Anatomy, Physiology, & Testing of the Facial Nerve: Introduction
The facial nerve is directly and indirectly involved in numerous pathological conditions affecting the temporal bone, ranging from infection to neoplasia. In each instance, a solid understanding of its complex anatomy is crucial to the physician’s ability to both diagnose and treat disorders of the facial nerve.
The facial nerve (Figure 69–1) begins its development near the end of the first month of gestation, when the acousticofacial primordium, giving rise to both the facial and acoustic nerves, develops adjacent to the primordial inner ear, the otic placode. The geniculate ganglion, which arises from the second branchial arch, develops early in the second month of the gestation. Adjacent to the developing geniculate ganglion, the acousticofacial primordium differentiates into a caudal and a rostral trunk. The caudal trunk progresses into the mesenchyme of the second branchial arch, becoming the main trunk of the facial nerve. The rostral branch becomes associated with the first arch, eventually developing into the chorda tympani nerve, providing taste to the anterior two-thirds of the tongue. This development partially explains the close association of the chorda tympani with the facial nerve.
Figure 69–1.
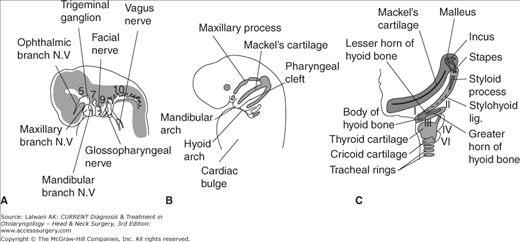
A schematic illustration demonstrating the embryology of the facial nerve. (A) The location of the primitive facial nerve in the developing embryo is shown in relation to other important nerves in the head and neck. (B) The location of the second branchial arch giving rise to the main trunk of the facial nerve is shown in relation to the other branchial arches. (C) Other derivatives of the second branchial arch are shown and help explain the complex innervation pattern of the facial nerve. (Reproduced with permission from Langman J & Sadler TW, Langman’s Medical Embryology, 5th ed. Williams and Wilkins: Baltimore, MD; 1985.)
Both the geniculate ganglion and the nervus intermedius, arising from the second branchial arch, form independently of the motor division of the seventh nerve. During the sixth week of gestation, the motor division of the facial nerve establishes its position in the middle ear between the membranous labyrinth (an otic placode structure) and the developing stapes (a second arch structure). The nerve then passes into the mesenchyme of the second arch. During this time, the chorda tympani nerve becomes associated with the trigeminal nerve, which will carry the chorda tympani on its way to the tongue via the lingual nerve. The greater superficial petrosal nerve, which carries preganglionic parasympathetic fibers toward the pterygopalatine ganglion, also develops during this time period.
Most of the anatomic relationships of the facial nerve are established by the end of the second gestational month. Although the fallopian canal, the bony canal that transmits the facial nerve through the temporal bone, begins its development in the fifth gestational month, it is not complete until several years after birth. The incomplete development of this canal is though to be responsible for the natural dehiscences that may contribute to facial palsies that are associated with childhood otitis media.
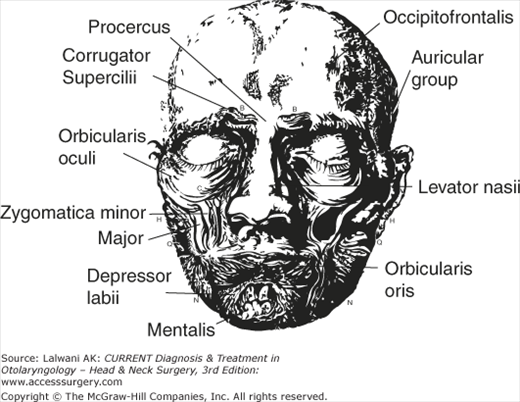
During the sixth gestational week, the extratemporal portion of the facial nerve begins development. By the end of the second gestational month, all five divisions of the extratemporal nerve—the temporal, zygomatic, buccal, mandibular, and cervical branches—are present. Over the third month, the nerve becomes enveloped by the parotid gland. The facial muscles (Figure 69–2), developing independently, are formed at 7–8 week gestation and must be innervated by the distal facial nerve branches or else will degenerate. By the end of the third gestational month, a majority of the facial musculature is identifiable and functional.
