Migraine and Other Headaches
B. Todd Troost
When you’re lying awake
With a dismal headache
And repose is taboo’d by anxiety,
I conceive you may use
Any language you choose
To indulge in without impropriety.
“Iolanthe” by W.S. Gilbert
A headache, in a variety of forms, is one of the most common complaints presented to the clinician. A new classification of headache has been proposed by the International Headache Society (IHS) and is summarized in Table 1.1 This chapter addresses the neuro-ophthalmologic aspects of migraines and provides a brief review of other common headaches, facial and ocular pains.
A Migraine is a periodic and paroxysmal protean disorder that affects more than 17% of women and 6% of men in the United States.2,3 It is estimated that the lifetime prevalence of migraine in women is 99% and the lifetime prevalence in men is 93%.4 Neuro-ophthalmologic symptoms and signs are common in migraines and should be recognized by the clinician. The term hemicrania evolved from a variety of older descriptions and was one of the first names for this disorder; this was later contracted by the French in the thirteen century to the word “migraine.” More than 300 years ago, Thomas Willis wrote the first modern description of a migraine and its possible causes. Historical figures believed to have had migraines include Julius Caesar, Emmanuel Kant, Alexander Pope, Isaac Newton, and Sigmund Freud. Throughout the eighteenth and nineteenth centuries, descriptions of the clinical phenomena and suggestions for therapy continued to appear in the writings of many prominent men in the medical professions. Sacks5 pays homage to Edward’s masterful treatise On Megrim, Sick Headache, and Some Allied Disorders (1873) as an unequaled description of the disorder. Further detailed clinical descriptions are found in the writings of Gowers.6
In contemporary medicine, Dalessio, Goadsby, Raskin, Sacks, Silberstein, Lipton, Stewart, Saper, and Welch are among those who could be singled out for their contributions to the study of migraines. One central theme seems to decry the simplistic view that a migraine is defined by a unilateral (hemicranial) headache. As Sacks5 wrote, “It is necessary to state that headache is never the sole symptom of a migraine, nor indeed is it the necessary feature of migraine attacks.” Another quote emphasizes this belief: “Migraine is diagnosed by the entire history, not by physical findings or by the presence of headache alone.”7 It is unfortunate that many have limited their concept of migraine to a stereotyped syndrome of visual disturbance followed by unilateral throbbing headache, which is diagnosed by the response to ergot preparations. Migraine gives rise to a number of well-recognized syndromes, as well as a variety of “equivalents” less commonly considered as migraine. The symptom-complexes or syndromes of migraine include migraine without aura, migraine with aura, ophthalmoplegic migraine, retinal migraine, as well as the others listed in Table 1. The clinical features of migraine will be discussed according to the formal criteria published by the IHS in 2004.1
Other conditions and syndromes discussed include cluster headache, trigeminal neuralgia, atypical facial pain, temporal arteritis, and the headaches produced by intracranial mass lesions, muscle contraction, trauma, vascular anomalies, and ocular lesions.
TABLE 1. New International Headache Society Classifications of Headaches | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
DESCRIPTION OF THE MIGRAINE ATTACK
Blau8 has divided the migraine attack into five phases: the prodrome, occurring hours or days before the headache; the aura, which come immediately before the headache; the headache itself; the headache termination; and the postdrome. As pointed out by Silberstein and Lipton,9 “Although most people experience more than one phase, no one particular phase is required for the diagnosis of migraine.” These authors provide a description of the five phases, which reviews the initial manifestations of migraine.
PRODROME
Premonitory phenomena occur in approximately 60% of migraineurs, often hours to days before the onset of headache. These phenomena include psychologic, neurologic, constitutional, and autonomic features. Psychologic symptoms include depression, euphoria, irritability, restlessness, mental slowness, hyperactivity, fatigue, and drowsiness. Neurologic phenomena include photophobia, phonophobia, and hyperosmia. The generalized or constitutional symptoms include a stiff neck, a cold feeling, sluggishness, increased thirst, increased urination, anorexia, diarrhea, constipation, fluid retention, and food cravings. Some patients just report a poorly characterized premonition that a migraine attack is coming.
AURA
An aura refers to the appearance of focal neurologic symptoms that proceed or even accompany an attack of migraine. Approximately 20% of migraine sufferers experience auras. Most aura symptoms develop over a course of 5 to 20 minutes and usually last less than 60 minutes. The aura can be characterized by visual, sensory, or motor phenomena, and may also involve language or brainstem disturbances. When a headache follows, it most often occurs within 60 minutes of the end of the aura. The appearance of isolated auras without headache is known as migraine dissociée. The most common aura is visual, previously termed classic migraine. It usually has a distribution in the right or left homonymous hemifields.
Sensory disturbances involve one side of the body and are characterized by descriptions of numbness or tingling on the face and in the hand. Further neurologic symptomatology is discussed under the heading of migraine with prolonged aura and migrainous infarction.
HEADACHE PHASE
The typical migraine headache is unilateral and throbbing. It may be bilateral and constant at first and later become throbbing. As pointed out by Lipton and Stewart,10 pain is characterized as throbbing in 85% of patients. However, it should be noted that a throbbing headache is described in other types of headache.11 The pain of migraine is almost always accompanied by other features such as anorexia. Nausea occurs in up to 90% of patients and vomiting occurs in approximately one-third of migraineurs.10
Many patients experience photophobia, phonophobia, and osmophobia, and seek seclusion in a dark, quiet room. Additional generalized symptoms include blurry vision, nasal stuffiness, anorexia, hunger, tenesmus, diarrhea, abdominal cramps, polyuria (followed by decreased urinary output after the attack), facial pallor (or, less commonly, redness), sensations of heat or cold, and sweating.9 Localized edema of the scalp, the face, or the periorbital regions may occur; tenderness may occur and be particularly prominent. There may also be tenderness of the scalp, a special prominence of a vein or artery in the temple, or a stiffness or tenderness of the neck. Impaired concentration is common; memory impairment occurs less frequently. Depression, fatigue, anxiety, nervousness, and irritability are common. A sensation of faintness may be experienced. The IHS selects particular associated features as cardinal manifestations for diagnosis.
