Chapter 154 Miscellaneous Uveal Tumors
Epithelial tumors of the ciliary body: congenital
Medulloepithelioma
Medulloepithelioma (diktyoma, teratoneuroma) is a congenital tumor that is generally believed to arise from the epithelium of the medullary tube. This tumor usually arises from the ciliary body epithelium, but medulloepitheliomas of the retina and the optic nerve also occur. The first detailed histologic description of the tumor was by Verhoeff,1 who called it a teratoneuroma, despite the absence of teratomatous features. Fuchs2 reported his observations of a medulloepithelioma and coined the term diktyoma because of the netlike appearance of cells composing the tumor. Grinker3 was the first to use the term “medulloepithelioma,” which has become the preferred name because it refers to the correct cell of origin.
Three large series of medulloepitheliomas have been reported4–6 and provide the bulk of our knowledge of the clinical features of this tumor. In Broughton and Zimmerman’s series,5 the median age at occurrence of initial symptoms was 3.8 years, with a range of 6 months to 41 years. Andersen4 reported that the average age at the time of enucleation was 4.5 years for benign medulloepitheliomas and 7 years for malignant tumors. In the series of Canning et al.6 the median age at diagnosis was 3 years. In all three series, all tumors were unilateral and single, and there was no racial or hereditary predisposition.
The signs and symptoms of the 56 patients reported on by Broughton and Zimmerman5 are summarized in Tables 154.1 and 154.2.
Table 154.1 Medulloepithelioma – symptoms and signs
| Clinical finding | Cases (n) |
|---|---|
| Poor vision (or blindness) | 22 |
| Pain | 17 |
| Mass in iris or ciliary body | 10 |
| Leukocoria | 10 |
| Other pupillary abnormality | 2 |
| Exophthalmos (or orbital mass) | 4 |
| Enlarging globe | 4 |
| Strabismus | 3 |
| Epiphora | 2 |
| Change in color of eye | 2 |
| Hyphema | 1 |
(Reproduced with permission from Broughton WL, Zimmerman LE. A clinicopathologic study of 56 cases of intraocular medulloepitheliomas. Am J Ophthalmol 1978;85:407–18.)
Table 154.2 Medulloepithelioma – clinical findings on initial examination
| Clinical finding | Cases (n) |
|---|---|
| Cyst or mass in iris, anterior chamber, or ciliary body | 30 |
| Proptosis or orbital mass | 8 |
| Retinal mass | 2 |
| Glaucoma | 26 |
| Cataract | 14 |
| Buphthalmos | 6 |
| Iritis | 4 |
| Rubeosis | 3 |
| Retinal detachment | 3 |
| Strabismus | 3 |
| Vitreous hemorrhage | 1 |
| Hyphema | 1 |
(Reproduced with permission from Broughton WL, Zimmerman LE. A clinicopathologic study of 56 cases of intraocular medulloepitheliomas. Am J Ophthalmol 1978;85:407–18.)
One remarkable feature of medulloepitheliomas is the frequent presence of cysts, which are formed by the production of mucopolysaccharide by the epithelial cells. These cysts can be present within the body of the tumor but also may be free-floating in the anterior or posterior chamber and vitreous (Figs 154.1–154.4). The presence of vitreous or anterior chamber cysts should alert the clinician to consider the possibility of a diagnosis of medulloepithelioma, although vitreous cysts have also been described with malignant melanoma.7

Fig. 154.1 External photograph showing ciliary body mass.
(Case presented by Milton Boniuk, Verhoeff Society, 1997.)
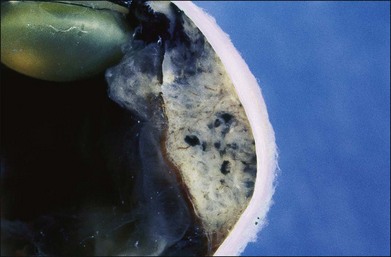
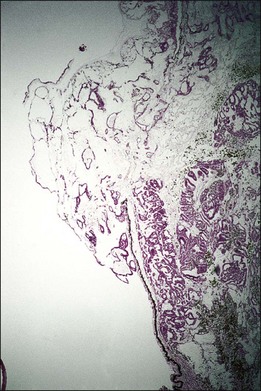
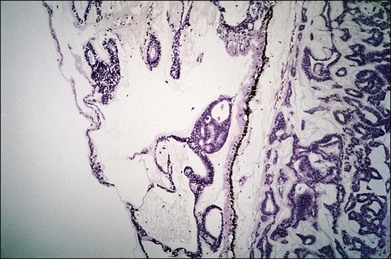
Fig. 154.4 Histopathology demonstrating cystic spaces overlying ciliary body epithelium. (H&E; ×400.)
