Chapter 6 Milestones and normative data
Intercanthal distance and palpebra
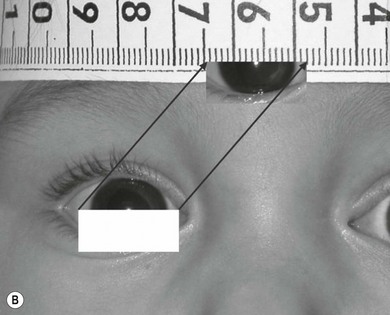
Abnormalities in the distance between the inner canthi and the outer canthi and the size and shape of the palpebral fissure are important features in craniofacial malformations and fetal alcohol syndrome. A fast non-contact method of measuring facial components is provided in Fig. 6.1A,B.1

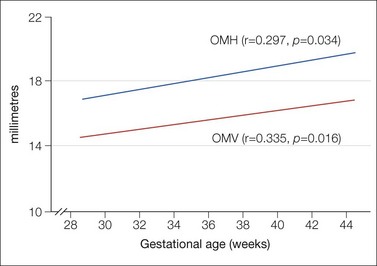
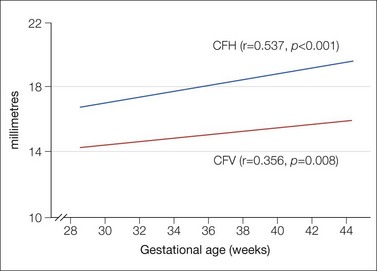
Palpebral fissure changes in early childhood have been studied by analyzing digital imaging:2 during the first 3 months of life the upper eyelid is at its lowest position, later rising to its maximum between the age of 3 to 6 months, and then declining until adulthood. The lower eyelid is close to the pupil center at birth, dropping until the age of 18 months when its position stabilizes. A single lower eyelid crease is common at birth, a double crease at the age of 36 months. Figure 6.2 shows the linear relationship between gestational age and orbital margin horizontal (OMH), as well as vertical (OMV) diameters in the unborn child.3 There is a linear relationship between gestational age and conjunctival fornix horizontal (CFH) and conjunctival fornix vertical (CFV) diameters (Fig. 6.3).3
The palpebral fissures are 15 ± 2 mm at 32 weeks of gestation, 17 ± 2 mm at birth, 24 ± 3 mm at 2 years of age, and 27 ± 3 mm at the age of 14.4,5 Inter-racial differences exist: the palpebral fissure is longer in Black Americans.6
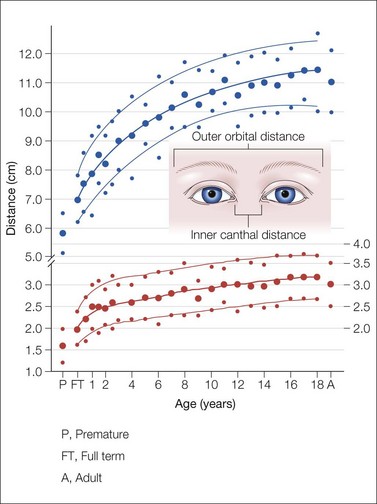
Inner canthal distance and outer orbital distance are 16 and 59 mm, respectively, in premature infants; 20 ± 4 and 69 ± 8 mm in newborn babies; 26 ± 6 and 88 ± 10 mm at the age of 3; and 31 ± 5 and 111 ± 12 mm at the age of 14 (Fig. 6.4).7
A universal approach is the canthus index:

Normals, unrelated to age, lie between 28.4 and 38%.8 The canthus index of over 1000 children between 6 and 18 years old was determined as follows:9
| Boys | Girls | |
|---|---|---|
| 6 years | 38.2% (SD 2.1%) | 38.3% (SD 1.8%) |
| 16 years | 37.1% (SD 2.6%) | 36.6% (SD 1.9%) |
Tear secretion
Tearing is not a problem when holding open the eyelids on the youngest premature babies. Later, in preterm babies (30–37 weeks after conception) mean basal tear (with topical anesthesia) secretion is 6.2 (± 4.5 SD) mm and at term 9.2 (± 4.3) mm tested with a Schirmer tear test strip. Mean reflex tear secretion is 7.4 (± 4.8) mm in preterm and 13.2 (± 6.5) mm in term infants.10
Cornea
The premature cornea lacks luster and clarity, making some diagnoses difficult. Shallow anterior chambers, miotic pupils, and bluish irides are features of prematurity. The corneal diameter in infants at 25–37 weeks postconceptional age increases by 0.5 mm every 15 days from 6.2 to 9.0 mm (Fig. 6.5).11,12 The horizontal and vertical diameters of the cornea in full-term boys are 9.8 ± 0.33 mm and 10.4 ± 0.35 mm and in girls 10.1 ± 0.33 mm and 10.7 ± 0.29 mm.13 Two millimeters of growth in corneal diameter (approximately 20%) occurs in early infancy and early childhood. An adult value of 11.7 mm is reached by 7 years.
