Chapter 17 Mastoidectomy—Canal Wall Down Procedure
 Videos corresponding to this chapter are available online at www.expertconsult.com.
Videos corresponding to this chapter are available online at www.expertconsult.com.
There are two approaches to mastoidectomy in patients with cholesteatoma and chronic otitis media. The canal wall up (also known as intact canal wall) technique is discussed in detail in Chapter 16. This chapter describes the technique for canal wall down surgery. Related topics discussed in this chapter include the role of atticotomy, mastoid obliteration procedures, reconstruction of canal wall down cavities that have not been previously reconstructed, management of dural venous sinus injury during chronic ear surgery, and facial nerve monitoring in chronic ear surgery.
DEFINITIONS
INDICATIONS FOR CANAL WALL DOWN MASTOIDECTOMY
Some authors have argued that canal wall down surgery permits excision of cholesteatoma in the sinus tympani region.1 Anatomically, this is not full visualization because the depths of the sinus tympani are medial to the facial nerve. Nonetheless, Hulka and McElveen2 showed that canal wall down procedures do permit additional visualization in the anterior epitympanum and sinus tympani region. The latter is not fully visualized with any technique. Another relative indication for canal wall down mastoidectomy is failure of previous canal wall up procedures with recurrent cholesteatoma from epitympanic retraction pockets. The anatomy of a canal wall down mastoidectomy with full exteriorization of the epitympanum makes retraction pocket recurrences of cholesteatoma unlikely because the whole epitympanum has been exteriorized. Although the use of Silastic in canal wall up facial recess surgery and staging has been significant in reducing the incidence of recurrent cholesteatoma with canal wall up surgery, the presence of a scutal edge and a distinct epitympanum in cases with persistent eustachian tube dysfunction can produce recurrent cholesteatoma.
SURGICAL TECHNIQUES
Patient Preparation
As mentioned previously, the decision to convert a mastoid operation from canal wall up to canal wall down is usually made intraoperatively. The usual steps for tympanoplasty with mastoidectomy surgery would have been accomplished, including canal incisions, as described in the chapters on tympanoplasty (undersurface graft Chapter 12 and lateral graft Chapter 9). The ear has been reflected forward, the middle ear work has been completed, the tympanic membrane remnant has been prepared for grafting, and the mastoidectomy has begun.
Basic Techniques
Adequate Saucerization
Removal of bone from the edges of the mastoid defect saucerizes or bevels the edges of the defect so that there is no overhanging bone obstructing the wider cavity below (Fig. 17-1). This saucerization ensures that there is no disease tissue laterally. Also, saucerization permits soft tissue surrounding the mastoid to slide into the defect. Paradoxically, removing additional bone around the margins of the mastoid cortex in this saucerization step actually makes a smaller cavity rather than a larger cavity.
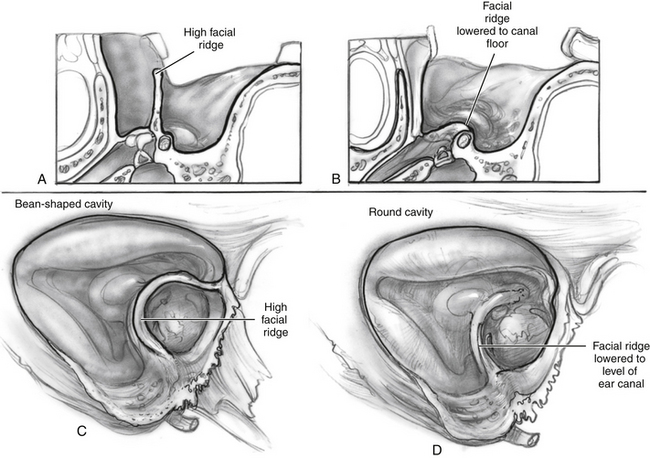
Adequate Lowering of the Facial Ridge
The boundary between the EAC and the mastoid cavity is defined by the height of the facial nerve. Leaving excessive bone overlying the facial nerve (facial ridge) between the EAC and the mastoid cavity creates a situation in which there is a deep trough on the mastoid side (Fig. 17-2). This high ridge is sometimes referred to as a “beginner’s hump.” Occasionally, novice mastoid surgeons leave a large ridge of bone overlying the facial nerve for fear of injuring it. This ridge creates a difficult situation postoperatively with trapped mastoid spaces that are hard to clean in the office, and it prevents natural cleaning. The surgeon should lower the ridge of bone overlying the facial nerve so that the fallopian canal is barely visible with a thin amount of bone overlying the vertical segment of the facial nerve.