Chapter 15 Management of the Patient with Anaphylaxis
Introduction
The first documented case on possible anaphylaxis in humans occurred in 2640 Bc. Hieroglyphics suggest that the Egyptian pharaoh Menes may have died from a wasp sting.1 Anaphylaxis is a term first used by Richet and Portier in 1902. During attempts to immunize dogs to sea anemone venom, fatal reactions occurred using doses that previously were tolerated. The Greek term “phylaxis” means protection and “ana” translates into backwards. Since the fatal reactions were the opposite of the “phylaxis” they were trying to achieve, they used the term anaphylaxis to describe the opposite of protection.2 Unfortunately, a universally accepted definition of anaphylaxis still does not exist, and the point at which a severe “allergic reaction” becomes anaphylaxis remains unclear. This lack of a clear entity can cause confusion when examining medical literature or attempting to learn more about anaphylaxis. In the allergy treatment setting, the term “systemic reaction” is commonly used in place of “anaphylaxis.” This lack of a universal classification system limits our knowledge concerning the prevalence of this problem, contributes to its underrecognition by health care professionals, and probably results in the undertreatment of anaphylactic episodes.
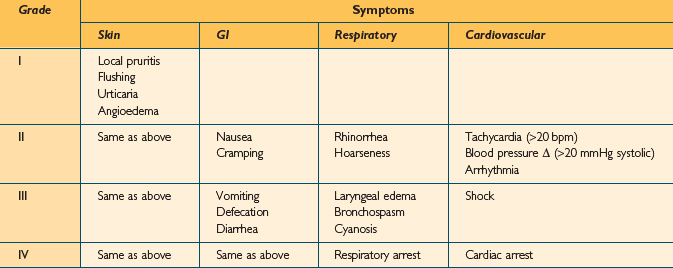
In an attempt to improve communication concerning the understanding of anaphylaxis, several authors have developed severity grading scales. Unfortunately, no single system has proven more useful than another, and none is universally accepted.3 Grading scales may be useful, however, especially when communicating among doctors, reporting results, or analyzing treatment options. One such grading scale is shown in Table 15.1. In Ring and Messner’s classification, grade I anaphylaxis is characterized by cutaneous manifestations and angioedema. In grade II anaphylaxis, milder respiratory and cardiovascular effects are noted. With grade III anaphylaxis, there is severe multisystem involvement, and finally, in grade IV, anaphylactic death is imminent. A similar, but simpler grading system was developed by Brown. In this system, anaphylaxis is divided into mild (generalized erythema, urticaria, periorbital edema, or angioedema), moderate (dyspnea, stridor, wheeze, nausea, vomiting, dizziness, diaphoresis, chest or throat tightness, or abdominal pain), and severe (hypoxia, hypotension, neurologic compromise, cyanosis, confusion, collapse, loss of consciousness, incontinence).4
Etiology
A large variety of agents are capable of eliciting anaphylactic reactions. By definition, IgE-mediated anaphylaxis requires prior exposure and sensitization. Non-IgE-mediated (anaphylactoid) reactions do not require antigen processing or prior exposure. Common causes of anaphylaxis are foods, drugs, insect venoms, and immunotherapy (IT) (Box 15.1), with foods appearing to be the most common cause.5 Of foods, the usual culprits are tree nuts, peanuts, milk, eggs, soy, wheat, shellfish, and fish. As for drugs, the most common instigators for anaphylaxis include beta lactam antibiotics, anesthetic drugs, opioid analgesics, radiocontrast media, NSAIDs, and aspirin. Drug reactions in the operating room are also possible. In the perioperative period and during medical procedures, the risk of anaphylaxis is somewhere between 1 in 4500 and 1 in 25 000, with a fatality rate between 3% and 6%. The most common agents implicated in surgical procedures are muscle relaxants and latex.6 Exercise can also cause anaphylaxis.7 Finally, a likely cause for anaphylaxis cannot be found for many episodes, and these cases are considered idiopathic.