Another noteworthy feature of medulloepithelioma is that the intraocular pressure is frequently elevated at the time of diagnosis (see Table 154.2). This may result from secondary angle closure by the ciliary body mass, iris neovascularization, or growth of tumor cells across the trabecular meshwork.
Medulloepitheliomas may be benign or malignant. Broughton and Zimmerman5 considered 66% of the tumors in their series to be malignant. Andersen,4 using more stringent criteria, classified 26% of the tumors in his series as malignant. From a practical point of view, even cytologically benign medulloepitheliomas can be locally invasive, extending into the iris, cornea, sclera, or orbit. For that reason all medulloepitheliomas should be considered as potentially malignant tumors, as recommended by Andersen.4
The initial treatment in all reported cases has been surgical – iridectomy, iridocyclectomy, or enucleation – and with total excision, the prognosis is excellent. Canning et al.6 have stressed the importance of attempting local resection (i.e., iridocyclectomy) only in patients with very small tumors. Of the four patients in their series who were treated by iridocyclectomy, all subsequently required enucleation. A total of 45 (80%) of the patients in Broughton and Zimmerman’s series5 treated by iridocyclectomy subsequently required enucleation.
In both Broughton and Zimmerman’s5 and Anderson’s4 series of patients, the most important prognostic factor appeared to be extension of tumor into the orbit. In Broughton and Zimmerman’s series,5 11 patients had extraocular extension; of this group, four died of tumor-related causes. Intracranial spread of tumor was the usual cause of death, although one patient died of lymphatic spread to the mediastinum. The effectiveness of exenteration, radiation therapy, or chemotherapy – used individually or in combination – in managing extraocular extension is not established at this time. Such methods should be considered in cases with extrascleral extension because of the high tumor-related morbidity and mortality in this group of patients.
Glioneuroma
Glioneuromas are choristomatous malformations that arise from the medullary epithelium of the anterior portion of the optic cup. They are extremely rare, and only a few cases have been reported.8–12
These tumors are composed of well-differentiated neural tissue, including neurons and astrocytes. All the reported cases8–12 have eventually required enucleation because of complications of the enlarging tumor or suspected malignancy. Because this is a benign tumor, it could conceivably be managed by local resection.
Astrocytoma
Only two cases of astrocytoma of the ciliary body have been reported.13,14 One patient was 24 years old, and the other was 52 years old. At presentation, both had solid tumors of the ciliary body, and in one patient the astrocytoma was associated with neovascular glaucoma. Growth of the tumor was not documented in either case. These tumors were probably choristomas of the anterior portion of the optic cup. Both lesions consisted of pilocytic astrocytes. Both tumors were treated by iridocyclectomy. Interestingly, in the patient with neovascular glaucoma, the rubeosis was observed to diminish after removal of the tumor.
Epithelial tumors of the ciliary body: acquired
Senile hyperplasia
Senile hyperplasia (Fuchs adenoma) is a benign tumor. The frequency with which it is seen increases with age; this tumor may be observed in approximately 20% of postmortem eyes. Because these tumors are almost always <2 mm in size, they are usually of no clinical significance. However, they may cause a sectorial cataract15 and have been removed because of clinical suspicion of malignancy.15,16
Adenomas and adenocarcinomas
Adenomas and adenocarcinomas have been described by various names, including benign and malignant epitheliomas and adult medulloepitheliomas. Adenomas and adenocarcinomas of the ciliary epithelium appear as solid tumors of the ciliary body. In Andersen’s review of 30 of these cases, the presenting symptom was an observed mass in nine cases and decreased visual acuity in eight cases.4 Other manifestations included glaucoma, cataract, pain, and proptosis. The average age of the patients with adenomas at the time of enucleation was 43 years. For the patients with adenocarcinomas, the average age at the time of enucleation was 55 years. It is noteworthy that several of the reported adenocarcinomas were present in blind eyes involving a previous history of trauma, suggesting that the adenocarcinomas may have represented malignant transformation of reactive hyperplasia of the ciliary epithelium.
The pathologic basis of these tumors has been more thoroughly described elsewhere.7 Briefly, the adenomas consist of cuboidal or columnar cells resembling the nonpigmented or pigmented ciliary epithelium. These cells may have a tubular or papillary arrangement and may be closely packed or enmeshed in a mucoid material.
Because these lesions cannot be reliably differentiated from melanomas, they are usually treated by enucleation or brachytherapy. It is evident that extraocular extension is an important factor in prognosis. Andersen reported two cases of adenocarcinoma that had extended outside the globe at the time of enucleation.4 Both of the patients developed intracranial extension of the tumor. In another series of 21 cases of adenocarcinoma of the ciliary epithelium, follow-up information was available for 16 patients.17 Of those 16 patients, five died of tumor extension into the central nervous system or of widespread metastatic disease; four of the five patients had extraocular extension at the time of initial surgery. The role of exenteration, radiation therapy, or chemotherapy in extraocular extension has not been defined.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


