 Melanocytic Tumors of Iris Stroma
Melanocytic Tumors of Iris StromaIris Nevus
General Considerations
The common iris nevus is covered well in the literature (1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29). In contrast to iris freckle, a nevus effaces the architecture of the iris stroma. Iris freckle occurs in about 60% of the population and probably has no malignant potential, whereas an iris nevus occurs in 5% of the population and may rarely give rise to malignant melanoma. There are conflicting reports regarding a relationship between iris nevus and choroidal melanoma (7,12,25). Iris nevus, like other melanocytic uveal tumors, shows a predilection for whites and becomes clinically apparent during puberty or young adulthood.
Clinical Features
The size, shape, and pigmentation of iris nevus can vary from case to case (6). It can be small and circumscribed, large and diffuse, or flat to dome shaped, and can sometimes show satellite seeding into the adjacent iris. It can be entirely amelanotic and transparent, or it can be deeply pigmented. Greater than 80% are located in the inferior half of the iris (15). It was once believed that an irregular pupil, angle involvement, secondary cataract, secondary cyst, tapioca configuration, and adjacent transcleral extension were signs of malignant transformation. However, we now know that many iris nevi can produce such secondary changes (1). Overall, about 5% of borderline suspicious iris nevi show growth within 5 years after diagnosis and evolve into low-grade melanoma (5). Secondary glaucoma associated with iris nevus is extremely rare, and significant elevated intraocular pressure should raise suspicion of iris melanoma. Iris nevus can frequently be associated with a pigment epithelial cyst immediately posterior to the lesion (1,17).
A variation of iris nevus is melanocytoma, a lesion that may simulate melanoma and is best known to occur on the optic disc. In contrast to ordinary nevus and melanoma, it is more deeply pigmented and can readily undergo necrosis and pigment dispersion and can induce secondary glaucoma (2,3,9,11,29). The glaucoma seen with melanocytoma is due to obstruction of trabecular meshwork by melanophages that contain pigment liberated by necrotic melanocytoma cells. Hence, this condition has been termed melanocytomalytic glaucoma (3). Histopathologically confirmed iris melanocytoma has been documented to show clinical enlargement in young children (8). In some instances, iris melanocytoma can represent anterior extension of a larger melanocytoma in the ciliary body (19,20). Like other iris nevi, iris melanocytoma can undergo malignant transformation (1,21,22,29). In such cases, the melanoma component may be only a small focus within the benign lesion.
An unusual variation of iris nevus observed by the authors is an amelanotic lesion that can show growth, suggesting malignancy. When such tumors have come to histopathologic evaluation, it may be difficult for pathologists to determine whether the lesion is benign or malignant microscopically. This condition has been observed to have a familial tendency (16). An iris nevus that has received little mention in the literature is the sector iris nevus. This lesion appears as a well-defined sector of increased pigmented that extends from the pupil to the angle. It can range in size from 1 to >6 clock hours. This lesion is probably congenital, and we consider it to be a localized form of ocular melanocytosis. In some instances, an iris nevus can have a multinodular surface that resembles tapioca. A tapioca nevus can be remarkably similar to tapioca melanoma. Although we are not aware of publications on tapioca nevi, we have diagnosed it on many occasions. Another variation is the diffuse iris nevus (Cogan-Reese syndrome) (10), a condition that may fall in the spectrum of the iridocorneal endothelial syndrome, discussed in Chapter 3.
Pathology
Histopathologically, iris nevus cells can range from slender spindle cells to rounded cells similar to those seen in melanocytoma of the optic nerve. Rarely, benign epithelioid cells may predominate, suggesting a diagnosis of melanoma (27). In borderline cases, iris nevus may be difficult to differentiate microscopically from a low-grade melanoma (3). Not surprisingly, it has been shown that nucleolar size is statistically smaller in iris nevus than in iris melanoma (13).