Epidemiology
The epidemiology of anaphylaxis is incompletely understood due to the variability in case definition and differences in methodology. Additionally, many cases of anaphylaxis are probably never diagnosed. With these caveats, a fairly broad description of the incidence and etiologies of anaphylactic and anaphylactoid reactions is possible. Yocum et al studied the incidence of anaphylaxis in a defined population in Olmstead County, Minnesota over a 5-year period and found an average annual incidence of 21 cases per 100 000 persons per year. The case fatality rate was 0.65%.8 Analysis of data from multiple countries yielded an incidence rate of 1–3 cases of severe anaphylaxis per 10 000 people and a fatal anaphylaxis rate of 1–3 per million people. These rates included anaphylaxis from all causes.9 It is estimated that 1.24–16.8% of the US population may suffer an anaphylactic reaction, and 0.002% may die. It is has been reported that there are up to 1500 deaths per year in the USA from anaphylaxis.10
Neugut et al published a review of anaphylaxis in the USA.10 Several points of interest can be found in that text about the various etiologies of anaphylaxis. Approximately 1% of the US population suffers from food allergies, and approximately 0.0004% of the population has a severe allergic or anaphylactic reaction each year, with about 100 deaths per year. Penicillin is the most common drug that causes anaphylaxis, and one report suggests that penicillin causes approximately 75% of all fatal anaphylactic cases in the USA each year. Penicillin causes fatal anaphylaxis at a rate of 0.002% among the general population (about 500–1000 deaths per year), and nonfatal penicillin-induced anaphylaxis may occur in 0.7–10% of the population taking penicillin. Radiocontrast media causes anaphylactoid reactions in 0.22–1% of exposures. Newer nonionic contrast media have lower rates however. Latex allergy has become more common over the last few decades, mostly due to the increasing use of latex gloves for universal precautions in the health care setting. The annual incidence of latex-induced anaphylactic reactions is estimated to be 220 per year. Stinging insects, especially those in the hymenoptera, are common causes of anaphylaxis. These insects include bees, wasps, hornets, and ants. Anaphylaxis from hymenoptera stings may occur in 0.5%–5% of stings, resulting in approximately 40–100 deaths per year in the USA. On subsequent stings, individuals who have had an anaphylactic reaction have a 30–60% chance of another anaphylactic reaction. In patients who receive venom immunotherapy this risk decreases to 3%.
One of the greatest risk factors for anaphylaxis appears to be atopy.8,11 Atopic patients are also at greater risk for anaphylactoid reactions (such as those from radiocontrast media, for example), even though these reactions are not necessarily IgE mediated. It is postulated that increased production of interleukin (IL) 4, IL-5, and IL-13 may make the atopic patient prone to mast cell mediator release, as these cytokines have effects on mast cell degranulation.11 Although anaphylaxis seems most common in adults, incidence varies in different age groups based on the various triggers. Gender may play a role as well, as anaphylaxis is more common in males under 16 and females over 30.11 Asthma is also a significant risk factor for anaphylaxis, and asthmatics may be more prone to respiratory involvement in anaphylactic episodes.