TERMINATION AND POSTDROME
In the termination phase, the pain diminishes. Thereafter the patient may be listless, tired, or “washed out” and not feel well for 24 to 48 hours. Rarely patients feel unusually refreshed or euphoric after an attack, whereas it is more common to note depression and malaise.9
PATHOPHYSIOLOGY
Although there is some understanding of the mechanism of migraine, its precise underlying causes are unknown. Extensive reviews and volumes have been published on the pathophysiology of headaches and, in particular, of migraines.12,13,14,15
According to Goadsby et al.,16,17 a migraine is best understood as a primary disorder of the brain. A migraine is a polygenetic disorder believed to have a primary problem in the abnormal function of an ion channel in the brain-stem nuclei that modulates sensory input.17 Specific gene abnormalities have been found in patients with familial hemiplegic migraine, that is a missense mutation in the α1 subunit of the voltage-gated P/Q-type calcium channels.18 As pointed out by Goadsby,16 it is likely that the aura of migraine is separate from the headache as cases of migraine with aura have been linked to the familial-hemiplegic-migraine locus.19
GENETICS IN MIGRAINE
Migraines frequently run in families, suggesting that hereditary factors are clearly involved.20,21 Familial hemiplegic migraine, a rare subtype of migraine, is inherited as an autosomal dominant pattern or with sporadic inheritance. Familial hemiplegic migraine is caused by mutations in specific genes. The first gene identified was the CACNA1A gene located on the chromosome 19p13 which coded for the pore-forming subunit Cav2.1 of P/Q-type sodium channels. This gene is found in approximately 75% of such findings. This would define this type of migraine as a “channelopathy.” It has also been suggested that migraine with aura has a loci on chromosome 4Q.22
It was primarily through the work of Wolff and colleagues15 that vascular phenomenon were recognized as a mechanism responsible for the headache of migraine. Research to date suggests that the initiation of a migraine attack is primarily a neuronal phenomenon with secondary hemodynamic consequences.17,23,24,25,26 Wolff divided the migraine attack into four phases: preheadache, headache, late headache, and postheadache. The preheadache phase is characterized by the constriction of certain blood vessels that supply the brain. Then, the beginning of the headache phase is characterized by vascular dilatation, particularly involving branches of the external carotid such as the temporal, occipital, and middle meningeal arteries. Local tenderness of the scalp ensues, and the scalp vessels may become rigid. The nature of the headache then changes from a pulsatile type to a more constant dull ache. Alleviation of the early headache phase with vasoconstrictors (e.g., ergotamine) is cited as evidence that this pain is related to vasodilatation. In their most simplistic form these concepts can be reduced to the idea that the cerebral symptomatology, including the auras of classic migraine, is the result of cerebral ischemia secondary to intracranial vessel spasm, and the ensuing headache phase is initiated by vasodilatation. However, vasodilatation may occur without pain, and additional factors are involved in the production of the headache. Local tissue changes take place (e.g., vessel edema, scalp swelling, and conjunctival chemosis) that may continue after vasodilatation has ceased. A wide variety of substances have causative roles in the production of large and small vessel dilatation as well as local tissue changes. Among the substances most frequently considered are the kinins (neurokinin and bradykinin), acetylcholine, histamine, serotonin, and reserpine. Migraine, then, may result from dysfunction of brain stem or diencephalic nuclei involved in nocieceptive modulation of afferents from the trigeminal vascular system.16 Positron emission tomography has detected activation in the brain stem during attacks of migraine.27,28
Sicuteri et al.29 hypothesized that the following sequence occurs: the initial event is a local release of catecholamines (with vasoconstriction and increased urinary excretion of vanillylmandelic acid); during subsequent reactive hyperemia serotonin is released (documented by plasma serotonin decrease30 and increased urinary 5-hydroxy indoleacetic acid31), presumably from platelets or mast cells, which sensitizes cranial pain receptors perhaps also affected by the kinins. Additional evidence suggests that there are nervous system connections between the trigeminal ganglia and cerebral blood vessels, termed the trigeminovascular system.32 Trigeminovascular neurons and their peripheral unmyelinated nerve fibers contain the neurotransmitter peptide, substance P. Stimulation of this system by a variety of mechanisms would cause the release of substance P, which is postulated to increase vascular permeability and dilate cerebral blood vessels. The role of this system in the generation of human vascular headache may account for the effects of hormones or other circulating substances that change the receptive field properties of trigeminal ganglion cells. Individuals prone to chemically induced headaches from ingestion of tyramine, alcohol, phenylethyamine, monosodium glutamate, nitroglycerine, wine, or chocolate also experience spontaneous headaches.33 Extensive studies of the reactivity of blood vessels in migraine34 and cerebral blood flow24,25,35,36 suggest that abnormal vasomotor responses may be present in patients with migraine between, as well as during, migraine attacks.
There are several lines of indirect evidence that suggest a relationship between serotonin and migraine, making the understanding of the pharmacology of serotonin important for understanding the pharmacology of the new serotonin agonist in migraine therapy.9 The serotonin or 5-HT receptors consist of at least three distinct types of molecular structures: guanine nucleotide G protein-coupled receptors, ligand-gated ion channels, and transporters. At least five 5-HT1 receptor subtypes are present in humans. Headaches resembling migraine can be triggered by serotonergic drugs such as reserpine (a 5-HT releaser and depleter) and m-chlorophenylpiperazine (a serotonin agonist).37,38
Other metabolic and endocrine factors also influence migraine attacks. According to Friedman and Merritt,39 80% of pregnant women previously prone to migraines either lose the headaches or experience improvement. Callaghan,40 however, found an increase in the severity of migraine in pregnancy. The use of oral contraceptives appears to increase the incidence and severity of migraine.41,42 Whitty43 felt that migraine might be precipitated by withdrawal of progesterone, while Somerville44 found from a study of three women with regular menstrual migraine that their attacks were related to estradiol withdrawal rather than to decreasing levels of progesterone. Tyramine has also been invoked as a precipitating factor, especially in the so-called allergic migraine,45 however, only approximately 5% of migraine subjects notice headaches precipitated by food. Some patients, however, are unusually sensitive to chocolate or alcohol, particularly red wines. Recent therapeutic trials with dietary therapy designed to avoid hypoglycemia suggest that glucose and/or insulin metabolism may play a role in the generation of vascular headache.