At birth, the facial nerve is located just beneath the skin near the mastoid tip, as it emerges from the temporal bone. This nerve is thus placed at risk when a postauricular incision is made in a young child, as is often done for ear surgery. As the mastoid tip forms and elongates during childhood, the facial nerve assumes its more medial position. Individual axons of the facial nerve also undergo myelination until the age of 4Â years, an important consideration during electrical testing of the nerve during this time period.
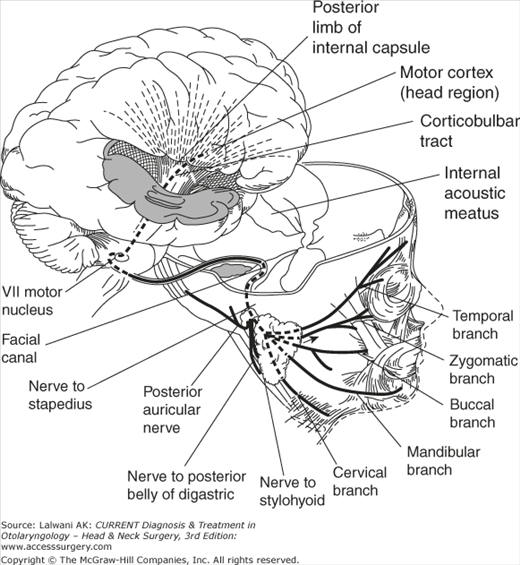
The primary somatomotor cortex of the facial nerve is located in the precentral gyrus, corresponding to Brodmann areas 4, 6, and 8. It is from this region that the complex voluntary motor functions of the facial nerve, such as facial expression, are controlled (Figure 69–3). Neural projections from this area combine into fascicles of the corticobulbar tract during their descending course through the internal capsule. These neural projections continue through the pyramidal tracts within the basal pons. In the caudal portion of the pons, most of the facial nerve fibers cross the midbrain to reach the contralateral facial nucleus. A small number of facial nerve fibers innervate the ipsilateral facial nucleus, a majority of which are destined for the temporal branch of the nerve. This distinction becomes important when the clinician is trying to determine if a facial paralysis is due to a central or peripheral lesion: central lesions spare the forehead muscle since they receive input from both cerebral cortices, whereas peripheral lesions will involve all branches of the facial nerve.
In addition to these voluntary neural projections to the facial nerve, there is also an extrapyramidal cortical input to the facial nucleus from the hypothalamus, the globus pallidus, and the frontal lobe, all of which control involuntary facial expression associated with emotion. Additional projections to the facial nuclei from the visual system are involved in the blink reflex. Projections from the trigeminal nerve and nuclei contribute to the corneal reflex, whereas those from the auditory nuclei help the eye close involuntarily in response to loud noises.
The efferent projections from the facial motor nucleus emerge dorsomedially to form a compact bundle that loops over the caudal end of the abducens nucleus beneath the facial colliculus or internal genu (or turn). The neurons then pass between the facial nerve nucleus and the trigeminal spinal nucleus, emerging from the brainstem at the pontomedullary junction (Figure 69–4).
Figure 69–4.
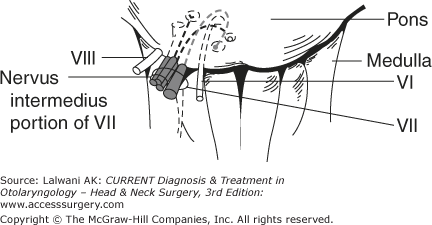
The anatomy of the facial nerve (CN VII), cochlear nerve, and vestibular nerve (CN VII), as they exit the brainstem at the level of the pontomedullary junction. (Reproduced, with permission from Wilson-Pauwels L, Akesson EJ, Stewart PA, Cranial Nerves: Anatomy and Clinical Comments. B.C. Decker Inc.: Toronto; 1988.)