Probably the greatest concern of the clinical allergist, with regard to anaphylaxis, is the occurrence of anaphylactic responses to antigen immunotherapy. Unfortunately, as mentioned above, the allergy patient is at higher risk for an anaphylactic response to injected antigen immunotherapy. In the allergy treatment setting, anaphylactic reactions are often referred to as “systemic reactions.” Subcutaneous antigen immunotherapy can be fatal, and proper practices are required to minimize risk to the patient. Information about the incidence of fatal reactions to immunotherapy injections is relatively sparse. In a study including 36 359 injections of specific antigen immunotherapy with aluminum-adsorbed vaccine, there was an incidence of serious systemic side effects in approximately 0.1% of all injections.12 All severe reactions occurred within 30 minutes of injection. Among these allergy patients, asthmatic subjects proved at higher risk for systemic reaction, with most episodes occurring during dose escalation. However, there was no risk associated with age, gender, degree of skin test reactivity, or allergen injected. Survey studies conducted by the American Academy of Allergy and Immunology (AAAI) revealed a total of 40 deaths after skin testing or immunotherapy in the period from 1945 to 1983, 17 immunotherapy-associated deaths from 1985 to 1989, 10 deaths from 1990 to 1991, and six deaths from 1992 to 1996. The risk of death in American patients receiving immunotherapy from 1985 to 1989 was estimated to be 1 for every 2 million injections. In 1997, the American College of Allergy, Asthma and Immunology (ACAAI) estimated that deaths from immunotherapy occurred at a rate of 0.67 per 1 million injections.13 Other studies from England and Germany in the 1980s seemed to show a spike in immunotherapy deaths attributable to new, higher potency, standardized extracts.13 In the US survey covering 1985 to 1989, 77% of fatalities occurred in patients with asthma, even though the vast majority of patients were being treated for rhinitis.13 In all of the survey studies, there was a high proportion of fatalities from those who suffered from asthma or whose asthma was steroid dependent or poorly controlled. This occurrence makes it clear that symptomatic or severe asthma is a risk factor for severe systemic reactions to immunotherapy. Another important point is that most fatal immunotherapy reactions occur during the dose escalation phase, rather than the maintenance phase, of immunotherapy. Similarly, there is an increased frequency of nonfatal systemic reactions during dose escalation. There is little information about the incidence of anaphylaxis using different dose escalation protocols. However, rushed protocols appear to be associated with an increased rate of systemic reactions.13
High levels of sensitivity to the injected allergen have been found in a large portion of fatal cases, but as mentioned previously, skin sensitivity does not necessarily predict systemic reactions. Fatal cases appear more likely during a patient’s allergy season. The European Academy of Allergology and Clinical Immunology (EAACI) and the American Academy of Allergy, Asthma and Immunology (AAAAI) practice parameters both recommend reducing the seasonal pollen doses administered during a patient’s pollen season. Beginning a new vial during immunotherapy is also a risk factor for systemic reactions and is associated with fatalities, probably because of variability in extract potency associated with lot-to-lot variation or mixing errors. In some studies, pollen and dust mite antigens are more likely to provoke a severe or fatal systemic reaction than hymenoptera venom immunotherapy,13 but whether particular antigens are more likely to provoke a systemic reaction is controversial. Venom immunotherapy, in which subjects have already suffered an anaphylactic reaction prompting their need for immunotherapy, is a special case. Rush protocols are often employed to yield protection as soon as possible. Perhaps because of the frequent use of rush protocols, the incidence of systemic reactions during hymenoptera venom immunotherapy may be as high as 35%.14 Depot allergens may be less likely to provoke a systemic reaction than aqueous extracts, but these allergens are not available in the USA.12 One important risk factor for a systemic reaction to an immunotherapy injection is a previous reaction to an immunotherapy injection.13 Patients who have had systemic reactions should have their dosage reduced on subsequent administration. Most severe systemic reactions after immunotherapy injections occur within 30 minutes, and patients who had systemic reactions should be observed for this length of time so that medical intervention can be promptly initiated, if necessary. Above all, it must be noted that human error is one of the greatest risk factors for fatal reactions to immunotherapy.13
The largest study concerned with the safety of allergy immunotherapy was conducted by a group of physicians in the American Academy of Otolaryngic Allergy.15 The study evaluated the overall safety of immunotherapy given in the office environment and at home. This study included 1144 000 injections given in the prescribing physician’s office, at home or in other physician’s offices. The overall minor reaction rate was 0.009%, while the rate of major reactions was 0.005%. There were no hospitalizations and no deaths. Due to proper selection of patients eligible for home injections, the rate of reactions was less in the home injection group compared to the office injection group. The study also identified risk factors for major reactions during immunotherapy. Table 15.2 lists the percentages of patients experiencing a major reaction who exhibited each risk factor in this study.
