Chapter 8 Management of the Child with Otitis Media
Otitis media (OM) is a significant problem for infants and children. Acute otitis media (AOM) is the second most common infectious diagnosis in the first year of life, and the number one reason for the use of antibiotics in this age group. Acute otitis media and recurrent acute otitis media (RAOM) are both considerable clinical problems in infants and children. From an economic standpoint an estimated US$5 billion a year is expended combating this problem in the USA.1 Recent studies have also suggested that the overall incidence of AOM is increasing. Joki-Erkkila et al evaluated the diagnosis of AOM from 1978 through 1979 and compared it to 1994 through 1995. They demonstrated an increased incidence of 68% with a 95% confidence interval.2
As a general rule most episodes of AOM are treated with at least one course of oral antibiotics by primary care practitioners. Besides the significant potential side effects of oral antibiotics, each episode of AOM is associated with a conductive hearing loss due to residual middle ear fluid present in 50% of treated ears after 1 month of infection. As described above, a subset of children with acute otitis media develop multiple episodes of AOM known as recurrent acute otitis media (RAOM). These children with RAOM are also designated as otitis prone. Therapeutic options for children with RAOM are limited to either long-term administration of prophylactic antibiotics or placement of tympanostomy tubes. Tympanostomy tube placement is the most common suggested surgical intervention performed in children.3–5 Although this is a relatively simple procedure, it still requires a general anesthetic and reported complications include prolonged otorrhea and persistent tympanic membrane perforations.6–16
Although recurrent acute otitis media is a very common diagnosis, the pathophysiological mechanism under this disorder is multifactorial and poorly understood. There are numerous risk factors for the development of RAOM. These include male gender, sibling history of recurrent otitis media, early occurrence of infection, absence of breast-feeding, day care attendance, and second-hand smoke.17 A recent meta-analysis conducted by Uhari and colleagues analyzed risk factors associated with AOM. They found sibling history, day care attendance, parental smoking, breast-feeding less than 3 months, and pacifier use as significant risk factors for RAOM.18
Epidemiology
As described above, there are several risk factors involved in the development of acute otitis media, not the least of which is crowding in large day care centers. Indeed day care attendance is a complex risk factor for many infectious illnesses in infants and young children. Alho and colleagues looked at risk factors for RAOM and upper respiratory tract infections (URTI). They found both day care attendance and short duration of breast-feeding to be significant risk factors, increasing the risk of both RAOM and URTIs.19 Fleming and colleagues looked at two groups of children, those attending day care on a regular basis and those who did not attend day care. They also found children in day care had an increased risk of URTIs and an increased risk of ear infections. These investigators found that 66% of ear infections were linked to day care attendance.20 Collet and colleagues did an 8.5-month prospective study of children in day care. Their study demonstrated an increased risk factor of greater than or equal to five episodes of URTIs, two episodes of AOM, and two episodes of conjunctivitis.21 Other investigators have attempted to understand the basis for this increased risk. Stenstrom and Ingvarsson performed a retrospective review that looked at general illness in otitis prone (OP) versus nonotitis prone (NOP) children. They found otitis prone children accounted for between two and four times the number of episodes of rhinopharyngitis, sinusitis and tonsillitis, and significantly more episodes of bronchopulmonary infections, gastrointestinal and urinary tract infections.22 Kvaerner and colleagues evaluated exposure to upper respiratory pathogens in AOM. They found that sibling attendance in day care was the most prominent risk factor for the development of AOM, followed by the number of children in the day care center.23
It has been suggested that day care attendance may create differences in nasopharyngeal colonization. These differences in chronic nasopharyngeal colonization may play a significant role in the development of the subset of children designated as otitis prone. Indeed the incidence of bilateral myringotomy and tympanostomy intubation in children in day care is 31% versus 11% for the population not in day care.24 Brook and Gober evaluated the type of organisms found in the nasopharynx of otitis prone children versus nonotitis prone children. They found nonotitis prone children tended to have more diverse flora possibly thought to inhibit the attachment of middle ear pathogens in the nasopharynx.25 Ito and colleagues evaluated nasopharyngeal colonization of healthy children who attended day care and compared this to healthy children who did not attend day care. They demonstrated day care children were much more likely to have penicillin-resistant Streptococcus pneumoniae cultured from the nasopharynx compared to the controls not in day care.26 Other studies have shown that nasopharyngeal colonization with resistant organisms leads to an increased rate of AOM and unresolved otitis media.27 Farjo and colleagues evaluated different strains of Haemophilus influenzae in the nasopharynx of children at 16 day care centers. They demonstrated sharing of the same strains in 13 out of 15 day care centers. These authors suggested that this degree of sharing demonstrated transmission of the pathogenic organisms in the day care center.28
Relevant Anatomy and Physiology
▪ Eustachian Tube
The Eustachian tube is an important conduit between the nasopharynx and the middle ear. Composed of both bony and cartilaginous segments, it functions to equilibrate middle ear pressure, drain fluid in the middle ear, and protect the middle ear from infected nasopharyngeal secretions. Under most conditions, the Eustachian tube is closed, opening intermittently with swallowing to provide the tubal functions noted above. Numerous investigators have demonstrated that there are subsets of both children and adults who have Eustachian tube dysfunction.29–31 One major cause of Eustachian tube dysfunction involves lack of appropriate opening of the lumen, such as in patients suffering from cleft lip and cleft palate malformations. These individuals may easily develop middle ear atelectasis, and run significant risk for aspiration of nasopharyngeal pathogens. Mechanical obstruction due to inflammation or compression by a nasopharyngeal tumor or mass will also predispose patients to significant problems with middle ear atelectasis, leading to aspiration of middle ear pathogens from the nasopharynx. Alternatively, other patients have patulous Eustachian tubes that are abnormally open and provide poor protection of the middle ear from nasopharyngeal infecting agents. Age-related anatomic and functional differences have also been noted in the Eustachian tube.32 In adults the Eustachian tube is approximately 35 mm and inclined at a 45 degree angle. In infants the tube is around 18 mm, about half the size of adults, and positioned closer to a 0 degree angle. The shorter length and position of the Eustachian tube in infants and children is thought to lead to an increased likelihood of nasopharyngeal reflux and a decrease in clearance function.
