Management of Orbital Trauma
Mami Aiello Iwamoto
Nicholas T. Iliff
Trauma to the orbits may be blunt or penetrating in nature and can result in injury to the bone or soft tissue. The size, composition, and velocity of the object inflicting trauma, the direction, and point of impact affect the severity and type of injury. This chapter discusses a method for evaluating a patient with orbital trauma and the specific diagnosis and management of traumatic optic neuropathy, orbital hematoma, bony orbital injury, and orbital foreign bodies.
INITIAL ASSESSMENT
Intraocular injuries occur in up to 67% of patients with maxillofacial trauma.1 In the United States, perforating globe injury occurs in 35% of patients with ocular trauma that requires hospitalization.2 Therefore, in evaluating orbital trauma, one should have a high index of suspicion for concomitant vision-threatening ocular complications, such as globe rupture, or indirect structural damage to the anterior segment, posterior segment, or optic nerve. The history and examination should be directed to identifying the extent of injury. Inquiry into the circumstances of the trauma will elucidate the mechanism of injury and help to direct the examination and diagnostic procedures toward the establishment of a diagnosis and formulation of a management plan. Depending upon the size of an object relative to the bony orbit, the force from the impact may be dissipated more over the orbital soft tissue or along the bone. Smaller objects traveling at relatively high velocity may result in penetrating injury and potentially a retained orbital foreign body. Denser, less forgiving objects will not absorb an impact’s kinetic force, which will then be transmitted more directly to the orbital structures. Trajectory of the object and point of impact will predict the structure that will most likely incur the brunt of the impact. Although generally well protected by the bony orbit, the globe may be injured, and coexisting intraocular injuries must be identified and managed accordingly.
Knowledge of orbital and periorbital anatomy is the basis for appreciating the significance of symptoms and clinical findings. If there is a report of decreased vision, ocular injury must be ruled out. If there is no evidence of intraocular injury, trauma to the optic nerve must be considered. Diplopia following orbital fracture may result from direct injury to, or incarceration of, an extraocular muscle, nerve injury to the extraocular muscle, or from the mass effect of orbital hemorrhage causing globe dystopia. Acute proptosis may be indicative of mass effect, such as with a hemorrhage, edema, or emphysema, or due to bone displacement into the orbit associated with fractures. Infraorbital hypesthesia suggests infraorbital nerve trauma as with some orbital floor fractures. Acute epiphora may indicate injury to the lacrimal system with medial canthal or nasoethmoidal trauma. Rhinorrhea should raise suspicion for cerebrospinal fluid leak in roof fractures.
The eye should be examined with minimal manipulation until the integrity of the globe is established. Visual acuity, pupillary examination, and color vision testing using Hardy-Rand-Rittler (HRR) or Ishihara pseudoisochromatic plates help to determine the optic nerve function. The adnexal and periocular structures should be examined carefully for potentially subtle foreign body penetration sites that may leave only minor external wounds. The orbital rims should be palpated to detect bone contour deformities, such as a step-off. Hyphema needs to be identified because this represents a relative contraindication for orbital surgery due to the potentially increased risk of complications from rebleeding. A delay of at least 1 week after the clearing of the anterior chamber should be considered. A dilated fundus examination can determine presence of lenticular trauma, retinal detachment, or intraocular foreign bodies. Such findings as sector retinal contusion or retinitis sclopeteria may indicate an occult intraorbital foreign body.
Computed tomographic (CT) scan of the orbits is the radiologic study of choice for further evaluating orbital trauma and detecting foreign bodies. High quality axial and coronal views are recommended. The newer spiral multi-detector CT scans provide more rapid image acquisition, improved image resolution, and flexibility to reformat coronal or sagittal views without having to reposition the patient. Three-dimensional reconstructions of digitized CT scan images may facilitate the assessment of complex orbital fractures but are limitedin evaluating isolated orbital floor fractures, since image artifact from reconstructing relatively thin bone of the orbital floor may obscure the detail of the actual bony defect. CT scans, in general, are more helpful than magnetic resonance imaging (MRI) for visualizing bone. In addition, MRI is contraindicated if a ferromagnetic metallic foreign body is suspected.
