CHAPTER 142 Mastoidectomy
History
The first scholarly treatise on mastoid surgery for suppurative disease was by Schwartze in 1873.1,2 The procedure he described was a cortical mastoidectomy with limited exenteration of mastoid air cells. For acute and coalescent mastoiditis, which were prevalent in the preantibiotic era, this procedure proved remarkably efficacious. As one might expect, however, the simple mastoidectomy rarely cured chronic otitis media or cholesteatoma. During the next 20 years, it became evident that creating an open cavity was necessary for these diseases, and in 1890, Zaufal described removing the superior and posterior canal wall, tympanic membrane, and lateral ossicular chain, a procedure now known as the radical mastoidectomy.3 This procedure was modified by Bondy, who recognized that disease limited to the pars flaccida could simply be exteriorized, leaving the uninvolved middle ear alone. His description of the “modified radical mastoidectomy” or “Bondy procedure” in 1910 represented one of the first reports addressing hearing function.1
Interest in hearing preservation and restoration gained further attention after Lempert introduced the fenestration operation in 1938, and Zollner and Wullstein described tympanoplasty techniques in the early 1950s.4–6 During the next decade, Jansen, Sheehy, and others extended these principles of restoring function and maintaining normal anatomy with the introduction of the intact canal wall mastoidectomy with facial recess approach.7,8
Anatomy
The temporal bone consists of four parts: squamous, tympanic, mastoid, and petrous (Figs. 142-1 and 142-2). The smallest part is the tympanic portion, which forms the external auditory canal. This chapter focuses primarily on the mastoid portion, which articulates with the parietal and occipital bones and houses the mastoid air cell system, which is in continuity with the air cells of the petrous pyramid. Transmastoid procedures provide access to the facial nerve, internal carotid artery, jugular bulb, labyrinth, internal auditory canal, and petrous apex.
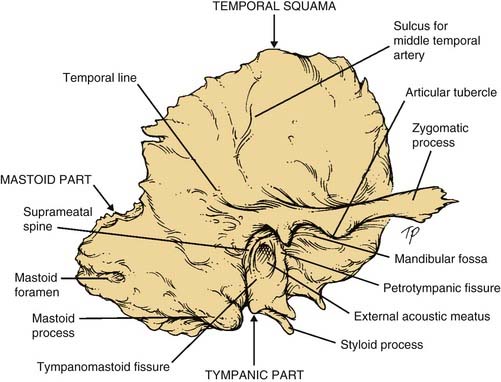
Figure 142-1. Right temporal bone. Lateral view.
(From Donaldson JA, Duckert LG, Lambert PR, Rubel EW, eds. Surgical Anatomy of the Temporal Bone. 4th ed. New York: Raven Press; 1992.)
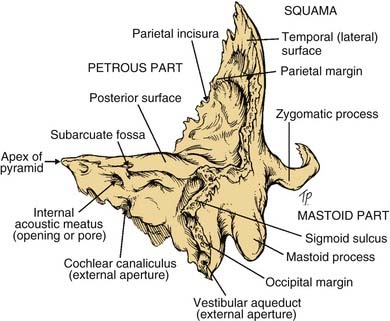
Figure 142-2. Left temporal bone. Posterolateral view.
(From Donaldson JA, Duckert LG, Lambert PR, Rubel EW, eds. Surgical Anatomy of the Temporal Bone. 4th ed. New York: Raven Press; 1992.)
Nomenclature
The otologic surgeon has various mastoid procedures from which to choose, depending on extent of disease. In addition, variations on these standard approaches are often discussed in the literature. The nomenclature for mastoid surgery can seem confusing at first. Concomitant surgery involving the middle ear requires additional terminology, such as tympanoplasty or ossiculoplasty. Box 142-1 lists the standard mastoid procedures for addressing chronic ear disease.
Operative Procedure (see Key Indicator Video on website)
The surgical site is prepared by shaving 1 to 2 cm of hair around the ear and injecting 5 to 10 mL of local anesthetic with a vasoconstrictor (e.g., 1% lidocaine with 1 : 100,000 epinephrine) postauricularly and within the external ear canal. To facilitate closure, the C-shaped incision is placed about 1 cm behind the postauricular crease, rather than within it (Fig. 142-3). If extensive saucerization of the mastoid cavity is planned (e.g., translabyrinthine or retrolabyrinthine approach to the cerebellopontine angle, skull base tumor resection), the incision is placed more posteriorly.

Figure 142-3. Postauricular incision is placed about 1 cm behind the postauricular crease, facilitating skin closure.
(From Sheehy JL. Surgery of chronic otitis media. In: English GE, ed. Otolaryngology. Philadelphia: Lippincott; 1986:1.)
With the mastoid cortex fully exposed, the first bur cut is made along the temporal line, which approximates the level of the middle cranial fossa dural plate. It is important to recognize, however, the variability of the position of the tegmen, depending on the degree of mastoid pneumatization. The second bur cut is made perpendicular to this and tangential to the external bony canal; it should be carried inferiorly to the mastoid tip (Fig. 142-4).
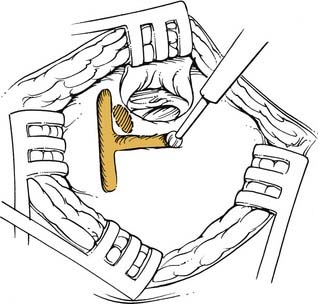
Figure 142-4. Initial bur cuts are along the temporal line and tangential to the bony canal.
(From Sheehy JL. Mastoidectomy: the intact canal wall procedure. In: Brackmann DE, Shelton C, Arriaga MA, eds. Otologic Surgery. Philadelphia: Saunders; 1994.)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