▪ Middle Ear
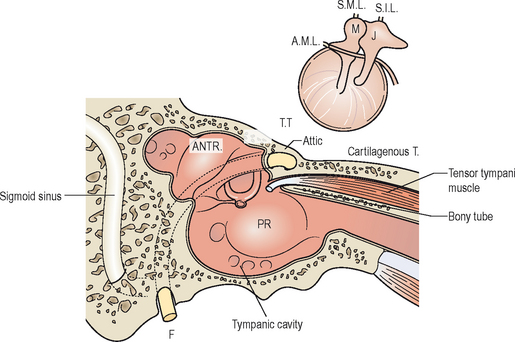
The middle ear is divided into three parts, the hypotympanum, mesotympanum, and epitympanum. The hypotympanum is defined as the area of the middle ear inferior to the tympanic membrane, while the mesotympanum covers the region of the middle ear medial to the tympanic membrane, and the epitympanum the superior aspect of the tympanic membrane. The direct open pathway of the middle ear at the level of the epitympanum to the aditus ad antrum and the mastoid air cells provides a potential route for spread of infectious processes from the middle ear to the mastoid cavity that could lead to development of acute mastoiditis, as shown in Figure 8.1.
Histology
The normal middle ear contains primarily cylindrical or layered cubic epithelium interspersed with ciliated cells. Adjacent to the Eustachian tube orifice the tympanic cavity epithelium changes to pseudo-stratified ciliated cells, as it is in the entire length of the Eustachian tube. There are different histological changes that occur during development of acute otitis media in normal ears, ears with some inflammatory change, and ears with a previous history of otitis media with effusion. For AOM in a normal ear, the goblet cell density is relatively low in the middle ear, immunologic defenses are not present, and recovery to a normal epithelium is usually fairly rapid. Development of AOM in a pathologic ear presents differently, as the epithelium is pseudo-stratified and cylindrical goblet cell glands are increased in density, resulting in a prolonged return to a normal histology. Conversely, the middle ear mucosa in an AOM-infected ear with a previous history of OME is pathologic and secretory, and filled with both mucus and secretions, with any additional episodes of AOM further deteriorating the histologic condition of the middle ear. For OME, initial histologic changes are similar to AOM, with an increase in goblet cells, basal cell hyperplasia, vessel dilation, and new gland formation. This may then go on to a secretory stage which is dominated by mucous secretions, an increase in goblet and mucous glands within the middle ear, and infiltration of lymphocyte fibroblasts and plasma cells. During the restoration phase of OME there is a period of decreased mucous production, degeneration of the mucous glands, and a pseudo-stratified epithelium that goes back to a one- or two-layered cubic epithelium, followed by a return of the middle ear to a more normal histologic condition.33
Pathophysiology
▪ Bacterial Infections
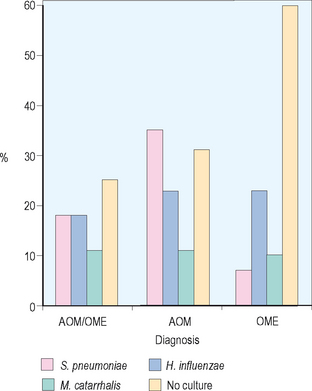
Acute otitis media has been revealed to be primarily a bacterial infection, with recent investigations even suggesting that COME is an indolent bacterial infection. Numerous investigators have demonstrated the importance of middle ear pathogens in the development of AOM. Bluestone and colleagues reviewed approximately 7400 middle ear isolates from children undergoing tympanostomy tube placement. They found Streptococcus pneumoniae and Haemophilus influenzae at 18%, Moraxella catarrhalis at 11%, mixed growth at 11%, and no growth at 25% overall in these 7400 isolates, as shown in Figure 8.2. When divided by diagnosis for children with AOM, 35% grew out S. pneumoniae, 23% H. influenzae, and 11% M. catarrhalis. For children with OME the predominant middle ear pathogen was H. influenzae at 23%, followed by M. catarrhalis 10%, and S. pneumoniae 7%. These investigators also demonstrated shifts in antibiotic resistance with beta-lactamase production from M. catarrhalis increasing from 60% to 80% in AOM and 60% to 100% in OME. Regarding H. influenzae they showed an increase of 15% to 25% for acute otitis media and 20% to 30% for OME.34
Other investigators have looked at the incidence of pneumococcal isolates to penicillin resistance and found that 61% of nasopharyngeal pneumococcal isolates from day care centers were penicillin resistant, versus a 33% rate of incidence of nasopharyngeal pneumococcal isolates that were penicillin resistant from a county health care center.35 There also may be significant clinical implications for shifts in antibiotic sensitivity. Antonelli and colleagues looked at the incidence of admission for mastoiditis at a major tertiary medical center between 1987 and 1997. Their study demonstrated a significant increase in the incidence of mastoiditis. S. pneumoniae was found to be the causative agent in the majority of these infections, with all but one strain of S. pneumoniae found to be penicillin resistant.36