The role of trauma in the production or exacerbation of a preexisting migrainous tendency is still incompletely defined. Many individuals experience vascular headaches of the common migraine type after even minor head trauma.46 A previously well-controlled migraineur can experience a recrudescence of prior symptomatology after a head trauma. Such exacerbations are usually short-lived with a return to the preinjury status in weeks to a few months. However, there are some patients who experience posttraumatic migraine headaches for years after a head injury. Other triggering events preceeding migraine attacks include bright light, especially sunlight reflected from water, exercise or exertion, and high altitude. Vascular headache of the migraine type may also follow orgasm.47 The role of stress is less clear. It appears more likely that migraine headache follows a period of psychologic stress than occurring during the time of stress.
The pathophysiology of the migraine aura itself also has been studied extensively. Wolff showed that the use of a potent vasodilator, amylnitrate, could abort the migraine scotoma (Fig. 1), supporting the vasoconstrictor hypothesis. Milner48 suggested that the scotomas of migraine and the neurophysiologic phenomenon, Leão’s spreading depression, may be related. The spreading depression progresses across the cortex at approximately 3 mm/min, similar to the slow evolution of the visual phenomenon that had been detailed by Lashley,49 and estimated to spread over the occipital cortex at a rate of 3 mm/min.
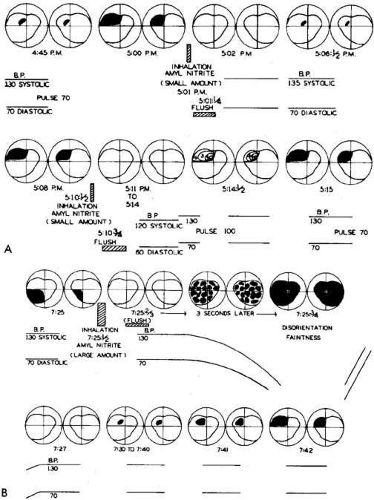 Fig. 1 A. Effect of inhalation of small amount of amyl nitrite on preheadache scotomas in migraine subject. The amount was insufficient to cause a drop in blood pressure or “light-headedness.” B. With inhalation of a large amount of amyl nitrite, a drop in pressure occurred with amblyopia and faintness. (Wolff HG: Headache and Other Head Pain, 2nd ed. New York: Oxford University Press, 1963) |
It is currently believed that the aura of migraine may be the human counterpart of the animal phenomenon of Leão’s spreading depression.50 The aura is characterized by a wave of decreased blood flow or oligemia passing across the cortex24,51,52,53 at a slow rate (2 to 6 mm/min) consistent with the spread of the visual phenomenon through the visual cortex, as mentioned above.54 There is a short phase of hyperemia preceding the oligemia that may be a correlate of the scintillating scatoma, also a characteristic of migraine with aura.55 However, persistent oligemia is probably a response to depressed neuronal function and is present when the headache starts, as noted by Goadsby.16,53,56 Such findings coupled with the direct evidence of adequate local oxygen supply57 vitiate the theory that migraine is just a vascular headache.16
Three cardinal factors are important in the pathogenesis of migraine, according to Goadsby.16 These include the cranial blood vessels, the trigeminal innervation of these vessels, and the reflex connection of the trigeminal system with a cranial parasympathetic outflow. The pain sensitive structures within the cranium, such as large blood vessels or the dura mater, are innervated by branches of the ophthalmic division of the trigeminal nerve58 and the posterior fossa structures are innervated by branches of C2 nerve roots.59 As indicated by Goadsby,16 involvement of the ophthalmic division of the trigeminal nerve and the overlap with structures innervated by C2 explain the common distribution of the pain of migraine in the frontal and temporal regions, as well as involvement of parietal occipital and high cervical regions, by referred pain. Peripherally, the trigeminal afferents are activated in migraine by the release of calcitonin gene-related peptide (CGRP) a vasodilator,60 and while the mechanism of pain generation is not entirely clear, animal studies suggest that pain is caused by a sterile neurogenic inflammation in the dura mater.61 This may, in part, explain the prevention of migraine pain by substances such as botulinum toxin type A, which inhibit the release of CGRP.62 As stated by Goadsby,16 the pain may be a combination of an altered perception—as a result of peripheral or central sensitization—of craniovascular input that is not usually painful63 and the activation of feed-forward neurovascular dialator mechanism that is functioning specific to the first ophthalmic division of the trigeminal nerve.64 Again, the effect of botulinum toxin type A in reducing migraine pain may interfere with this peripheral activation and, therefore, function to provide peripheral desensitization.62
MIGRAINE WITHOUT AURA
The IHS classification has improved the diagnosis of headaches. It has also facilitated clinical research on migraine. In order to establish a diagnosis of migraine without aura, five attacks are needed (Table 2). Each attack must last 4 to 72 hours and have two of the following four pain characteristics: unilateral location, pulsating quality, moderate to severe intensity, and aggravation by routine physical activity. In addition, the attacks must be associated with at least one of the following: nausea, vomiting, or photophobia and phonophobia. With these criteria, no single characteristic is mandatory for a diagnosis of migraine. A patient who has severe pain aggravated by routine activity, photophobia and phonophobia, meets these criteria as does the more typical patient with unilateral throbbing pain and nausea.
TABLE 2. Migraine Without Aura | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Migraine usually lasts several hours or the entire day. When the migraine persists for longer than 3 days, the term “status migrainosis” is used. Frequency of attacks varies widely from a few per lifetime to several per week.9 The average migraineur experiences from one to three headaches per month.3 A precise location ascribed to migraine, such as unilateral or temporal, is misleading, for as Wolff34 wrote:
The sites of migraine are notably temporal, supraorbital, frontal, retrobulbar, parietal, postauricular, and occipital… They may as well occur in the malar region, in the upper and lower teeth, at the base of the nose, in the median wall of the orbit, in the neck, and in the region of the common carotid arteries and down as far as the tip of the shoulder.
