 Melanocytoma of the Optic Disc and Posterior Uvea
Melanocytoma of the Optic Disc and Posterior UveaMelanocytoma of the Optic Disc and Posterior Uvea
General Considerations
Melanocytoma is a variant of melanocytic nevus that is classically located on the optic disc. Since the nature of optic nerve melanocytoma was elucidated by Zimmerman, many articles have been published on this unusual ocular neoplasm (1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38). It is presumed to be congenital and nonhereditary and is a deeply pigmented lesion that usually is located on all or part of the optic disc. Unlike uveal melanoma, optic disc melanocytoma does not appear to have a predilection for whites. Historically, optic disc melanocytoma was often confused with malignant melanoma both clinically and histopathologically. Today, however, it is generally recognized by its typical clinical features, which differ from those of most melanomas, and erroneous enucleation is rarely done.
Although it was originally believed to be unique to the optic disc, it is now recognized to also occur in the iris, ciliary body, and choroid. Iris melanocytoma is discussed in Chapter 2 because it is a variant of melanocytic tumor of the iris stroma. Because most choroidal melanocytomas are impossible to differentiate clinically from other deeply pigmented choroidal nevi, they do not come to histopathologic evaluation.
Clinical Features
The clinical features of posterior uveal melanocytoma vary depending on whether the lesion is located on the optic nerve, choroid, or ciliary body.
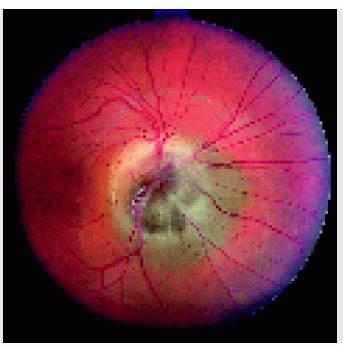
Optic Nerve Melanocytoma. A recent review of 115 patients with optic nerve melanocytoma seen by the authors (7) revealed that mean age at diagnosis was 50 years; 38% were male, 62% female, 65% white, 29% African American, and 6% Asian, Hispanic, Indian, or Arabic. The lesion was unilateral in 99%. Visual symptoms that appeared related to the melanocytoma were present in 24%, and an afferent pupillary defect was noted in 9%. The melanocytoma was dark brown to black in 100%. The mean tumor diameter was 2 mm, and the mean thickness was 1 mm. Associated findings included a choroidal component (54%), retinal component (30%), optic disc edema (25%), retinal edema (16%), localized subretinal fluid (14%), retinal exudation (12%), retinal hemorrhage (5%), vitreous seeds (4%), and retinal vein obstruction (3%).
Optic nerve melanocytoma has a marked tendency to undergo spontaneous necrosis, which can result in profound visual loss. About 10% to 15% show subtle enlargement over several years, but that does not usually mean malignant transformation. Malignant transformation into melanoma occurred in 1% to 2% (7).
Localized Choroidal Melanocytoma. Unlike its optic disc counterpart, melanocytoma of the choroid does not possess highly specific clinical features. Because it is a variant of choroidal nevus, it may be indistinguishable clinically from other deeply pigmented choroidal nevi. The diagnosis can be suspected on the basis of ophthalmoscopy that shows the lesion to be black to dark brown and it is, by definition, never amelanotic. As mentioned earlier, most ciliary body and choroidal melanocytomas are not confirmed histopathologically, and no highly reliable clinical diagnostic criteria have been established. Fluorescein angiography and ultrasonography are probably of no benefit in making the diagnosis. Presumed melanocytoma has rarely been recognized in the central retina, although histopathologic confirmation is lacking (28).
Ciliary Body. Ciliary body melanocytoma, like choroidal melanocytoma, does not have any specific diagnostic criteria. It appears to be similar to other deeply pigmented ciliary body tumors such as melanoma and adenoma of the ciliary pigment epithelium. However, we have made an accurate diagnosis of ciliary body melanocytoma on several occasions based on its intense black color and seeding from the tumor, presumably due to necrosis.
Diffuse Uveal Melanocytoma. In some patients with classic ocular melanocytosis, the eye is enucleated for choroidal melanoma, and the entire uveal tract is found to be thickened by deeply pigmented cells with cytologic features identical to those of melanocytoma. This was pointed out by Zimmerman in his early publication on the subject (2). It is believed that this diffuse melanocytoma and ocular melanocytosis represent the same entity. Diffuse uveal melanocytoma, like ocular melanocytosis, can give rise to localized melanoma, multifocal melanoma, and diffuse melanoma (36).
Diagnostic Approaches
Fluorescein angiography of optic disc melanocytoma typically shows hypofluorescence throughout the angiogram, sometimes with hyperfluorescence of secondary disc edema or retinal pigment epithelium atrophy. It is probably of no value in differentiating choroidal or ciliary body melanocytoma from melanoma, nevus, or pigment epithelial tumors. On several occasions, we have diagnosed melanocytoma of the iris or ciliary body by cytopathologic study of fine needle aspiration biopsy.
Pathology
Histopathologically, optic nerve melanocytoma is deeply pigmented due to abundant large melanosomes in the cytoplasm (1, 2, 3). Bleached preparations reveal the cells to be ovoid with abundant cytoplasm, relatively small nuclei, and few prominent nucleoli. Zimmerman agreed that his term melanocytoma was nonspecific, and credited Cogan with recommending the term magnocellular nevus in its place. We proposed the term hyperpigmented magnocellular nevus, which we believe is even more accurate, and we hope that this term will be accepted (38). In cases that come to histopathologic confirmation, necrosis is a common feature, sometimes with pseudocysts containing free-floating melanophages. Melanocytoma of the iris, ciliary body, and choroid have identical cytologic features.
Management
Rarely, a melanocytoma of the optic disc can evolve into malignant melanoma (7,8,13,14,31). Therefore, fundus photography and clinical evaluation should be done once or twice a year. Small degrees of growth may not signify malignant change. However, more progressive growth and visual loss should suggest malignant transformation. Enucleation may be the best treatment for a melanocytoma with documentation of growth and severe visual loss. Fine needle aspiration biopsy may be done first to confirm transformation into melanoma. Suspected melanocytoma of the choroid or ciliary body can be observed or managed like a comparable-sized melanoma, as described subsequently in the chapter on management of posterior uveal melanoma.
Selected References
1. Zimmerman LE, Garron LK. Melanocytoma of the optic disc. Int Ophthalmol Clin 1962;2:431-440.
2. Zimmerman LE. Melanocytes, melanocytic nevi, and melanocytomas: The Jonas S. Friedenwald Memorial Lecture. Invest Ophthalmol 1965;4:11-40.
3. Shields JA, Shields CL. Melanocytoma. In: Shields JA, Shields CL, eds. Intraocular Tumors. A Text and Atlas. Philadelphia: WB Saunders; 1992: 101-115.
4. Shields JA. Melanocytoma of the optic nerve head. A review. Int Ophthalmol 1978;1:31-37.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