TABLE 15.2 Major risk factors for immunotherapy-related anaphylaxis
| Risk factor | % of major reactions associated with risk factor |
|---|---|
| Build up immunotherapy | 90 |
| Active asthma | 46 |
| New vial, first injection | 10 |
| Prior systemic reaction | 7 |
| Vial prepared in another office | 6 |
| Beta-blocker treatment | 4 |
| Error (wrong patient’s vial) | 3 |
Immunology and Pathophysiology
Systemic anaphylaxis results from the release of mast cell and basophil mediators in sufficient quantity to evoke a systemic response involving multiple end organs. Anaphylaxis begins when antigen cross-linking of receptor-bound IgE causes mast cell mediator release. The exact mechanisms and thresholds required to initiate anaphylaxis after sensitizing antigen exposure are uncertain. This IgE-mediated mechanism of anaphylaxis requires systemic distribution of the offending agent, hence parenteral or enteral exposures are common routes for anaphylactic reactions. The signs and symptoms elicited by mast cell mediator release depend on the organ system in which those mast cells reside: skin, gastrointestinal tract, respiratory tract, and cardiovascular system. Mast cells in perivascular locations can have a significant effect on hemodynamics. Other cell types, including basophils, monocytes, eosinophils, antigen presenting cells, and epithelial cells, may participate in this process and affect the duration and intensity of the reaction with their interactions and secreted products.
One of the most important mediators is histamine, which causes vasodilation, increased vascular permeability, mucous hypersecretion, smooth muscle spasm, and eosinophil chemotaxis and activation. Serum histamine levels correlate with the severity of cardiopulmonary manifestations and GI manifestations in anaphylaxis episodes.16 Histamine mediates its effects through H1 and H2 receptors. Histamine causes extravasation of blood volume and decreased peripheral vascular resistance. Tryptase, chymase, heparin, and other chemokines and chemotactic factors are also involved. These above mediators activate other inflammatory systems, but may also have an attenuating role in the chain reaction of inflammatory events in an anaphylactic episode.11
Mast cell degranulation products can activate other important biochemical pathways that contribute to an anaphylactic episode, like the kininogen–kallikrein system, coagulation cascade, and the complement cascade through the actions of tryptase.11 Tryptase, which is stored in mast cell secretory granules, can activate the kinin system, clotting cascade, and complement cascade.17 Levels of C4 and C3 decrease in anaphylaxis, and increases in C3a have been measured, suggesting that complement activation plays a role in the process. Factors V, XIII, and fibrinogen decrease with anaphylaxis, suggesting involvement of these systems in anaphylactic episodes.16 Nitric oxide production is dramatically increased in anaphylactic episodes. The net effect of nitric oxide production is vasodilation and increased vascular permeability.11 In addition to preformed mediator release from mast cells, newly generated lipid mediators, including leukotrienes (LT) B4, C4, D4, E4, platelet activating factor, prostaglandin D2, and others, are involved. LT B4 is chemotactic and may play a role in the late manifestations of anaphylaxis. Recurrent or biphasic anaphylaxis may be secondary to inflammatory cell activation and recruitment (like eosinophils) and may occur 12 hours after the initial attack.16
Anaphylaxis is primarily an IgE-mediated phenomenon, but can involve IgG or IgM antibodies.3 In mouse models of anaphylaxis, there is an IgG-dependent pathway that depends on the involvement of macrophages, which secrete platelet activating factor.18 Antigen–antibody complexes may activate complement and trigger “immune aggregate anaphylaxis,” and this mechanism is implicated in anaphylactoid reactions to protamine, dextran, and albumin.17