The prodromes of common migraine are vague, preceding the attack by hours or days, and include psychic disturbances (such as depression or hypomania), gastrointestinal manifestations and changes in fluid balance. Usually the onset of the common migraine headache is unilateral, but the pain often becomes holocephalic. In an individual patient the headache is commonly more prominent on a single side, with occasional or rare alternation. Some individuals always experience a unilateral headache, while in approximately one-third the headache is diffuse from onset. Traditionally, the character of the headache is described as throbbing but this may be a feature only at onset, with the discomfort soon changing to a steady ache. The victim can often relieve unilateral headache by carotid artery or temporal artery compression, only to experience resurgence of the pain after release.
Nausea in some degree almost always accompanies common migraine. Vomiting can occur at the height of an attack, sometimes with relief of the headache, but more often only signals an intensifying phase of the episode, which continues for many minutes or hours. Usually the migraine sufferer becomes pallid and seeks seclusion, darkness, quiet, and a cold towel or ice bag for the head. Frequently at the time of nausea with vomiting, a diuretic phase with polyuria ensues, the consequence of fluid retention that occurred in the hours or days preceding the acute headache.
Ocular signs and symptoms may occur in common migraine, such as conjunctival injection, periorbital swelling, excessive tearing, foreign body sensation, and photophobia; however, these phenomena are more prominent in cluster headache.
MIGRAINE WITH AURA (CLASSIC)
The new term for classic migraine, that is migraine with aura, requires at least two attacks with any three of the following four features (Table 3): one or more fully reversible aura symptoms; aura developing over a course of more than 4 minutes; aura lasting less than 60 minutes; and headache after aura within 60 minutes. Migraine with aura refers to a more well-defined clinical constellation than does migraine without aura. The episodes are characterized by definite prodrome or aura, which is usually a visual sensation; however, sometimes motor or other sensory phenomena precede the headache. The headaches of classic migraine tend to be more compact and intense, rarely lasting more than 12 hours; most often 2 to 3 hours.
TABLE 3. Migraine with Aura | ||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Many general characteristics are shared by common and classic migraine. Both varieties affect men and women and can occur at any age, often seemingly triggered by a significant event such as puberty, school graduation, or marriage. A family history is usually present both in classic and common migraine and there may be an earlier history of colic as a baby or car illness as a small child. The full history of a complete migraineur would include migraine with aura in the teens, migraine without aura with nausea and vomiting in the second and third decades, followed by simple periodic headache or isolated migrainous auras in later life.
Migraine with aura is subclassified into migraine with typical aura (homonymous visual disturbance, unilateral numbness or weakness, or aphasia); migraine with prolonged aura (or lasting longer than 60 minutes); familial hemiplegic migraine; basilar migraine; migraine without headache and migraine with acute-onset aura.
The primary feature of migraine with aura is the visual aura. Extensive reviews of this phenomenon are found throughout the literature.5,6,34,65,66,67 While many variations occur, the following description by Richards44 summarizes the most common type of visual phenomena (Figs. 2 and 3):
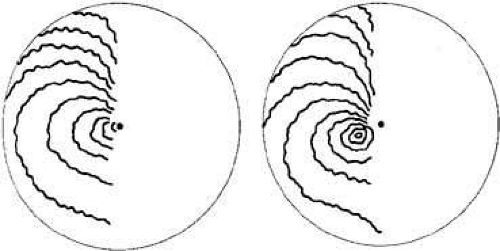 Fig. 2 Successive arcs expand across half of visual field, as shown in two diagrams based on Airy. The spectra may take 20 to 25 minutes to expand from a fuzzy gray area near the fixation point (dot) to the outer limit of the visual field. (Richards W: The fortification illusions of migraines. Sci Am 224:88, 1971) |
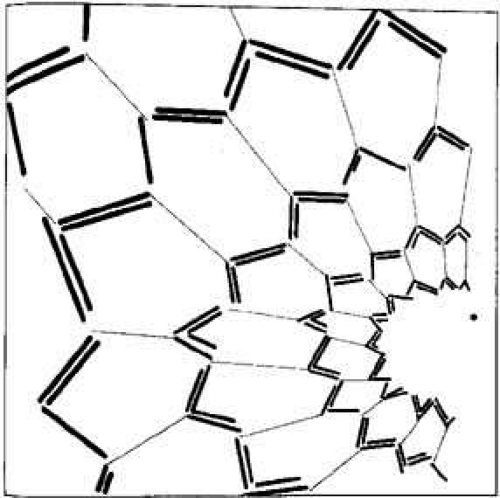 Fig. 3 Emerging honeycomb pattern from plotting data derived from visual phenomena in migraine subjects. Honeycomb and tendency for inner angle between lines to approximately 60 degrees suggest a hexagonal organization of occipital cortical cells. (Richards W: The fortification illusions of migraine. Sci Am 224:88, 1971) |
The visual disturbance usually precedes the headache… [it] begins near the center of the visual field as a small gray area with indefinite boundaries. If this area first appears during reading, as it often does, then the migraine is first noticed when words are lost in a region of “shaded darkness.” During the next few minutes the gray area slowly expands into a horseshoe with bright zigzag lines appearing at the expanding outer edge. These lines are small at first and grow as the blind area expands and moves outward toward the periphery of the visual field.
One important aspect of the visual disturbance just described, is that it expands slowly, over a period of 10 to 20 minutes. The initial region of visual abnormality is most often near fixation and then, as described by Lashley,49 with increase in size the disturbed area moves or “drifts” across the visual field so that its central margin withdraws from the macular region as its peripheral margin invades the temporal; the area may be totally blind (negative scotoma), amblyopic or outlined by scintillations.
The scintillations surrounding the negative scotoma make “fortification” figures or spectrums, so called by the appearance of a “map of the bastions of a fortified town.”49 The scintillations are brilliant, with the intensity of a bright fluorescent bulb flickering at a rate of 5 to 10 cycles per second (Figs. 4 and 5).