Management
Concerning management, the patient should be informed that the chances of malignant transformation are relatively low (1, 2, 3, 4, 5). Baseline photographs and examination every 6 to 12 months is recommended to detect evidence of growth. Fluorescein angiography has little value in diagnosis. Ultrasound biomicroscopy (UBM) can help to detect adjacent ciliary body involvement and to follow the lesion for growth. It can help to differentiate nevus in the angle from cyst. If photographic evidence of growth is documented, then active treatment should be considered. This is covered in the next section on iris melanoma.
Selected References
1. Shields JA, Shields CL. Melanocytic tumors of the iris stroma. Nevus. In: Shields JA, Shields CL, eds. Intraocular Tumors. A Text and Atlas. Philadelphia: WB Saunders; 1992:62-69.
2. Shields JA, Annesley WH, Spaeth GL. Necrotic melanocytoma of iris with secondary glaucoma. Am J Ophthalmol 1977;84:826-829.
3. Fineman M, Eagle RC Jr, Shields JA, et al. Melanocytomalytic glaucoma in eyes with necrotic iris melanocytoma. Ophthalmology 1998;105:492-496.
4. Jakobiec FA, Silbert G. Are most iris “melanomas” really nevi? Arch Ophthalmol 1981;99:2117-2132.
5. Territo C, Shields CL, Shields JA, et al. Natural course of melanocytic tumors of the iris. Ophthalmology 1988;95:1251-1255.
6. Shields JA, Sanborn GE, Augsburger JJ. The differential diagnosis of malignant melanoma of the iris. A clinical study of 200 patients. Ophthalmology 1983;90:716-720.
7. Harbour JW, Brantley MA Jr, Hollingsworth H, et al. Association between posterior uveal melanoma and iris freckles, iris naevi, and choroidal naevi. Br J Ophthalmol 2004;88:36-38.
8. Shields JA, Eagle RC Jr, Shields CL, et al. Progressive growth of an iris melanocytoma in a child. Am J Ophthalmol 2002;133:287-289.
9. Kiratli H, Bilgic S, Gedik S. Late normalization of melanocytomalytic intraocular pressure elevation following excision of iris melanocytoma. Graefes Arch Clin Exp Ophthalmol 2001;239:712-715.
10. Ozdemir Y, Onder F, Cosar CB, et al. Clinical and histopathologic findings of iris nevus (Cogan-Reese) syndrome. Acta Ophthalmol Scand 1999;77: 234-237.
11. Teichmann KD, Karcioglu ZA. Melanocytoma of the iris with rapidly developing secondary glaucoma. Surv Ophthalmol 1995;40:136-144.
12. Bataille V, Sasieni P, Cuzick J, et al. Risk of ocular melanoma in relation to cutaneous and iris naevi. Int J Cancer 1995;60:622-626.
13. Grossniklaus HE, Oakman JH, Cohen C, et al. Histopathology, morphometry, and nuclear DNA content of iris melanocytic lesions. Invest Ophthalmol Vis Sci 1995;36:745-750.
14. Carlson DW, Alward WL, Folberg R. Aggressive nevus of the iris with secondary glaucoma in a child. Am J Ophthalmol 1995;119:367-368.
15. van Klink F, de Keizer RJ, Jager MJ, et al. Iris nevi and melanomas: a clinical follow-up study. Doc Ophthalmol. 1992;82:49-55.
16. Paridaens D, Lyons CJ, McCartney A, et al. Familial aggressive nevi of the iris in childhood. Arch Ophthalmol 1991;109:1552-1554.
17. Sneed SR, Vine AK. Spontaneous collapse of a primary iris cyst associated with an iris nevus. Arch Ophthalmol 1991;109:21-22.
18. Workman DM, Weiner JW. Melanocytic lesions of the iris—a clinicopatho-logical study of 100 cases. Aust N Z J Ophthalmol 1990;18:381-384.
19. Biswas J, D’Souza C, Shanmugam MP. Diffuse melanotic lesion of the iris as a presenting feature of ciliary body melanocytoma: report of a case and review of the literature. Surv Ophthalmol 1998;42:378-382.