Some anaphylactoid reactions due to drugs, exercise, or physical factors may be due to direct release of mediators from mast cells. Aspirin- and NSAID-induced anaphylactoid reactions are due to altered arachidonic acid metabolism. It is thought that inhibited production of prostaglandin E (which prevents mast cell degranulation) and excess production of leukotriene C (which stimulates degranulation) is responsible for mediator release in NSAID-induced anaphylactoid reactions. Radiocontrast material may provoke anaphylactoid reactions by activating multiple systems, including the kallikrein–kinin, clotting system, and complement system.17 Non-IgE-mediated complement activation can occur from exposure to radiocontrast media, liposomal drug preparations, NSAIDs, and other drugs in a reaction now called CARPA (C activation-related pseudo-allergy). A CARPA reaction can occur on first exposure to an agent. In the case of radiocontrast media, the classical and alternative complement pathways are activated.19
Physiologic Changes in Anaphylaxis
The main cardiovascular clinical feature of anaphylaxis is hypotension. Anaphylactic hypotension is due to fluid extravasation and vasodilation, resulting in a mixed distributive-hypovolemic shock. There may be vasodilation, reversible cardiac depression, and paradoxically, bradycardia.20 In anaphylaxis, blood pressure declines and heart rate increases, but depleted intravascular volume leads to worsening cardiac output. While peripheral vascular resistance initially decreases, it may recover, perhaps due to endogenous epinephrine, angiotensin II, or endothelin.11 With anaphylaxis, massive fluid shifts occur that affect cardiovascular stability. There may be up to a 50% decrease in circulating blood volume as quickly as 10 minutes after the onset of symptoms.16
Anaphylactic shock is a severe and prolonged hypotension caused by mediators such as histamine and prostaglandins released by tissue mast cells and circulating basophils. These mediators cause vasodilation and increased capillary permeability. In addition to the hemodynamic effects mentioned, mediators of anaphylaxis directly affect the heart. H1 receptors can “mediate” coronary vasoconstriction, and H2 receptors can increase atrial and ventricular contractility, the sinoatrial node firing rate, and coronary artery dilation. Platelet activating factor decreases coronary blood flow and decreases cardiac output.16 Histamine and other mediator production are affected by beta-adrenergic neurohumoral mechanisms acting via cyclic AMP (adenosine monophosphate). Beta-blockade may increase the synthesis and release of anaphylactic mediators, increase the sensitivity of peripheral end organs, and in experimental anaphylaxis increase the risk of death.21 Beta-blockers prevent the salutary effects of epinephrine (adrenaline), when given in an anaphylactic emergency. Unopposed alpha-adrenergic stimulation from epinephrine may cause coronary constriction or exaggerate the systemic pressor effects of epinephrine. Finally, beta-blocker treatment may increase the risk of anaphylaxis up to threefold in patients receiving immunotherapy.21
In anaphylactic deaths, pathologic findings include laryngeal edema, mucous plugging and hyperinflated lungs, and myocardial damage. Also, a dilated right ventricle, eosinophilia in the pulmonary vessels and GI tract, as well as congestion of abdominal viscera are noted. These findings indicate that death from anaphylaxis is usually a result of cardiovascular collapse or upper/lower airway obstruction.17
Signs and Symptoms of Anaphylaxis
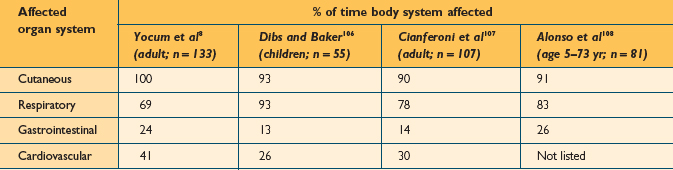
The clinical manifestations of anaphylaxis occur as a result of the systemic release of mediators from basophils and mast cells, and therefore involve some predictable signs and symptoms in organs with high concentrations of these cells.22 The upper and lower airways, skin, conjunctiva, gastrointestinal and cardiovascular systems are often affected individually or in combination. The most common signs and symptoms have been described in several publications. Kemp et al published the largest series detailing the clinical manifestations of anaphylactic reactions in 266 patients. The findings of this study are listed in Table 