TRAUMATIC OPTIC NEUROPATHY
Traumatic optic neuropathy is estimated to occur in 4% of midfacial, supraorbital, or frontal sinus fractures1 and, therefore, should be suspected when there is decreased vision following orbital trauma in absence of globe injury. There will be a relative afferent papillary defect and evidence of orbital soft tissue injury. Visual acuity, afferent pupillary defects, visual fields, and color vision should be ascertained when possible. When damage occurs in the intraorbital portion of the optic nerve, the appearance of the fundus may resemble a central retinal artery or vein occlusion and vitreous, subhyaloid, or retinal hemorrhages may be found radiating from the optic disc.3,4 However, with more posterior damage, the optic disc acutely may appear normal. An orbital CT scan should be obtained with axial and coronal views to assess the integrity of the optic nerve and the presence of an optic nerve sheath hematoma, orbital hemorrhage, or fracture (Fig. 1). The radiologic finding of optic canal fractures may be subtle, and blood in the posterior ethmoid sinus may be the only indication of a fracture with intracanalicular extension.
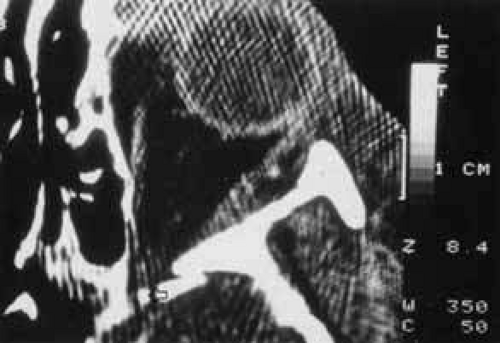 Fig. 1 CT scan of a fragment of bone extending into the optic canal (arrow). |
The optic nerve is susceptible to damage from three different mechanisms. Direct damage to the nerve from penetrating wounds causing avulsion, laceration, or impingement, such as by a fracture fragment, may present with immediate visual loss and carries a relatively poor prognosis for visual recovery.5,6,7,8,9 Perfusion of the optic nerve may be compromised in a type of “compartment syndrome,” where the confined intracanalicular portion of the optic nerve develops edema or hemorrhage.10 Onset of vision loss relative to the trauma may be slightly delayed, reflecting a progressive compressive etiology. The latter mechanism is most commonly found with injuries involving a blow to the frontal region.5,11 Holographic studies have suggested that force applied to the facial eminences can be transmitted to the optic foramen, with subsequent traction and shearing forces applied to the optic nerve and small nutrient vessels.6 A third mechanism of optic nerve injury is from rapid deceleration. The orbital portion of the optic nerve can sustain forward movement, but the intracanalicular portion is relatively fixed at the optic canal foramen, and the traction may result in hemorrhage from feeder vessel shearing, edema, or contusion necrosis.8 If traumatic optic neuropathy is suspected in the setting of coexisting orbital wall fracture, treatment of the latter should be delayed until after the optic nerve injury has been addressed.
MANAGEMENT OF TRAUMATIC OPTIC NEUROPATHIES
Management of traumatic optic neuropathy remains controversial. Intervention is advocated in suspected optic nerve trauma, unless there is clear evidence of an irreversible condition, such as optic nerve avulsion. Although spontaneous visual recovery has been reported,3,12,13 treatment with high-dose corticosteroids or surgical decompression represent viable options. Intravenous corticosteroids may be beneficial in treating traumatic optic neuropathy.10,14,15,16 The recommendations are based upon spinal cord injury treatment studies. The rationale for high-dose steroid use is based on the hypothesis that significant central nervous system trauma initiates free radial damage, which is inhibited by the corticosteroids.17,18 In spinal cord injuries, steroids should be administered within 8 hours of injury to be efficacious.19 A loading dose of methylprednisolone 30 mg/kg intravenously, followed by 15 mg/kg administered 2 hours later, and then 15 mg/kg every 6 hours is recommended.7 If visual function improves within 24 hours, the steroid doses are continued for an additional 5 days, then tapered rapidly. When no improvement occurs within 48 to 72 hours, steroid administration is discontinued without a tapering dose.14 Some authors advocate decompression of the optic canal if a trial of high-dose steroids does not produce a favorable response.14,20,21 Surgery has been advocated based on the rationale that decompression may reduce the compressive effect of hemorrhage, edema, or bone fragments. Transantral-ethmoidal,5,22 transethmoidal,23,24,25 transorbital,26 and modified frontal craniotomy27 approaches have been described. The relative benefits of steroid therapy and surgery for traumatic optic neuropathy are still quite controversial, and randomized, controlled clinical trials comparing no treatment, high-dose steroids, and specific surgical decompression are still needed to determine the best course of treatment.