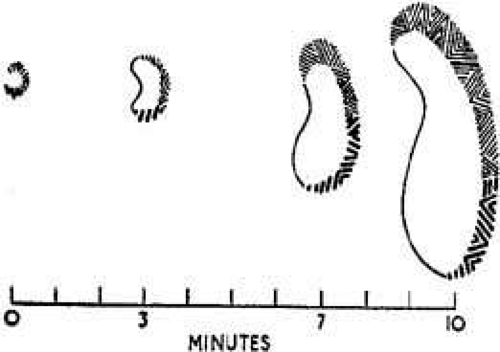 Fig. 4 Successive maps of a scintillating scotoma to show characteristic distribution of the fortification figures. (Modified from Lashley KS: Patterns of cerebral integration indicated by scotomas of migraine. Arch Neurol Psychiatry 46:333, 1941. Copyright © 1941, American Medical Association) |
 Fig. 5 Variations in fortification figures. Coarser and more complicated figures are generally in lower part of field. (Lashley KS: Patterns of cerebral integration indicated by scotomas of migraine. Arch Neurol Psychiatry 46:333,1941. Copyright © 1941, American Medical Association) |
Gowers,68 commenting on the descriptions by the British astronomer, Sir George Airy, and his physician son, Dr. Hubert Airy (both migraineurs), was particularly impressed with the intensity of the visual sensation. Many migraine sufferers can precisely recall their own vivid visual experiences well enough to describe them precisely or even on occasion to paint them (Fig. 6 and 7). Not all migraine visual disturbances begin near the fixation point; some patients consistently experience scotomas starting eccentrically in the visual field, and these sensations can appear alternately or simultaneously in both hemifields (Fig. 8). Other less dramatic visual auras also occur: just the sensation of peripheral brightness or awareness of a rhythmicity or pulsating character in the intensity of the ambient light. The duration of these visual symptoms is measured in minutes rather than the brief few seconds of flashing, bright moving spots, or transient flickering phenomena characteristic of occipital epileptic discharges.7,68 Additional visual disturbances are categorized by Klee and Willanger,66 consisting of metamorphopsia, diplopia, polyopia, and apparent movement of stationary objects. Variations in the scotomas of migraine, including their occurrence in patients with acquired blindness, are well described.65,69 The auras of migraine, although most commonly only visual, have many other associated manifestations, such as hemihypesthesias, perioral anesthesia, vertigo, and transient aphasia. The aura or prodromes of classic migraine may be precipitated by intense stimuli: bright lights, loud noises, head trauma, or the intake of certain foods in susceptible individuals.
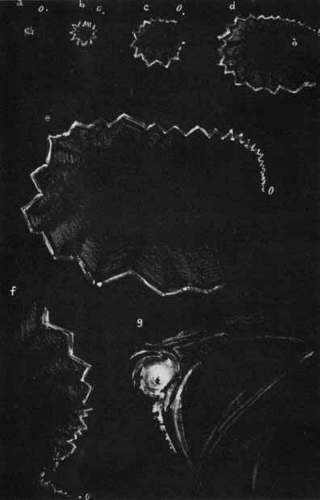 Fig. 6 Left-sided fortification spectrum of migraine. Illustration by Dr. Hubert Airy of his own scotomas. A bright stellate object (A) appeared suddenly below and to the left side of fixation (o). It rapidly enlarged, first as a circular zigzag, but on the inner side the zigzag was faint (B); as arc increased in size, it was broken centrally (C). In D, original circular outline had become oval. Rectangular lines that made up the fortification spectrum became longer as the process extended peripherally. When spectrum had extended through greater portion of the field (E), upper portion also began to expand (F). At this time the lower part of spectrum disappeared. The phenomenon ended in a whirling focus of light (G) 20 minutes after it began. At this time a headache appeared on the right side. (Gowers WR: Visual sensations in migraine. In Subjective Sensations of Sight and Sound: Abiotrophy and Other Lectures. London: Churchill, 1907) |
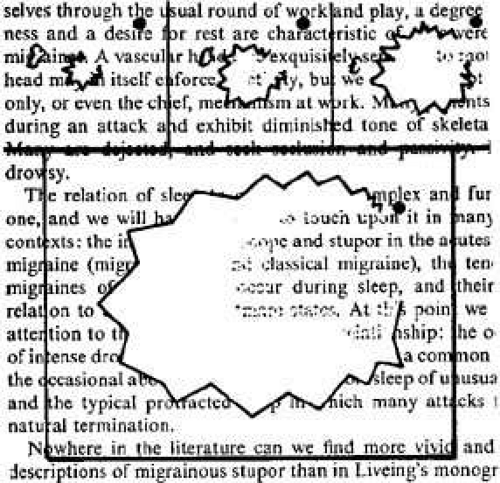 Fig. 7 Inhibitory character within angled oval of an expanding fortification spectrum. Outside the limiting line, vision is preserved; within it, vision is lost. This occurs at first over the whole area; afterwards, when the sphere is broken and has become oval, loss is most intense close to the limiting line and becomes less toward the middle. (Gowers WR: Visual sensations in migraine. In: Subjective Sensations of Sight and Sound: Abiotrophy and Other Lectures. London: Churchill, 1907) |
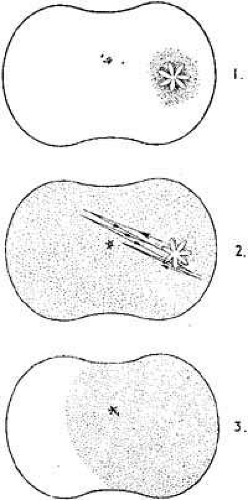 Fig. 8 Radial movement of a visual stellate object that itself remained unchanged throughout the episode. Stellate form appeared near edge of right half of field just below the horizontal and consisted of approximately six pointed leaf-like projections alternately red and blue. It appeared on a small area of darkness, moved slowly toward the left and upward, passing above the fixation point to beyond the middle line. Then it returned to its starting place, retraced this path once or twice and passed to the right edge of the field, suddenly disappearing at the spot where it began. (Gowers WR: Visual sensations in migraine. In Subjective Sensations of Sight and Sound: Abiotrophy and Other Lectures. London: Churchill, 1907) |
In the usual sequence of migraine with aura the sensory prodrome precedes the onset of the headache (in accord with the traditional concept of vasoconstriction followed by vasodilatation). The visual disturbance rarely may have a simultaneous onset with headache or, once having disappeared, may recur following the onset of headache. Such unusual patterns, or strict unilaterality for all attacks, should increase suspicion of a mass lesion or vascular malformation. As opposed to definite periodicity with symptom-free intervals and predictable circumstances, as in migraine without aura, migraine with aura may occur “out of the blue” and in multiple attacks over a few days.