20. Shields JA, Augsburger JJ, Bernardino V Jr, et al. Melanocytoma of the ciliary body and iris. Am J Ophthalmol 1980;89:632-635.
21. Cialdini AP, Sahel JA, Jalkh AE, et al. Malignant transformation of an iris melanocytoma. A case report. Graefes Arch Clin Exp Ophthalmol 1989;227:348-354.
22. Nakazawa M, Tamai M. Iris melanocytoma with secondary glaucoma. Am J Ophthalmol 1984;97:797-799.
23. Hodes BL, Gildenhar M, Choromokos E. Fluorescein angiography in pigmented iris tumors. Arch Ophthalmol 1979;97:1086-1088.
24. Shields CL, Shields JA, Shields MB, et al. Prevalence and mechanisms of secondary intraocular pressure elevation in eyes with intraocular tumors. Ophthalmology 1987;94:839-846.
25. Michelson JB, Shields JA. The relationship of iris nevi to posterior uveal melanoma. Am J Ophthalmol 1977;83:694-696.
26. Nordlund JR, Robertson DM, Herman DC. Ultrasound biomicroscopy in management of malignant iris melanoma. Arch Ophthalmol 2003;121: 725-727.
27. Shields JA, Karan DS, Perry HD, et al. Epithelioid cell nevus of the iris. Arch Ophthalmol 1985;103:235-7.
28. Demirci H, Mashayekhi A, Shields CL, et al. Iris melanocytoma: clinical features and natural course in 47 cases. Am J Ophthalmol 2005;139:468-475.
29. Shields JA, Shields CL, Eagle RC Jr. Melanocytoma (hyperpigmented magnocellular nevus) of the uveal tract. The 34th G. Victor Simpson Lecture. Retina 2007;27:730-739.
▪ Iris Freckle and Iris Nevus: Pigmented Variations
 Figure 2.1. Multiple iris freckles. The freckle does not efface or alter the normal iris architecture. |
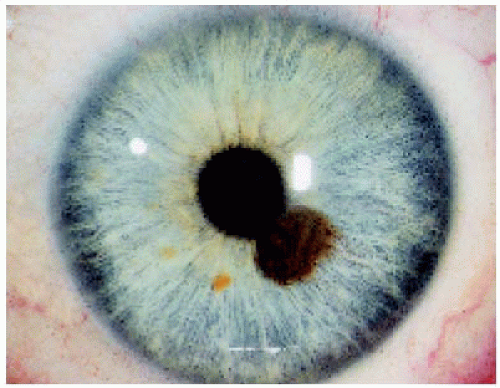 Figure 2.2. Iris nevus adjacent to the pupil in a 69-year-old woman. |
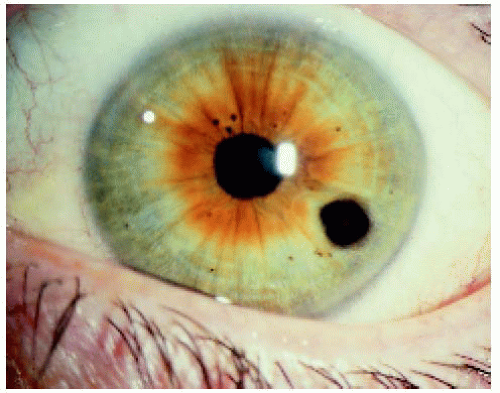 Figure 2.3. Iris nevus in the midportion of the iris in a 40-year-old woman. |
 Figure 2.4. Slightly larger iris nevus in the inferonasal quadrant of the left iris in a middle-aged woman. |
 Figure 2.5. Sector inferior iris nevus in a 39-year-old man. Most such sector nevi are noted at birth or shortly thereafter and may represent a localized variation of ocular melanocytosis. |
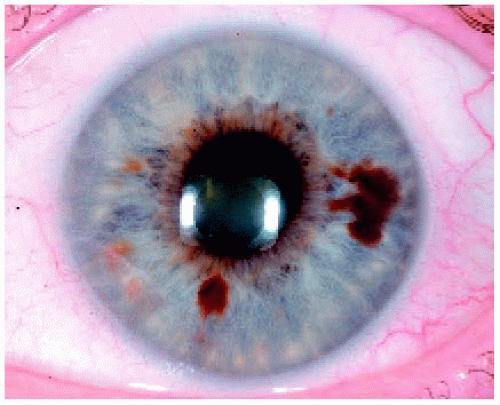 Figure 2.6. Two pigmented iris nevi in same eye. Note that there are also several iris freckles. |
▪ Iris Nevus: Nonpigmented and Minimally Pigmented Variations
The nonpigmented or minimally pigmented iris nevus can resemble a leiomyoma, metastatic carcinoma, lymphoma, and other nonpigmented iris lesions. The term nonpigmented is used here for simplicity, even though some may contain slight pigmentation. Selected examples are illustrated.