15.3. Several other publications have reported on the organ systems commonly affected during anaphylactic reactions in smaller series of patients (Table 15.4). The onset of symptoms of anaphylaxis is usually fairly rapid. When an antigen is introduced by injection, symptoms typically begin within 5–20 minutes,23 but more delayed initial reactions can certainly occur. It is rare for anaphylaxis to occur beyond 60 minutes after antigen injection.23,24 Ingestion of offending foods and drugs tends to result in a slower onset of anaphylaxis. It may take several hours after ingestion for anaphylaxis symptoms to begin, but in some cases, there can be rapid onset within minutes. The median time for anaphylaxis to occur after an insect sting is 15 minutes.10,25,26 It is generally considered that the more rapid the onset, the more severe the overall reaction.10,27,28
TABLE 15.3 Common signs and symptoms of anaphylaxis
| % of patients affected (Kemp et al105; n = 266) | |
|---|---|
| Urticaria, angioedema | 90 |
| Shortness of breath, wheezing | 60 |
| Dizziness, syncope | 29 |
| Flushed skin | 28 |
| Abdominal cramps, diarrhea | 26 |
| Laryngeal or tongue edema, choking dysphagia | 24 |
| Nausea, emesis | 20 |
| Hypotension | 20 |
| Rhinitis symptoms | 16 |
| Conjunctivitis symptoms, periorbital edema | 12 |
| Substernal or esophageal discomfort | 6 |
| Headache | 5 |
| Generalized pruritis (no rash) | 4 |
| Vision change | 2 |
| Seizure | 2 |
Cutaneous involvement is by far the most common finding with anaphylaxis. Urticaria and edema are the most common cutaneous manifestations. Although these skin reactions are almost always present, the lack of skin involvement cannot completely rule out anaphylaxis. Some authors have reported series of patients who presented with severe anaphylaxis without known cutaneous symptoms.29,30
The respiratory tract is also commonly involved in an anaphylactic reaction. Exacerbation of nasal allergy symptoms often occurs early in the process. A person might experience a feeling of tightness in the throat. The voice may become hoarse as edema develops in the larynx. Lower airway involvement leads to cough, wheezing, and dyspnea as anaphylaxis progresses.31
Tachycardia is usually a reliable early sign of cardiovascular involvement due to a decrease in effective vascular volume. Skin flushing and erythema from vasodilation may occur. As circulatory collapse ensues, the skin may become cool and clammy. Hypotension can result in multiple generalized symptoms, including dizziness, confusion, nausea, emesis, and abdominal cramps. Coronary vasospasm can result in chest pain, arrhythmias, and myocardial infarction.32,33 In severe anaphylaxis, cardiovascular shock is the endpoint, with multiple organ failure.20
Anaphylaxis may occur in biphasic or protracted patterns. After recovering from an initial episode of anaphylaxis, recurrent symptoms may develop. This process is known as biphasic anaphylaxis. This is thought to be a consequence of the classic late-phase allergic reaction. The recurrent symptoms begin from 1 to 28 hours after resolution of the initial episode. The secondary reaction usually involves the same organ symptoms as the original reaction.34 The true incidence of biphasic anaphylaxis is not known. The reported frequency varies from 4 to 23% of anaphylaxis cases. The highest reported frequency (23%) occurred with food reactions. It has been reported that a biphasic reaction is more likely to occur if the initial reaction is severe. A biphasic reaction occurs in up to 30% of severe food-induced anaphylaxis cases.35 Allergen injections have a much lower reported frequency, occurring in about 4% of anaphylaxis cases.32 Due to the possibility of biphasic reactions, the clinician should consider a 12- to 24-hour hospital observation of a patient after the successful treatment of an initial episode of anaphylaxis.36,37 Protracted anaphylaxis can also occur, with prolonged symptoms lasting 5–32 hours. Protracted anaphylaxis usually involves prolonged respiratory distress or hypotension.32
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