ORBITAL HEMORRHAGE
Hemorrhage can be localized to the subperiosteal potential space, extraconally, or intraconally within the orbital soft tissue, or within the belly of extraocular muscles. The condition can be associated with pain, nausea, diplopia, or decreased vision. The more obvious finding might be lid ecchymosis and edema but requires further examination for retroseptal signs. There may be conjunctival chemosis or expanding ecchymosis. Clinical findings reflect the mass effect of accumulating blood within the confines of the bony orbit and orbital septum (Fig. 2). Subperiosteal hematomas are usually restricted by the tight adherence of the periosteum to the orbital bone except in areas, such as suture sites, where this association is weakest. Hemorrhage localized to the muscle sheath may cause selective extraocular muscle restriction that requires radiologic studies to distinguish it from incarceration into a fracture site (Fig. 3). Localized bleeds within the orbital soft tissue can produce proptosis or dystopia. Diffuse hemorrhage may limit eye movement globally and increase retropulsive resistance. Increased intraorbital pressure on the globe and optic nerve may cause elevated intraocular pressure, choroidal folds, compressive retinal vascular compromise, or optic neuropathy, so maintaining vigilance for progressive, potential, vision-threatening situations is important.
 Fig. 2 Proptosis, ecchymosis, and chemosis resulting from orbital hemorrhage. |
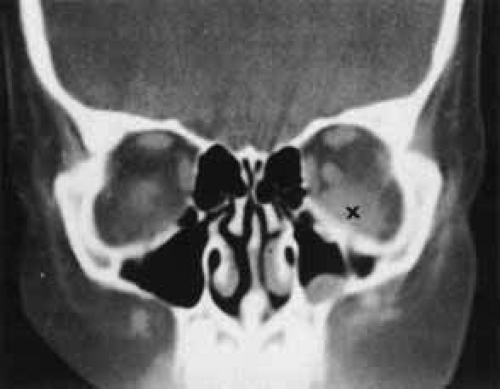 Fig. 3 CT scan of inferior orbital hematoma (X) involving the inferior rectus muscle and causing severe upgaze and moderate downgaze limitation. |
MANAGEMENT OF ORBITAL HEMORRHAGE
Orbital hemorrhages often resolve spontaneously without sequelae. However, if the hemorrhage is severe or progressive, it is important to identify the potential for vision-threatening central retinal artery occlusion by closely monitoring visual acuity, pupillary response, color vision, intraocular pressure, and retinal perfusion. The retinal perfusion may be inadequate if spontaneous pulsations of retinal arteries are present or are induced by applying minimal external globe pressure. Since perfusion compromise can result from either excessive elevation in intraorbital or intraocular pressures, both aspects are addressed. Intraocular pressure-lowering topical agents can be administered to lessen resistance to retinal arteriolar filling. If this is inadequate, the restriction and mechanical compression of the orbit from tight eyelids can be relieved by performing a lateral canthotomy, advancing to cantholysis if necessary. Intraocular pressure can be further diminished with an anterior chamber paracentesis, if vascular compromise remains imminent in spite of the other interventions.
Lateral canthotomy and cantholysis can be performed in a treatment room. Local anesthesia of 2% xylocaine with 1:100,000 epinephrine is injected in the lateral canthal area. The proposed incision extends horizontally from the lateral canthal angle, beyond the lateral fornix, to the level of the lateral orbital rim. This can be performed with a Stevens scissors alone, or, if cautery is not readily available, a straight clamp can be positioned in the proposed area and clamped for 10 seconds to provide hemostasis prior to making the incision with the scissors. Often this maneuver allows enough widening of the palpebral fissure to relieve orbital pressure. When this maneuver alone is ineffective, a lateral cantholysis is performed by positioning the Stevens scissors perpendicular to the canthotomy incision and releasing the lateral canthal ligament fibers in the lateral aspect of the upper and lower lids along their attachments to the rim (Fig. 4).28 Additional decompression of the orbit rarely becomes necessary and would best be managed under general anesthesia with the intent to explore the orbit for the mechanism of active bleeding with possible bony decompression of the lateral wall.