Migraine-with-aura attacks tend to diminish in the third and fourth decades. While most migraine patients experience a stereotyped clinical pattern, there is a well-recognized group in which both classic and common migraine attacks are admixed.70 Some patients with classic migraine may lose the headache component eventually and suffer only isolated auras thereafter. This monosymptomatic pattern stresses the importance of accurate history-taking when confronted by a patient with isolated visual phenomena (migraine dissociée). Haas71 emphasized the occurrence of “migraine aura status”. The differential diagnosis should include consideration of vertebro-basilar transient ischemic attacks. Symptomatology that favors migraine has been reviewed by Fisher,72 and includes luminous visual images, build-up of images, progression from one aura to another, and benign outcome.
MIGRAINE WITH PROLONGED AURA AND MIGRAINOUS INFARCTIONS
In the new classification of migraine,1 subtype 1.6 indicates complications of migraine. This would include all of the permanent defects discussed in this section.
Focal symptoms and signs of the aura may persist beyond a headache phase. In the previous classification, this was termed complicated migraine. It is now defined by the IHS classification with two labels with increased specificity. If the aura lasts for longer than 1 hour but less than 1 week, the term migraine with prolonged aura is applied. If the signs persist for more than 1 week or a neuroimaging procedure demonstrates a stroke, a migrainous infarction has occurred. As pointed out previously, in mid or later life the aura may not be followed by headache and has been termed migraine accompagnée or migraine associée. Migraine with aura (classic) in early reports was sometimes referred to as “ophthalmic migraine” (to be differentiated from ophthalmoplegic migraine, a subtype of migraine with aura). Migraine with aura is further reviewed in sections Cerebral, Ophthalmoplegic, Retinal, Basilar, and Other Varieties.
CEREBRAL
A variety of cerebral symptoms may occur in migraine with aura, including motor, visual, and other sensory defects. As pointed out previously, if the aura lasts for more than 1 hour but less than 1 week, the term migraine with prolonged aura is applied. However, if the signs persist for more than 1 week or a neuroimaging procedure shows a stroke the term used is migrainous infarction. The HIS classification of migraine-related stroke is presented in Table 4. Welch23 has classified migraine-related stroke into four subtypes. These are described briefly.
TABLE 4. Classification of Migraine-Related Stroke | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
|
1. Coexisting Stroke and Migraine
A clearly defined clinical stroke syndrome must occur remotely in time from a typical migraine attack. Stoke in the young is rare; in contrast, migraine is common. As pointed out by Welch, the two conditions should coexist without migraine being a contributing risk factor for stroke.
2. Stroke with Clinical Features of Migraine
A structural lesion that is unrelated to migraine pathogenesis presents with clinical features of a migraine attack. Subtype A is symptomatic and in these patients, established structural central nervous system (CNS) lesions or cerebral vessels cause episodic symptoms typical of migraine with neurologic aura, although infrequently. Such cases could be termed symptomatic migraine. Cases of cerebral arteriovenous malformation exemplify this concept and may masquerade as migraine with aura.7,73
Welch’s second subtype is a migraine mimic. In this category, stroke caused by acute and progressive structural disease is accompanied by headache and a constellation of progressive neurologic signs and symptoms. These situations are difficult to distinguish from those of migraine, hence the term migraine mimic. The diagnosis can be most difficult in patients who continue to have migraine late in life, when the incident of cerebrovascular disease increases.23
3. Migraine-Induced Stroke
Migraine-induced stroke must meet the following criteria: neurologic deficit must be identical to the migraine symptoms of previous attacks; the stroke must occur during the course of a typical migraine attack; and all other causes of stroke have been excluded, although stroke risk factors may be present.
4. Uncertain Classification
Welch has indicated that many migraine-related strokes cannot be categorized with certainty. For example, the IHS definition of migraine-induced stroke does not prevent the diagnosis in patients with migraine without aura. Migraine-induced stroke associated with treatment of the attack is appropriately classified in category. In addition, there are occasional cases of migraine-like symptoms and persistent neurologic deficit associated with cerebrospinal fluid (CSF) protein and pleocytosis.74,75 Other rare syndromes and migraine-related stroke include migraine associated with mitochondrial encephalopathies76 and “migraine coma.”77 Intracerebral hemorrhage has been reported,78 with most cases, according to Welch, being migraine mimics. Whether there is a role of antiphospholipid antibodies is still to be determined.79 Permanent homonymous visual field defects are well documented in migraine patients.67,80,81,82 The defects almost always occur in patients who have previously had migrainous attacks with transient scintillating scotomas. Computed cranial tomography (CT) or magnetic resonance imaging (MRI) has now documented a number of cerebral infarctions usually in the occipital and parietal regions. Rothrock and colleagues83 evaluated 22 patients with migraine-associated stroke finding that 91 percent were women and 23% had a prior history of presumed migrainous stroke. They concluded that extracranial and intracranial vasospasm played a major role in some cases that they were able to document angiographically. One controlled study of migraine with aura reported that 91% of patients who had stroke during an attack had no arterial lesions. This was as opposed to 9% of migraine with patients with aura who suffered stroke remote from a migraine attack and 18% of patients with stroke without a migraine history.84 In a rigorous case controlled study no overall association between migraine and ischemic stroke was found, but among women younger than 45 years, migraine and stroke were significantly associated; the risk was increased fourfold and it became even greater in women who smoked.85
According to Hollenhorst,86 approximately 4% of patients who have a typical sequence of visual aura followed by hemicranial headache experience transient hemianopsia lasting up to 15 minutes. Much rarer are patients with permanent hemianopia. Bilateral upper quadrantic defects have been reported.87,88
Other sensory disturbances such as paresthesias particularly involve hands, fingers, and
lips.87,88,89 Various aspects of cerebral migraine with aura are illustrated by the following case history.