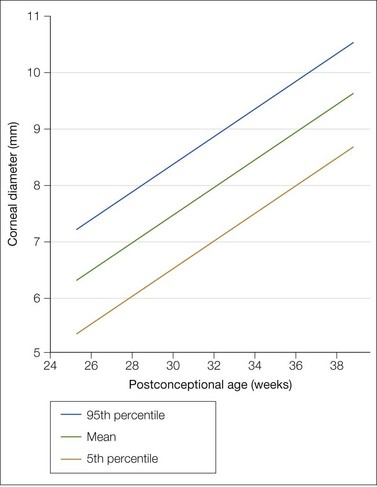
Fig. 6.5 Mean corneal diameter plotted against postconceptional age.
From Tucker SM, Enzenauer RW, Levin AV, et al. Corneal diameter, axial length, and intraocular pressure in premature infants. Ophthalmology 1992; 99: 1296–300.11 With permission from American Academy of Ophthalmology.
Central corneal thickness
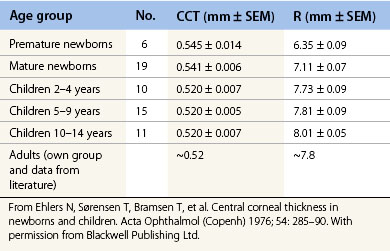
Abnormal thickness of the central cornea influences intraocular pressure, but also corneal hysteresis may play a role in children. Central corneal thickness (CCT) in a full-term baby is 0.54 mm greater than in a 1-year-old child. CCTs measured with optical pachymetry and corneal curvature are given for premature and full-term babies in Table 6.1.14
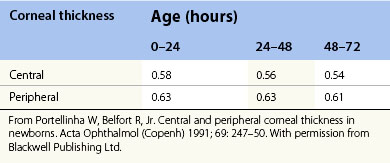
CCT in premature infants below 33 weeks gives a mean of 0.656 mm (SD ± 0.103 mm) 5 days postnatally and 0.566 (SD ± 0.064) at the age of 110 days.15 In full-term neonates,16 CCT is 0.573 ± 0.052 mm (range 0.450–0.691 mm) with a peripheral corneal thickness of 0.650 ± 0.062 mm (range 0.520–0.830 mm). Table 6.2 shows the decrease in thickness during the first few days of life.
Another study17 confirmed the above data and also measured peripheral corneal thickness: superior corneal thickness was 0.696 ± 0.055 mm, inferior was 0.744 ± 0.062 mm, nasal was 0.742 ± 0.058 mm, and temporal was 0.748 ± 0.055 mm. Adult values are reached at about 3 years of age. There is no significant difference of CCT among racial subgroups.18
Pupil size and reaction to light
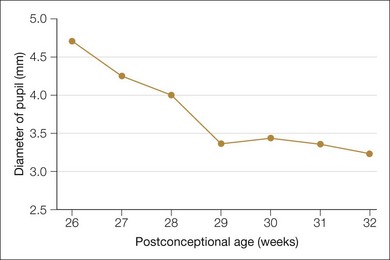
The pupil, in relative darkness, has a mean diameter of 4.7 mm at 26 weeks postconceptional age. The pupils subsequently become progressively smaller, reaching 3.4 mm at 29 weeks. There is no reaction to light until 30.6 weeks (± 1 week) postconceptional age.19 Figure 6.6 shows the change of pupil diameter in relative darkness (< 10 ft-c) in preterm neonates. The mean pupil size is 3.8 mm (SD ± 0.8 mm) in the newborn period. The incidence of anisocoria of less than 1 mm is 21%; no difference was greater than 1 mm.20
Pars plana and ora serrata
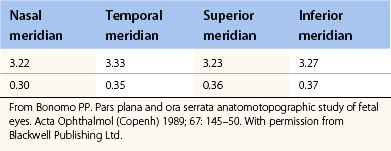
The average pars plana of third trimester fetuses is 1.17 mm in width, which is one-third of that in the adult eye. The distance between the sclerocorneal limbus and the ora serrata is 3.22 mm nasally and 3.33 mm temporally (Table 6.3).21 Similar figures were obtained from examination of 76 paraffin-embedded normal eyes from 1-week-old to 6-year-old children.22
Table 6.3 Values (mm) of the distance from sclerocorneal limbus to the ora serrata in the nasal, temporal, superior, and inferior meridians (mean ± SD) in fetuses aged 24–40 weeks20
Optic disc parameters
The diagnosis of optic nerve hypoplasia is a subjective one because it is not only optic nerve size that is important. The optic disc dimensions of 66 children of low refraction error aged 2–10 years was studied by fundus photography (Table 6.4A).23
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


