CHAPTER 90 Mechanisms of Normal and Abnormal Swallowing
Stages of Normal Deglutition
Swallowing is a complex neuromuscular function involving structures in the oral cavity, pharynx, larynx, and esophagus. Various researchers have divided normal swallowing into four stages: the oral preparatory stage, the oral stage, the pharyngeal stage, and the esophageal stage.1–5 The first two stages, the oral preparatory and the oral, are under voluntary control, whereas the second two stages, the pharyngeal and esophageal, are involuntary, being under reflexive control.6,7 The oral stage of swallow is under voluntary control, whereas the pharyngeal swallow is no longer considered a reflex but rather a programmed activity; the motor program varies with the characteristics of the food being swallowed (i.e., the bolus), voluntary control, and other as yet undefined parameters.
Voluntary Stages of the Swallow
Oral Preparatory Stage
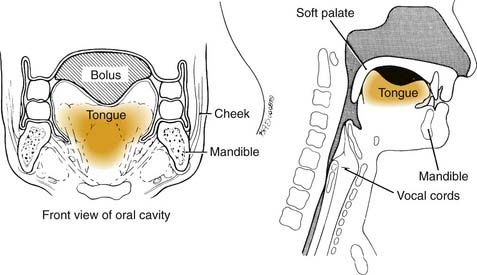
The oral preparatory aspect of deglutition, which prepares food for the swallow, involves the coordination of (1) lip closure to hold food in the mouth anteriorly, (2) tension in the labial and buccal musculature to close the anterior and lateral sulci, (3) rotary motion of the jaw for chewing, (4) lateral rolling motion of the tongue to position food on the teeth during mastication, and (5) bulging forward of the soft palate to seal the oral cavity posteriorly and widen the nasal airway.4 The forward position of the soft palate is not present during active chewing, and premature spillage while chewing is common and normal in people of all ages. Much of this coordination requires cerebellar input.8 The oral phase of deglutition is mechanical in that it involves the reduction of solid food to a pulverized consistency that may be easily swallowed. The most important neuromuscular function involved in the oral preparatory phase is the lateral rolling motion of the tongue.9 Without normal range-of-tongue motion, the manipulation and mastication of food during the oral preparatory phase would be impossible. At the termination of the oral preparatory phase, the tongue pulls the food together into a ball or bolus and holds it in a cohesive fashion on the floor of the mouth or against the hard palate (Fig. 90-1) in preparation for the beginning of the oral phase of the swallow.4,7,10–13
Oral Stage
The oral stage of the swallow is also a mechanical, voluntary stage and is designed to move food from the front of the oral cavity to the pharynx, wherein the pharyngeal stage of swallow is initiated. Again, tongue motion is the most critical element in this phase of the swallow because the tongue shapes, lifts, and squeezes the bolus upward and backward along the hard palate until the food reaches the pharynx.14–17 During this posterior propulsion by the midline of the tongue, the lateral margins of the tongue are sealed against the alveolar ridge, providing resistance against which the midline of the tongue propels the bolus.15 Tension in the buccal musculature is also thought to contribute to propelling the bolus backward, but to a much lesser degree than tongue movements.18 When the head or leading edge of the mandible crosses the tongue base, the pharyngeal swallow should be triggered in healthy people of all ages (Fig. 90-2). The pharyngeal swallow is usually triggered by the glossopharyngeal nerve (C9). In healthy people, the oral stage lasts no more than 1 to 1.5 seconds and is slightly prolonged with increasing age and with increasing viscosity of the bolus swallowed.5,19
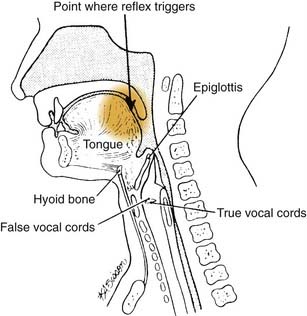
Figure 90-2. The lateral view of the head and neck illustrating the normal point at which swallowing reflex triggers.