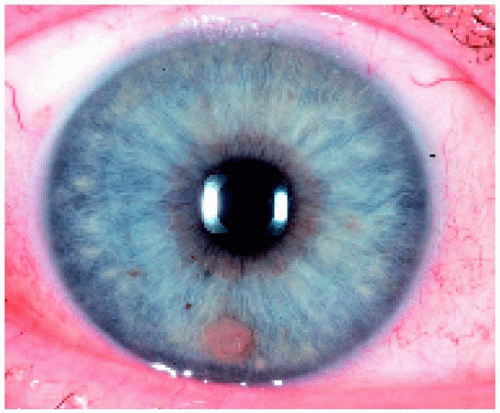 Figure 2.7. Circumscribed nonpigmented iris nevus in the inferior aspect of the iris stroma. |
 Figure 2.8. Very subtle nonpigmented iris nevus in peripheral iris inferotemporally. An unrelated pterygium is present nasally. |
 Figure 2.9. Nonpigmented iris nevus inferior between the 6 and 7 o’clock positions. Note the peaking of the pupil inferiorly and slight ectropion iridis. |
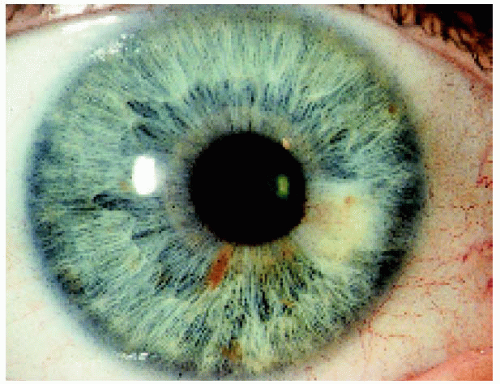 Figure 2.10. Nonpigmented iris nevus adjacent to the pupil in the left iris. |
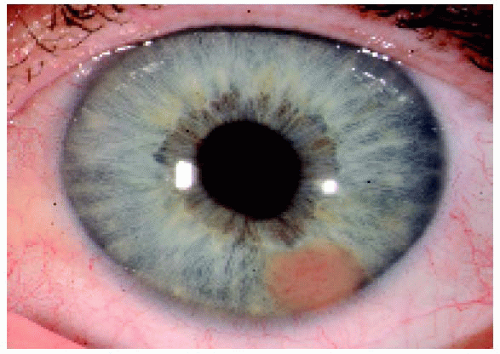 Figure 2.11. Nonpigmented peripheral nevus at the 5 o’clock position in the left iris. |
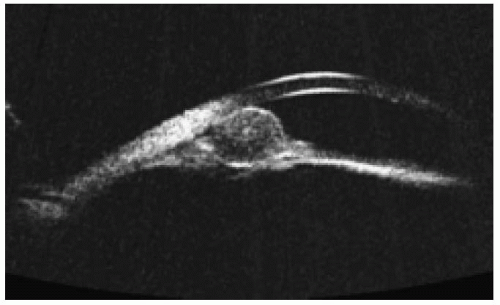 Figure 2.12. Ultrasound biomicroscopy of the lesion shown in Figure 2.11. Note the thickening of the peripheral iris and angle structures and relatively low internal reflectivity in the round mass. |
▪ Iris nevus: Effects on Adjacent Structures
Iris nevi can distort the adjacent pupil, involve the anterior chamber angle, produce a secondary cataract or a secondary cyst, and even demonstrate transcleral involvement. Such findings can occur with a nevus and do not necessarily indicate that the lesion is malignant.