In addition to supplying motor innervation to the muscles of facial expression, other neuronal projections found in association with the facial nerve are partially responsible for taste, cutaneous sensation of the external ear, proprioception, lacrimation, and salivation (Table 69–1; Figure 69–5). This bundle of these nerves, termed the nervus intermedius, or Neve of Wrisberg, exits the brainstem adjacent to the motor branch of the facial nerve. The general visceral efferent fibers of the nervus intermedius are preganglionic parasympathetic neurons that innervate the lacrimal, submandibular, sublingual, and minor salivary glands. The cell bodies of these nerves arise in the superior salivatory nucleus and join the facial nerve after it has passed the abducens nucleus. They travel together until reaching the geniculate ganglion in the temporal bone. At this point, the greater superficial petrosal nerve branches offs, containing the neurons destined for the pterygopalatine ganglion. The greater superficial petrosal nerve ultimately innervates the lacrimal, minor salivary, and mucosal glands of the palate and nose. The remaining fibers form part of the chorda tympani nerve, proceed to the submandibular ganglion, and eventually proceed to the submandibular and sublingual salivary glands.
| Facial Nerve Subdivision | Function |
|---|---|
| Branchial motor |
|
| Visceral motor |
|
| General sensory |
|
| Special sensory | Chorda tympani nerve—taste to anterior two-thirds of the tongue |
Figure 69–5.
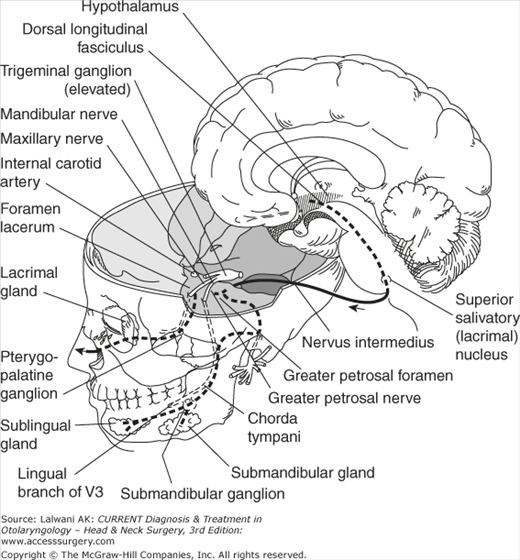
The anatomy of the visceral motor portion of the facial nerve, making up the nervus intermedius, or Wrisberg nerve. The preganglionic, parasympathetic portions of this nerve have cell bodies located in the abducens nucleus. From there they travel toward the geniculate ganglion in the temporal bone, located at the first genu of the facial nerve on the floor of the middle cranial fossa. Fibers from this nerve are destined to innervate the lacrimal gland, the minor salivary glands, and the mucosal glands of the palate and nose. (Reproduced with permission from Wilson-Pauwels L, Akesson EJ, Stewart PA, Cranial Nerves: Anatomy and Clinical Comments. B.C. Decker Inc.: Toronto; 1988.)
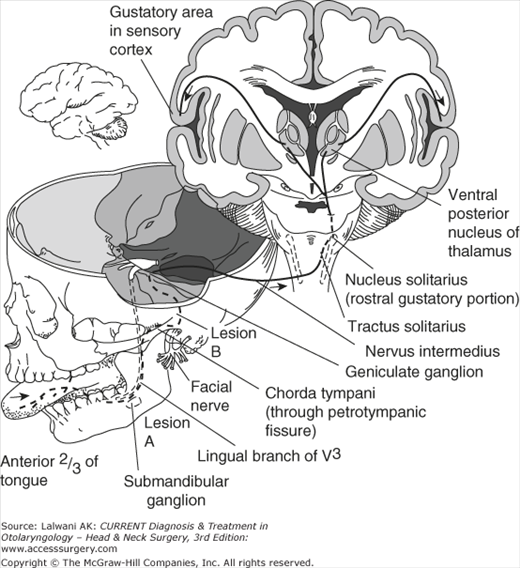
The special visceral afferent fibers, which also form a portion of the chorda tympani nerve, receive input from the taste buds of the anterior two-thirds of the tongue, as well as the hard and soft palates (Figure 69–6). These sensory afferents for taste have their cell bodies in the geniculate ganglion and will eventually synapse in the medulla, in the nucleus solitarius.