In animal studies and in healthy humans, the pharyngeal swallow has been found to be triggered not only from C9 but also from the superior laryngeal nerve at the inlet of the larynx.20–25 Normal swallowing does not use this secondary mechanism for triggering the pharyngeal swallow because food would have almost entered the airway by the time the pharyngeal swallow was triggered. Thus when videofluoroscopic examination of a patient shows that the pharyngeal swallow triggers late, as food is about to enter the airway or after the bolus has come to rest in the valleculae or pyriform sinuses, the patient is said to have a disorder of swallowing called a delayed triggering of the pharyngeal swallow.
Programmed Stages of the Swallow
Pharyngeal Stage
The pharyngeal swallow is mediated in the lower brainstem (the medulla) in the reticular formation immediately adjacent to the respiratory center. Coordination exists between these two centers because respiration ceases for a fraction of a second when the airway closes during the pharyngeal swallow. There is also cortical input to the triggering of the pharyngeal swallow through the tongue movement patterns in the oral phase of the swallow.20 The exact neurologic substrate for this cortical input is not clearly understood.26
Neuromuscular Activities Characteristic of the Pharyngeal Swallow
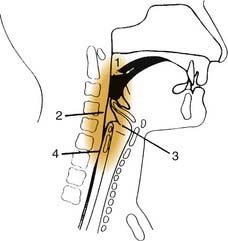
When the swallowing reflex is triggered, the brainstem swallowing center programs five neuromuscular activities to occur (Fig. 90-3). If triggering of the pharyngeal swallow is delayed, none of these neuromuscular activities occurs until pharyngeal swallow triggers (1) velopharyngeal closure to prevent backflow of material up the nose; (2) tongue base retraction to propel the bolus through the pharynx; (3) pharyngeal contraction to clear residue through the pharynx; (4) airway protection, which involves both elevation and closure of the larynx; and (5) cricopharyngeal or upper esophageal sphincter (UES) opening to allow the bolus to pass into the esophagus.1,2,27–33
Velopharyngeal closure and hyoid and laryngeal elevation occur as the first response to triggering the pharyngeal swallow. Then laryngeal closure occurs, followed closely by opening of the cricopharyngeal sphincter. These neuromuscular functions also overlap but do not all last for the entire pharyngeal stage of the swallow. Instead, each lasts only as long as the bolus is passing that part of the pharynx. When the bolus has reached the middle to lower pharynx, the soft palate lowers. At that time, the larynx is closed and elevated and the upper esophageal sphincter is open, preventing the passing bolus from entering the airway and allowing it to enter the esophagus. The duration of the pharyngeal stage of the swallow normally lasts a maximum of 1 second and does not vary dramatically with the consistency of food or age or gender of the patient.5,19
Airway Protection
Airway protection, as noted previously, involves two dimensions: elevation and closure. Elevation is created by contraction of strap musculature, which positions the larynx upward and forward under the tongue base as it is retracted at the end of the oral phase of the swallow. The larynx is pulled up and out of the way of the passage of the food bolus over the base of the tongue. Closure of the larynx involves three sphincters: the epiglottis and aryepiglottic folds, the false vocal folds and airway entrance, and the true vocal folds.27,28,34–36 The relative importance of each of the three sphincters has been debated in the literature.35,37,38 Most authors agree that the epiglottis and aryepiglottic folds play a relatively minor role in protecting the airway; their purpose is to divert food around the airway. The most important level of closure, airway entrance closure, is maintained only for the fraction of a second that the bolus is passing the airway.