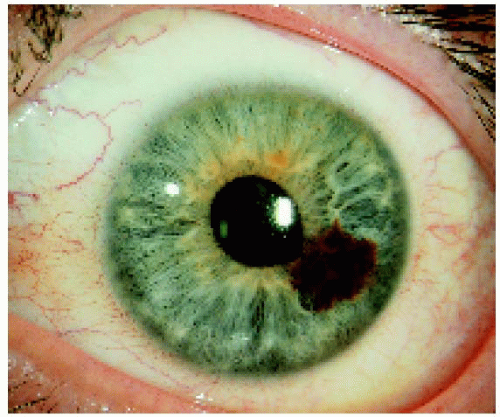 Figure 2.13. Peaking of the pupil secondary to an iris nevus in a 32year-old man. |
 Figure 2.14. Ectropion of the pupillary margin secondary to a sector iris nevus in a 48-year-old man. |
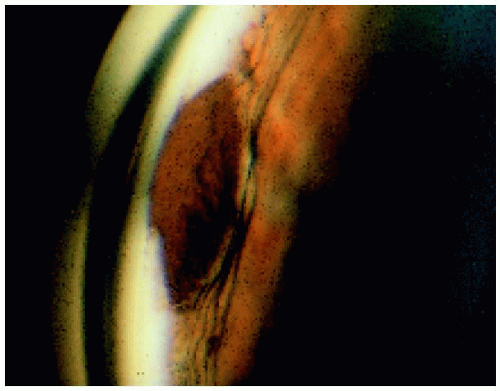 Figure 2.15. Gonioscopic view showing a peripheral iris nevus that affects the angle structures and stops abruptly at Schwalbe’s line. |
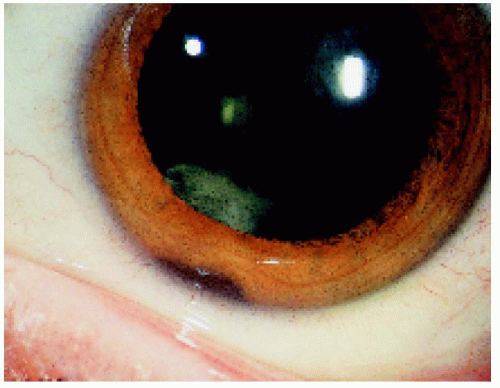 Figure 2.16. Sector cortical cataract secondary to a peripheral iris nevus. Such a cataract can occur with an iris nevus, but transillumination, gonioscopy, and ultrasound biomicroscopy can be used to exclude involvement of the ciliary body. |
 Figure 2.17. Slit lamp view of an iris nevus with a secondary cyst of the iris pigment epithelium posterior to an iris nevus. Such a cyst should not be misinterpreted as a malignant melanoma or a cystoid cavity within a melanoma. |
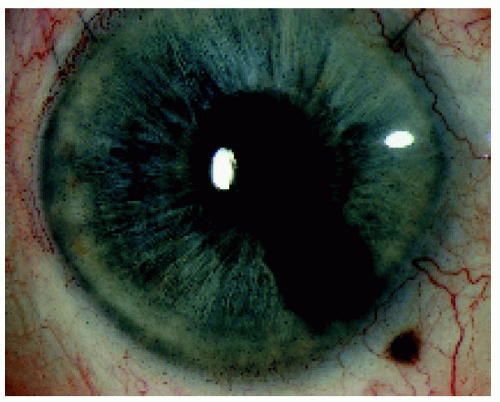 Figure 2.18. Iris nevus with transcleral involvement. Such a finding does not necessarily mean that the tumor has invaded through the sclera. It may be a transcleral component of a congenital nevus and not an extraocular extension of malignant melanoma. |
▪ Iris Melanocytoma
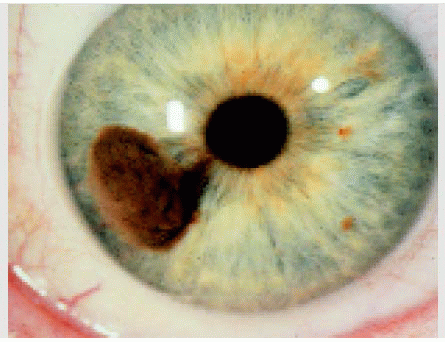
Melanocytoma is a deeply pigmented variant of melanocytic nevus. Although most are stable, some can show very slow growth and tumor seeding, similar to melanoma.
