 Management of Retinoblastoma
Management of RetinoblastomaManagement of Retinoblastoma
General Considerations
The management of retinoblastoma has gone through a remarkable evolution in the last century, and the treatment has become complex (1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55, 56, 57, 58, 59, 60, 61, 62, 63, 64, 65, 66). Today, the selected treatment of this important childhood tumor depends on many factors and requires considerable knowledge and experience. Affected children are examined under general anesthesia, at which time various treatments are applied, depending on the clinical findings. The relative indications, methods, and results of the various treatment methods are detailed in other sources and they are briefly summarized and illustrated here.
The proper management of retinoblastoma requires periodic examination under anesthesia with ophthalmoscopy using scleral depression, and large fundus drawings to document size and location of all tumors, extent of retinal detachment, and tumor seeding. This is supplemental by further documentation with fundus photography, ultrasonography, and fluorescein angiography. Based on the findings the best method(s) of treatment are selected. When all tumors are controlled, examinations are done less frequently.
Enucleation
For many years, enucleation was the only legitimate treatment, and it remains the primary management in most unilateral cases and often for the worst eye in many bilateral cases (14, 15, 16, 17). There has been a decrease in the frequency of enucleation in recent years, although it is still used primarily for advanced group E retinoblastoma in eyes with no hope for useful vision (14). It is important for the surgeon to cut the optic nerve as far posteriorly in the orbit as possible because the main route of tumor spread is via the optic nerve to the brain. Considerable experience has been obtained using integrated implants and prostheses that improve cosmetic appearance and ocular motility after enucleation (1,14, 15, 16, 17).
External Beam Radiotherapy
In the mid-1900s, external beam radiotherapy became the main alternative to enucleation for salvaging eyes. It achieved good local control in most cases, and it is still used frequently in selected cases (40, 41, 42). However, EBRT is associated with an increased incidence of second cancers, mainly in the field of irradiation (63, 67, 68, 69, 70) and with facial cosmetic problems. Therefore, in recent years, there has been a trend toward avoiding both enucleation and EBRT when possible.
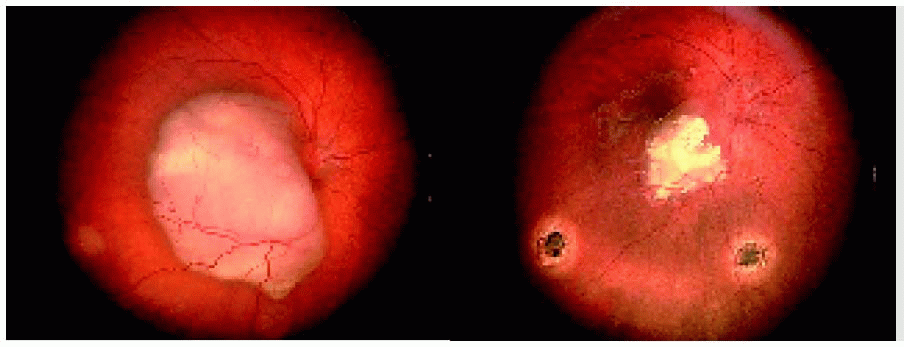
There are five tumor regression patterns following treatment for retinoblastoma. These patterns were originally applied to external beam radiotherapy. However, they are also now applied to other, more recent methods, including plaque radiotherapy, chemoreduction, laser photocoagulation, and cryotherapy, and they can even be applied to spontaneously regressed or spontaneously arrested tumors. These regression patterns are classified into type 0, tumor regression with complete tumor disappearance leaving no observable scar; type 1, tumor regression with complete calcification; type 2, tumor regression with no calcification (“fish-flesh” appearance); type 3, tumor regression with partial calcification; and type 4, tumor regression with flat atrophic scar. Selected examples are illustrated in subsequent sections.
Plaque Radiotherapy
Because of the potential complications of EBRT, plaque brachytherapy gradually become more popular, mainly for medium-size, localized retinoblastoma (43, 44, 45, 46, 47, 48, 49, 50, 51). It was initially used as a primary treatment, and later was used most often for tumors that failed EBRT, cryotherapy, or laser photocoagulation (43,47,51). Plaque radiotherapy continues to be a valuable adjunct as primary or secondary treatment for selected cases of retinoblastoma. A custom-designed radioactive plaque, usually with iodine-125 seeds, is sutured to the sclera directly over the base of the tumor. This requires considerable experience and meticulous alignment using binocular indirect ophthalmoscopy and scleral indentation to achieve precise localization for plaque placement.
Cryotherapy
Several alternative or supplemental methods of management have been popularized in recent years. Cryotherapy became popular for localized, more-peripheral lesions near the ora serrata. It is generally applied by a triple freeze-thaw technique with three applications at the same time to each tumor, using a standard cryoprobe used in retinal detachment treatment (52,53). Cryotherapy is an important supplemental method that is used routinely on many cases today.
Laser Photocoagulation
Xenon photocoagulation and argon laser photocoagulation became very popular for the management of small, posteriorly located tumors, and the results were encouraging. The technique is to apply moderately heavy laser treatment around the tumor to destroy its blood supply and induce its regression (54, 55, 56). In recent years, xenon photocoagulation and argon laser have been replaced in many centers by transpupillary thermotherapy.
Transpupillary Thermotherapy
A recently popularized technique of treatment is transpupillary thermotherapy (TTT). It delivers thermal heat to the tumor and results in a smaller residual scar than laser or cryotherapy treatment. We use it extensively in managing retinoblastoma. TTT can be used as a primary treatment for small retinoblastomas, but it is used more often as consolidation after tumor treatment with chemoreduction, plaque radiotherapy, or other methods (39).
Chemotherapy
Chemotherapy is generally reserved for patients who have evidence of tumor extension into the choroid, anterior chamber, optic nerve, or orbit. It is often used in conjunction with EBRT and other methods of treatment (1, 2, 3, 4, 5, 6,12,21).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