A 26-year-old woman was seen with a complaint of difficulty with vision. She had a history of migraine since the age of 12, characterized by an aura of “black spots” slowly spreading over the field of vision for 20 minutes, occasionally accompanied by numbness in the right hand and arm. Thereafter throbbing headache would occur that was left-sided 90% of the time. Her father had a history of classic migraine as a young man. Ten days prior to first being seen, she had a typical attack of migraine but with persistent difficulty in vision after the episode. Examination was entirely normal except for a congruous right homonymous visual field defect (Fig. 9). Ten days later she again developed her visual aura, but with a moderate right hemiparesis as well, during her headache. Brain scan and cerebral arteriography were normal. During the next week all neurologic abnormality including her visual field defect cleared completely.
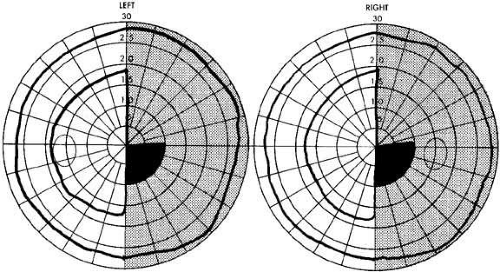 Fig. 9 Visual field defect in complicated migraine. Defect cleared completely. Visual acuity 20/20 OU. Relative homonymous hemianopia (2, 5/1000 w; scotoma out to 30/1000 w). |
Frequently a disturbance of language occurs with migraine, as pointed out by Sir George Airy in 1865, who described his own inability to speak during an attack. A typical history related to the author by his brother is as follows.
While reading, I become aware that I am unable to understand what I have just read. After rereading a paragraph two or three times, I begin to realize that I cannot understand the sense of words. The letters can be identified but the words are unintelligible… At this point a numb feeling occurs in my right hand and I finally realize that I am at the start of another migraine attack.
A wide variety of language difficulties, sensory defects, and motor abnormalities have been described (most often transient but rarely permanent) from presumed cerebral infarction. Caplan et al.90 reported 12 patients with transient global amnesia and prior migraine. In 3 patients, the classic migrainous phenomenon accompanied the amnestic attack.
Variable electroencephalographic (EEG) findings occur.89,91,92 There is general lack of agreement as to the incidence and significance of abnormalities in the EEGs of patients with migraine. Some authors report a normal EEG,93 but various abnormal patterns have been recorded.91,92 A detailed review by Hockaday and Whitty94 indicated an incidence of EEG abnormality in 61% of 560 migraine patients. The highest frequency of abnormality occurred in patients with transient lateralized motor or sensory auras.
Friedman95 first reported the results of angiography during an attack of migraine; there were no abnormalities. While the majority of patients in reported cases show normal arteriograms, others have demonstrated some abnormality during an attack (see Cluster Headache). However, angiography is considered by some to have increased risk in patients with migraine67,96 and has not yet provided useful information on the pathophysiology of complicated migraine.97,98,99
Hemiplegic migraine occurs both sporadically and as a familial syndrome. This entity is defined as “vascular headache” featuring sensory and motor phenomena that persist during and (for a brief time) after the headache.100 A narrower view would be to use the term hemiplegic migraine when only motor involvement (i.e., weakness or paralysis) occurs.
The first mention of transient hemiparesis during an attack of migraine was by Liveing,5 and multiple reviews and case reports have appeared since.101,102 Heyck103 reviewed the neurologic complications of 980 of 3890 patients with migraine. The majority of these patients complained of unilateral tingling or numbness that invariably involved the hand and sometimes spread to the arm, face, tongue, and, rarely, to the leg. The symptoms seldom lasted more than 30 minutes and could occur before or at the peak of the headache. Twelve of these patients had unilateral motor disturbances ranging from minimal loss of function to complete paralysis. There have been few permanent sequelae attributed to hemiplegic migraine; progressive dementia was noted by Symonds, and permanent hemiplegia has been reported.89,97,103
Reports of hemiplegic migraine in the literature seem to indicate that most cases are familial. However, Heyck97 pointed out the tendency to report familial cases; if unselected patients with the syndrome are reviewed, most do not occur in families with hemiplegic migraine but rather in “families with ordinary migraine as often as common or classic migraine.” Familial hemiplegic migraine is well documented,101,104,105 at times in kindred with associated neuro-ophthalmologic findings such as retinal degeneration and nystagmus.106 One interesting report is that of Dooling and Sweeney,107 who describe a blind woman whose attacks were precipitated by breast feeding her infant. This led to the speculation that oxytocin (chemically similar to ergotamine) could exercise a complex effect on cerebral vessels predisposed to vasospasm.
OPHTHALMOPLEGIC
So-called ophthalmoplegic migraine has now been changed in the official Classification of Headache of the International Headache Society.1 This is because many reports have shown abnormalities of the oculomotor nerve using MRI in children with recurrent painful ophthalmoplegia fulfilling the previous criteria for ophthalmoplegic “migraine.”108,109 It is now believed that all modern cases show MRI enhancement of the third nerve, which may represent a type of inflammation and, therefore, more characteristic of what is seen with facial nerve palsy than with any form of migraine.110 In this rare variety of what was formerly termed “complicated migraine” the headaches were associated with oculomotor nerve palsies.111,112 Usually the ophthalmoplegia is transient, however, it can become permanent especially after repeated attacks. Major controversy has surrounded the diagnostic and nosologic position of ophthalmoplegic “migraine” since its initial recognition in the mid 1880s. Until the 1930s and 1940s when angiography was introduced and practiced, it was impossible in many cases to rule out aneurysms and other lesions in the vicinity of the cavernous sinus. Multiple etiologies were cited as underlying causes of ophthalmoplegic “migraine” including aneurysm, basilar arachnoiditis, and tumors; indeed, many physicians believed that no separate clinical syndrome of ophthalmoplegic migraine existed but that all patients had specific organic lesions.