The general sensory afferent neurons of the nervus intermedius are responsible for cutaneous sensory information from the external ear canal and postauricular region. These cutaneous sensory fibers enter the spinal trigeminal tracts without synapsing in the geniculate ganglion.
The facial nerve leaves the brainstem at the pontomedullary junction (see Figure 69–4). At this location, it lies in close approximation to the eighth cranial nerve (the vestibulocochlear nerve). This intimate relationship takes on critical importance when disease, most commonly a vestibular schwannoma, arises in the region of the cerebellopontine angle. In this location, the facial nerve is placed in jeopardy both during the growth of the tumor and during attempted surgical resection in this area.
During its lateral course through the cerebellopontine angle and internal auditory canal (IAC), the relative positions of the facial and cochleovestibular nerves change by rotating 90°. In the cerebellopontine angle, the facial nerve is covered with pia, bathed in cerebrospinal fluid, and is devoid of epineurium. As a result, the nerve is very susceptible to trauma or manipulation in this region, such as during intracranial surgery.
After traversing the cerebellopontine angle, the facial nerve enters the temporal bone along the posterior face of the petrous bone. Within the temporal bone, the facial nerve successively passes through 4 regions prior to its exit out of the stylomastoid foramen: (1) the IAC, (2) the labyrinthine segment, (3) the intratympanic segment, and (4) the descending segment (Figures 69–7, 69-8, and Figure 69–9). From the lateral end of the IAC to its exit out the stylomastoid foramen, the nerve travels approximately 3 cm within the facial canal, also known as the fallopian canal.
Figure 69–7.
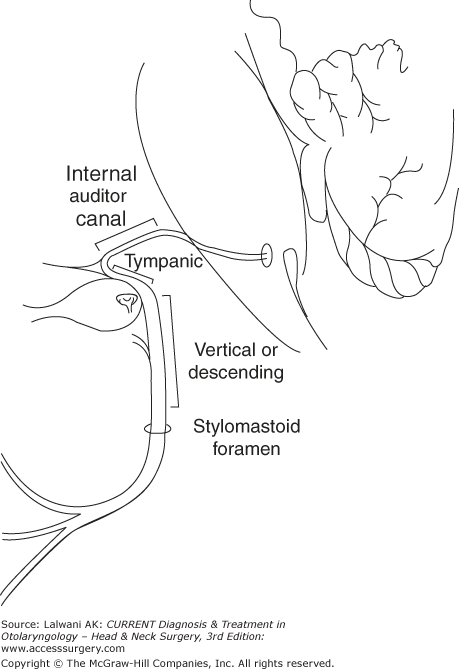
The intratemporal divisions of the facial nerve. After passing through the internal auditory meatus on the posterior face of the petrous temporal bone, the nerve enters its canalicular segment, within the IAC. It then becomes the labyrinthine segment, as it traverses between the cochlea and the vestibular labyrinth. After making its first genu (bend) at the geniculate ganglion, it becomes the tympanic segment, coursing through the middle ear space, just superior to the oval window. It then makes its second major genu at the level of the horizontal semicircular canal and becomes the vertical or descending segment. After passing through the stylomastoid foramen, it becomes extracranial.
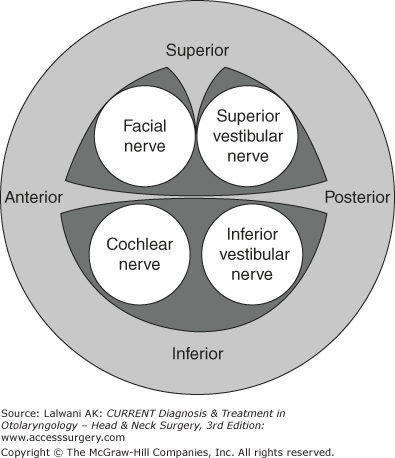
Figure 69–9.