Cricopharyngeal (Upper Esophageal Sphincter) Opening
The cricopharyngeus muscle acts in opposition to the function of the constrictor mechanism of the pharynx. At rest the constrictors are relaxed, and the cricopharyngeus muscle or upper esophageal sphincter is in tonic contraction to prevent air intake into the esophagus concurrent with inhalation into the lungs. Also, the contracted cricopharyngeus muscle prevents backflow from the esophagus into the pharynx.1 During the swallow, as the constrictor mechanism is contracting, the cricopharyngeus muscle relaxes at the appropriate moment. The anterior superior movement of the larynx opens the UES, and the bolus passes into the esophagus. The duration of UES opening and airway closure increases as bolus volume increases.39
Pharyngeal Pressure Generation: Tongue Base Retraction and Pharyngeal Contraction
When the tail of the bolus reaches the tongue base, the tongue base moves rapidly backward like a piston, increasing pressure in the pharynx. As the tongue base moves backward, the lateral and posterior pharyngeal walls at the tongue base level move inward. The tongue base and pharyngeal walls should make complete contact. Electromyographic and radiographic studies have shown that pharyngeal contraction, or the squeezing action of the constrictor mechanism to move the bolus through the pharynx, occurs sequentially, beginning in the superior constrictor muscle and moving through the medial to the inferior constrictor muscle.29,40
Pharyngeal contraction is responsible for clearing material from the pharyngeal walls and pyriform sinuses. When residue or material remains in the valleculae after the swallow, it is interpreted as a symptom of reduced tongue base movement.41 Tongue base movement occurs later as bolus volume increases.
Esophageal Stage
When the bolus has passed through the UES, the esophageal phase of swallow begins. The esophageal stage has greater variability in duration than the other stages of the swallow. Normal esophageal transit may vary from 8 to 20 seconds.4 The upper third of the esophagus is composed of mixed voluntary and involuntary muscle, and the lower two thirds is composed entirely of involuntary muscle. The lower esophageal sphincter acts as a valve to the stomach, which must open in time to allow the bolus to pass from the esophagus into the stomach.
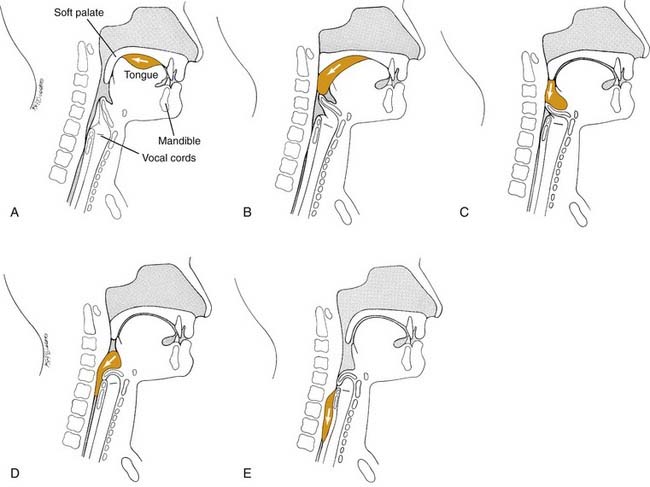
Figure 90-4 illustrates the progression of the bolus through the pharynx. If an anatomic or neuromuscular disorder affects the pharyngeal stage of the swallow, aspiration may result.
Signs and Symptoms of Abnormal Swallow
Aspiration (Coughing, Choking)
Aspiration is the entry of material into the airway below the true vocal folds. The effect of chronic aspiration in adults is not well understood, but in the long term it may result in pneumonia or pulmonary changes. Patients who are observed to aspirate on a radiographic study of swallowing are at significantly greater risk of pneumonia developing than patients who do not show aspiration on such a study. Many patients with head and neck cancer who have chronic aspiration do not survive long enough to experience the long-term effects of their aspiration. Aspiration may occur before, during, or after the pharyngeal swallow.4 Aspiration that occurs before the pharyngeal swallow may result from one of two disorders: reduced tongue control or a delayed or absent pharyngeal swallow. When tongue control is reduced during the oral preparatory or oral stages of the swallow, bits and pieces of food may fall into the pharynx and the open airway as the patient chews. Importantly, the airway is normally open during the oral preparatory and oral stages of the swallow. The airway is closed only for a fraction of a second during the pharyngeal swallow. Aspiration before the swallow can also occur because of a delayed or absent pharyngeal swallow. In these patients, the food is propelled out of the oral cavity by the tongue and falls into the pharynx, wherein it may come to rest in the valleculae, the pyriform sinus, or the airway before the pharyngeal swallow is triggered. The entry of food into the airway does not always trigger a cough, particularly in neurologically impaired patients and some patients with head and neck cancer in whom sensory input is damaged.41,42
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