Woody and Blaw113 reported two cases of ophthalmoplegic “migraine” occurring in infants who were 5 and 7 months old. The infants had recurrent attacks with almost complete clearing between episodes. Both children were treated with prednisone during subsequent attacks, which seemed to shorten the duration of the episodes.
In ophthalmoplegic “migraine” the third nerve is most frequently involved. Walsh and Hoyt67 state that abducens palsy occurs 1:10 as frequently as third-nerve palsy, with even rarer affliction of the fourth nerve. In most cases positive family history is not present. Thus, a typical clinical syndrome emerges: a child or young adult with periodic headache has ophthalmoplegia involving all functions of the third nerve, beginning at the height of an attack of cephalgia, which is primarily unilateral and in the orbital region; the paresis lasts for days to weeks after the cessation of headache; recovery is gradual and tends to be less complete after repeated attacks. The following case report is considered exemplary.
A 3-year-old boy presented with a complete left oculomotor palsy. The day before he had complained of headache, was lethargic, and went to bed early. The following morning he awakened with complete ptosis of the left upper lid but his headache was gone. On examination the left pupil was 6 mm and slightly reactive to light; all muscles supplied by the left third nerve were profoundly affected (Fig. 10), The neurologic examination and plain skull x-rays were entirely normal. The child recovered completely in 3 weeks’ time. An exactly similar episode occurred 20 months later, also with rapid spontaneous resolution, and a third episode occurred 1 year after that. The child is now well and suffers only occasional headaches.
 Fig. 10 Third-nerve paresis in 3-year-old boy with ophthalmoplegic migraine. Pupil was sluggishly reactive to light. Note failure of elevation, abducted position of left eye, and ptosis. |
In the differential diagnosis, consideration should be given to aneurysm, tumor, diabetes, and sphenoid sinus mucocele. The age at onset, negative glucose tolerance test, and radiologic studies will usually rule out the listed possibilities. Other clinical entities confused with ophthalmoplegic “migraine” have included myasthenia gravis and the Tolosa-Hunt syndrome. The former condition is ruled out if the pupil is involved (and actually should not be considered in the presence of pain) and with response to edrophonium chloride (Tensilon); the latter possibility should be considered if pain persists. On rare occasions only limited involvement of the third nerve occurs.
Reports of transient, otherwise unexplained unilateral pupillary mydriasis have been tentatively attributed to migraine in young patients.114,115 One should be careful to exclude intermittent angle-closure glaucoma with mydriasis as pointed out by Sarkies and colleagues.116 They reported a 31-year-old man with an 18-month history of episodic periorbital pain who, during an attack, noted blurred vision and a dilated pupil. He was found to have a sector palsy in the upper nasal quadrant of the left iris, an intraocular pressure of 16 mm Hg between attacks and on gonioscopy, and narrow angle with a plateau-type iris. During an attack his intraocular pressure increased to 26 mm Hg. After a provocative dark-room test, the patient developed a typical headache and was found to have an intraocular pressure of 45 mm Hg and a closed-angle on gonioscopy. This report is important because it points out a condition that must be eliminated before considering episodic mydriasis with ocular pain to be a part of ophthalmoplegic “migraine.”
Rarely, ophthalmoplegic “migraine” may occur without headache. Durkan et al.117 described two children with isolated recurrent painless oculomotor palsy in whom neurodiagnostic investigations were all normal.
In the differential diagnosis, suspicion would be raised by (1) the absence of a migraine history; (2) severe persistent headache with total ophthalmoplegia; (3) onset after age 20; and (4) symptoms and signs of subarachnoid hemorrhage. Angiography is not warranted in a young patient strictly fulfilling the clinical criteria.
Now, however, ophthalmoplegic “migraine” is a diagnosis of exclusion, and noninvasive imaging tests such as MRI or magnetic resonance angiography (MRA) should be performed in all cases to exclude the possibility of aneurysm.112 The finding of an entirely normal MRI, except for nerve enhancement, in a child with a third cranial nerve palsy after a 4 day history of headache, who is otherwise well, should complete the workup. This is because aneurysmal third-nerve palsies are extremely rare in children under age 14 years.118 However, in third nerve palsy involving pupillomotor function, serious consideration should be given to angiography. The usual cause will be a posterior communicating artery aneurysm, which is best excluded by conventional angiography. However, newer techniques such as MRA or spiral contrast-enhanced computed tomographic scanning may soon provide sufficient resolution to exclude aneurysm as a cause.112
The pathophysiology of ophthalmoplegic “migraine” remains obscure. Theories include swelling of the posterior cerebral artery, pituitary swelling, vascular anomaly with compression of the third nerve, and unilateral brain swelling. None of these theories has been documented, and cerebral angiography is unrevealing. Walsh and O’Doherty119 suggested that a swollen intracavernous carotid artery compressed adjacent cranial nerves within the cavernous sinus. Such swelling would also narrow the vessel, which they attempted to document angiographically. However, subsequent negative arteriograms during attacks do not support this theory.120 In Nigeria, ophthalmoplegic “migraine” has been associated with an abnormal hemoglobin.121
Ideally, prophylactic therapy would prevent the occurrence of repeated episodes and prevent the development of permanent eye muscle palsies, but reports suggest that therapy has met with only limited success.120 A trial with calcium channel blocking drugs such as verapamil or β-blocking drugs such as propranolol or even methysergide may be warranted if the attacks are frequent.
RETINAL
The IHS code is 1.4 for retinal migraine (Table 5). A short description from the Headache Classification Committee is the following: repeated attacks of monocular scotoma or blindness lasting less than 1 hour and associated with headache. Other ocular or structural vascular disorder must be ruled out. Additional terms include: ocular migraine, anterior visual pathway migraine, and ophthalmic migraine. This condition may be broadly defined as a transient or permanent monocular visual disturbance accompanying a migraine attack or occurring in an individual with a strong history of migrainous episodes.110 One term applicable to all such attacks would be “ocular migraine, “however, to include optic nerve dysfunction as well, a more general phrase (i.e, “anterior visual pathway migraine)” may be preferable. This last phrase would include reported defects, such as ischemic papillitis, retinal hemorrhage, vitreous hemorrhage, central serous retinopathy, pigmentary changes of the retina, and optic nerve atrophy.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