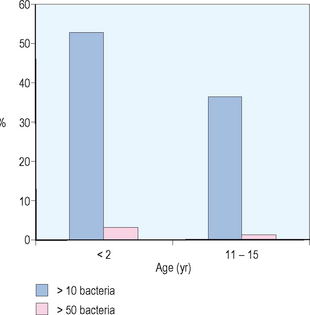
Although the normal middle ear is sterile, it has been suggested that ascending infection from the nasopharynx associated with Eustachian tube dysfunction is a critical step in the development of AOM. There is also an important relationship between nasopharyngeal colonization and otitis media. Stenfors and Raisanen evaluated attachment of bacterial cells in the nasopharynx in healthy children of different ages. They used immunofluorescence and graded the number of bacteria attached per nonciliated cell in the nasopharynx. As demonstrated in Figure 8.3, these investigators found for children less than 2 years old, 53% of nonciliated cells had greater than 10 attached bacteria and 36% of nonciliated cells had greater than 50 attached bacteria. For children 11–15 years old, 3% of nonciliated cells had greater than 10 attached bacteria while less than 1% of nonciliated cells had greater than 50 attached bacteria. These investigators also evaluated culture forming units of different middle ear pathogens. They found for children less than age 2, 100% had middle ear pathogens in the nasopharynx and for children 11–15 years of age only 44% had middle ear pathogens.37
▪ Viral Infections
The relationship between viral upper respiratory tract infections and acute otitis media is complex and not well understood. Ruskannen and colleagues recovered nasopharyngeal samples from 5092 children over a 5-year period and performed viral assays looking at the incidence of AOM. They found an increased incidence of AOM correlating in peaks from viral isolation of respiratory syncytial virus (RSV) from 1991 to 1992 and from 1993 to 1994. They also found an increased incidence of AOM in the fall of 1994 and early 1994 associated with adenovirus, parainfluenza virus, and influenza A virus. They found that 34% of patients with viral infections had AOM. The most common virus seen was RSV, followed by influenza A, parainfluenza type 3, adenovirus, and influenza B.38
Park et al performed a study using chinchillas to try to understand the potential role of viral infections in the pathogenesis of AOM.39 These investigators evaluated ciliary activity and dye transport function in chinchillas inoculated either intranasally or transbullarly with influenza type A virus. They used light microscopy and electron microscopy and demonstrated a disorganized epithelium and the presence of cellular debris in the Eustachian tube lumen 24 hours after injection. They also noted the presence of abnormal cilia and focal ciliated cell death seen up to 7 days post injection histopathologically. In addition, these investigators demonstrated extensive inflammatory and cellular infiltrate in the epithelial space at day 14. By 28 days the histology appeared normal. The same histopathologic features were identified whether the route of injection was transnasal or intrabullar. Evaluating ciliary beat frequency and dye transport, they showed a maximum decrease between 7 and 14 days with the return of normal activity by 28 days, as displayed in Figure 8.4. There was a close correlation between histopathological changes identified on light and electron microscopy and the functional analysis of ciliary motility as seen by ciliary beat frequency and dye transport. This study demonstrates the disruptive effect that viral infections can have on Eustachian tube function, and how this may lead to intrinsic obstruction of the Eustachian tube associated with inflammatory change.

▪ Altered or Impaired Immunity
A second host factor that is important in the development of RAOM is altered or impaired immunity. It has been demonstrated that certain bacteria may liberate exotoxins, toxic cell wall components, and endotoxins (i.e., purulent sinusitis transmembrane protein P15E can cause immunosuppression). This, along with an impaired immune response, may be a major factor in a predilection for RAOM. Bernstein looked at overall antibody titers of the IgG and IgG subclasses, and demonstrated that otitis prone children have significant reduction in antibody titers as compared to nonotitis prone children for numerous bacterial pathogens.40
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