 Figure 2.19. Deeply pigmented presumed iris melanocytoma inferotemporally in the right eye in a young man as seen in 1972. |
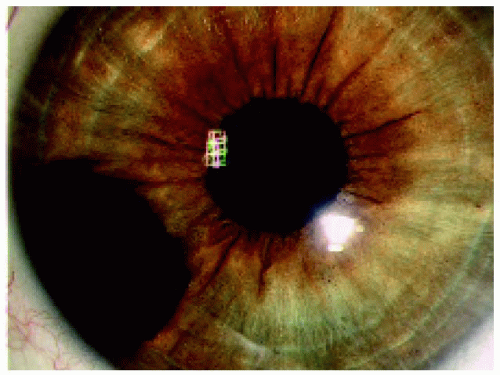 Figure 2.20. Same lesion in 2005, showing slight growth. The patient elected no treatment because growth was minimal for 33 years at the time of this writing. |
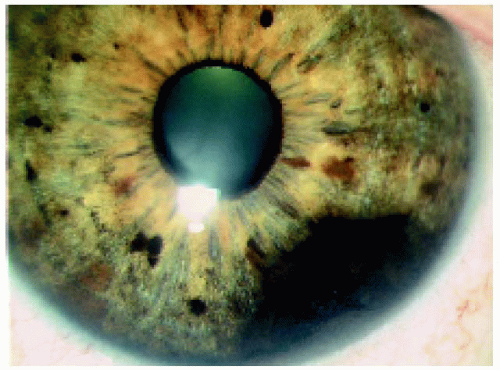 Figure 2.21. Friable iris melanocytoma with anterior chamber seeds. A fine needle aspiration was done, and the cytopathologic diagnosis was melanocytoma. The patient is being followed closely because of possibility of potential for secondary glaucoma, malignant transformation, and sampling error on needle biopsy. |
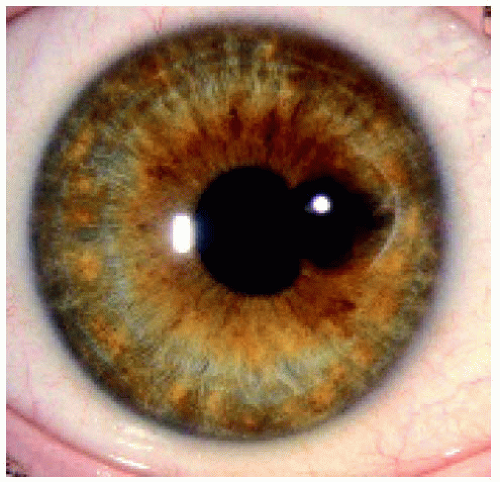 Figure 2.22. Melanocytoma near pupillary margin. The elevated lesion has a dark brown color and a rough, mossy appearance. It was removed by sector iridectomy. |
 Figure 2.23. Histopathology of the lesion shown in Figure 2.22, demonstrating dense cytoplasmic melanin that precludes a view of cell detail. (Hematoxylin-eosin × 150.) |
 Figure 2.24. Bleached section of the lesion shown in Figure 2.23, allowing better visualization of cell detail and features of melanocytoma. (Hematoxylin-eosin × 75.)
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|