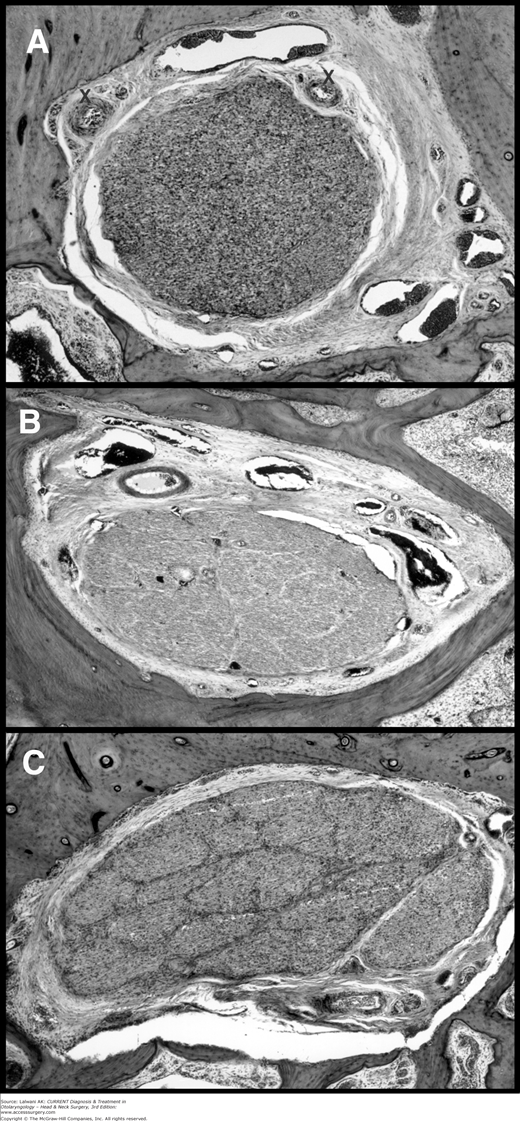
Histological cross sections of the facial nerve at 3 points along its course within the temporal bone. Proximally within the temporal bone at the level of the internal auditory canal, (A) the individual nerve fascicles are not defined and nerve elements appear homogenous. (B) As the nerve proceeds through the tympanic segment and (C) at the level of the stylomastoid foramen, individual nerve fascicles becomes increasingly defined.
After traversing the cerebellopontine angle, the facial nerve enters the temporal bone along the posterior face of the petrous bone, piercing the internal auditory meatus. At the lateral end of the IAC, a ridge of bone, the traverse crest, divides the IAC into superior and inferior portions. It is at this lateral portion of the IAC that the anatomy is most consistent: the superior portion is occupied by the facial nerve anteriorly and the superior vestibular nerve posteriorly (see Figure 69–8). These two nerves are additionally divided by a bony ridge, the vertical crest or “Bill’s bar.” The inferior portion of the IAC, below the transverse crest, contains the cochlear nerve (anterior) and the inferior vestibular nerve (posterior). Within the IAC, the dural covering of the facial nerve is transformed to epineurium.
At the lateral portion of the IAC, the facial nerve pierces the meatal foramen to enter the labyrinthine segment. The labyrinthine segment is notable in that it is the narrowest portion of the fallopian canal, where it averages <0.7 mm in diameter and occupies the canal to the greatest proportional extent. As a result, it is believed that infections or inflammations of the facial nerve within this region can lead to temporary or permanent paralysis of the nerve, such as in Bell’s palsy.
The distal end of the geniculate ganglion is considered the end of the labyrinthine segment of the nerve and lies just superior to the nerve. While it is generally bone-covered just below the floor of the middle cranial fossa, the geniculate ganglion is dehiscent into the middle fossa up to 15% of the time. Arising from the geniculate ganglion is the greater superficial petrosal nerve.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


