hearing, further limiting the understanding of speech.
The hearing loss that occurs with aging is not inevitable. Some individuals reach advanced age and maintain perfectly normal hearing. For example, the Mabaans, a Sudanese tribe who live in an almost silent environment, exercise daily, and abstain from smoking and eating animal fats, have significantly better hearing than age-matched control groups from industrialized areas in the United States. Similarly, other studies have shown that hearing loss is associated not only with noise exposure, but with hyperlipidemia, hypertension, and vascular disease. This has led some clinicians to consider presbycusis as “socioacusis” and to suggest that preventive measures such as limiting exposure to noise may substantially reduce the hearing loss that accompanies aging. Through military, industrial, and recreational (eg, hunting or target practice) activities, men typically receive significantly greater noise exposure than women. Thus, the higher incidence and greater severity of presbycusis in men also argues in favor of the role of environmental causes.
Morphologic studies of human temporal bones have demonstrated an age-related loss of inner and outer hair cells and supporting cells, with the greatest loss being in the basal turn of the cochlea. There is greater loss of outer hair cells compared with inner hair cells; however, these changes have not been directly correlated with auditory function. Age-related loss in spiral ganglion cells, eighth nerve fibers, and neurons in cochlear nuclei have been demonstrated (Figure 53–2C). Some studies have reported changes in the brainstem-evoked response with aging, suggesting alteration at the level of the superior olivary complex, the lateral lemniscus, or the inferior colliculus. Thus, age-related auditory dysfunction results from aggregate deterioration of the entire auditory pathway.
The exact cause of presbycusis remains speculative, in part because of the difficulty in separating the contribution of various etiological factors such as diet, nutrition, metabolism, arteriosclerosis, ototoxic exposure, and noise trauma. Many believe that genetic predisposition alone makes age-related biologic degeneration of the auditory system inevitable. Lifelong acoustic trauma and genetically programmed senescence are the most likely causes of age-related hearing loss. Recently, genome-wide association studies demonstrated that a common allele of GRM7 (gene encoding metabotropic glutamate receptor type 7) contributes to an individual’s risk of developing age-related hearing loss.
Degenerative changes and atrophy have been noted throughout the vestibular apparatus, including the otoconia, vestibular epithelium, vestibular nerve, Scarpa’s ganglion, and cerebellum. In the otolithic organs (the utricle and saccule), statoconia progressively demineralize and fragment, resulting in a decreased responsiveness to gravity and linear acceleration. The migration of degenerated otoconial debris into the dependant ampulla of the posterior semicircular canal may result in positional balance disturbances (cupulolithiasis or benign paroxysmal positional vertigo). After age 70, there is also a 20% decrease in the number of hair cells in the maculae of otolith organs and a 40% decrease in cristae of the semicircular canals. Type I hair cells are affected more than Type II hair cells.
In the sensory epithelium, there is accumulation of inclusion bodies, lipofuscin, and vacuoles. Atrophy and scar formation are also present in the sensory epithelia. A reduction in the number of ganglion cells in the Scarpa’s ganglion occurs earlier, by age 60. Beginning at age 50, there is a loss of nerve fibers between the vestibule and the Scarpa’s ganglion. The greatest loss occurs among the thick myelinated fibers of the cristae. Lipofuscin accumulation in the vestibular nuclei has also been observed. In the cerebellum, there is loss of Purkinje cells beginning in the fifth decade. Presbyastasis is a dysequilibrium that occurs with aging and should be used only as a diagnosis of exclusion.
Clinical Findings
Classically, four types of presbycusis have been defined: sensory, neural, metabolic or strial, and conductive (Table 53–1). These types may occur in isolation or in combination.
| Type | Pure Tones | Speech Discrimination |
|---|---|---|
| Sensory | High tones, abrupt slope | Related to frequencies lost |
| Neural | All frequencies | Severe loss |
| Strial | All frequencies | Minimal loss |
| Cochlear conductive | High tones, gradual slope | Related to steepness of high-tone loss |
Sensory presbycusis is audio-metrically characterized as bilateral, symmetric high-tone hearing loss with an abruptly sloping threshold pattern that begins in middle age. Speech discrimination is directly correlated with the preservation of high-frequency hearing. Histologically, there is a loss of both hair cells and supporting sustentacular cells isolated to the basal turn of the cochlea. The initial flattening of the organ of Corti is followed by secondary neural degeneration. The middle and apical turns of the cochlea containing the speech frequencies are usually spared. These pathologic changes are similar to those seen with noise trauma.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