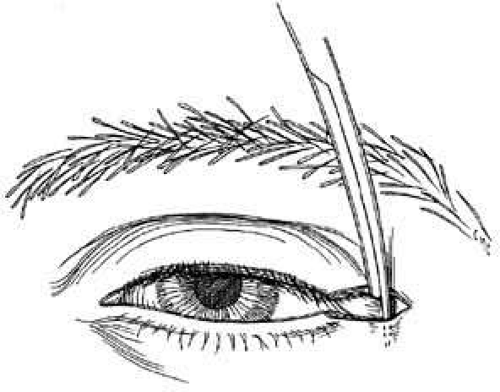 Fig. 4 Lateral cantholysis is accomplished by making a vertical incision through the lateral canthal ligament. |
ORBITAL BLOWOUT FRACTURES
Orbital floor, or blowout, fractures are common sequelae of blunt trauma and refer to fractures of the orbital floor that are not associated with fractures of the orbital rim. These fractures are induced by two possible mechanisms. The hydraulic theory suggests that blunt impact causes an increase in orbital pressure and the compression force is transmitted to the orbital walls, resulting in fracture of the weaker posterior floor region.29 The buckling theory suggests a direct impact onto the inferior orbital rim transmits force and results in a compressive fracture of the floor.30
This type of injury should be suspected when there is a blunt impact by an object usually larger than the span of the orbital rims. There is often pain at the impact site, enophthalmos, diplopia on upgaze, or infraorbital nerve dysesthesia. Often there is lid edema and ecchymosis, but a relatively atraumatic “white-eyed” appearance may be a more typical presentation in children.31 A CT scan with coronal views delineates the fracture size and degree of displacement as well as the associated soft tissue damage, such as prolapse of orbital fat or injury to the inferior rectus muscle.
MANAGEMENT OF BLOWOUT FRACTURES
Over the last 4 decades, the two issues central to management controversies have been the indications and the ideal timing for surgical intervention. Current guidelines are derived from reviews of numerous retrospective and noncomparative reports in the literature.32,33,34,35 A 1982 survey conducted among members of the American Society of Ophthalmic Plastic and Reconstructive Surgery reflects the absence of consensus in management approaches.36 Two-thirds of the 102 respondents were operating within 2 weeks of injury, one-third were operating 2 to 6 weeks after injury, and 2% were observing for 4 to 6 months. In brief, the advocates of early surgery37 (within 2 weeks after injury) claim that in the acute setting, less scarring is encountered and dissection and repositioning of the prolapsed tissue is easier. Indeed, others believe that with even earlier surgery (within days of injury), almost no scarring is noted. However, advocates of the conservative approach argue that waiting for spontaneous resolution of symptoms might obviate the need for surgery, which has potential morbidity.38 There is mounting evidence that early surgery gives better results than late. It has been demonstrated in a randomized prospective study that in patients with strabismus following blowout fracture, surgery within 72 hours produces a better extraocular motility outcome than if the surgery is performed after 10 days.39 A waiting period of up to 14 days may no longer be appropriate. The decision, based on CT scan and clinical findings as to whether or not to operate, can be made within day 1 or 2 of injury in nearly all cases.
Fractures resulting in trapdoor incarceration of soft tissue and those generating an oculocardiac reflex are conditions warranting urgent surgical intervention, ideally within hours of injury. Trapdoor entrapment fractures occur more often in children, as their more flexible bone will fracture then bend back and incarcerate soft tissue and risk ischemic damage (Fig. 5 and 6). Morbidity results if there is a muscular or perimuscular soft tissue entrapment and earlier repair appears to yield better outcomes.40 Urgent intervention is also indicated if there is persistent oculocardiac reflex40,41 or when soft tissue entrapment in the fracture induces vagal symptoms of nausea, vomiting, syncope and possibly heart block.
 Fig. 5 Right blowout fracture with prolapse of tissue into the fracture, causing limitation of upgaze. |
 Fig. 6 CT scan of trapdoor floor fracture. The inferior rectus is seen in the maxillary sinus (arrow). The fractured portion of the orbital floor has returned nearly to its original position.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|