CHAPTER 83 Malignancies of the Paranasal Sinus
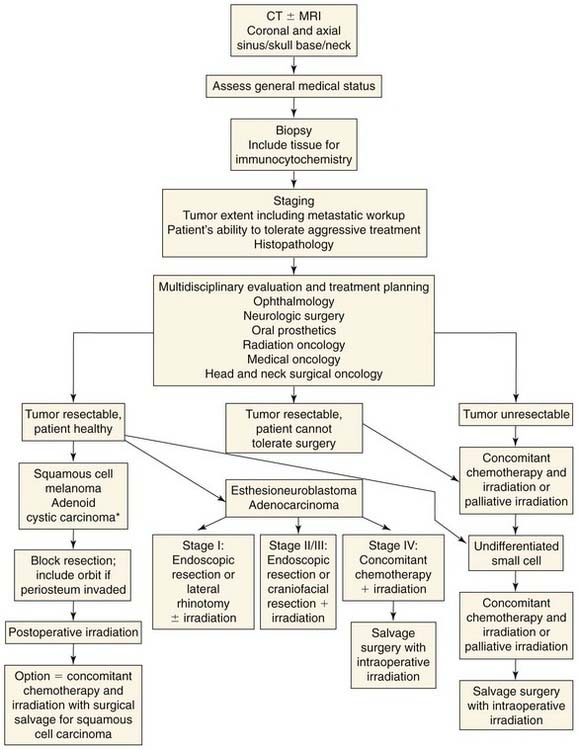
This chapter first reviews material common to all sinus tumors: anatomy, symptoms, physical findings, diagnostic assessment, and surgical options. Although these lesions are rare, numerous histologic subtypes must be discussed individually because management varies significantly among them (Fig. 83-1).
Epidemiology and Survival
Malignant lesions within the sinuses are uncommon, accounting for less than 1% of all neoplasms, with a frequency of 0.1 to 0.3 per 100,000 during the first decade of life that rises to 7 per 100,000 by the eighth decade of life.1 Several histologic subtypes have been described. In one of the most widely cited papers on the incidence of malignant sinonasal lesions, Jackson and colleagues2 reviewed 115 patients between 1957 and 1974 and reported on the histologic distribution of their tumors (Table 83-1). These rates are similar to those in a review by Sisson and associates3 in 1989. In 2007, the Memorial Sloan-Kettering Cancer Center published their experience with paranasal sinus malignancies; the histologic prevalence remains similar to that described by Jackson 30 years earlier (see Table 83-1).4 The most common lesions reported were squamous cell carcinomas, with a frequency of less than 1 per 200,000 per year.
Table 83-1 Rates of Malignant Tumors
| Number Reported (%) | ||
|---|---|---|
| Histology | Jackson et al (1977)2 | Hoppe et al (2007)4 |
| Squamous cell carcinoma | 61 (55) | 42 (49) |
| Undifferentiated carcinoma | 11 (10) | 4 (5) |
| Adenoid cystic carcinoma | 8 (7) | 11 (13) |
| Adenocarcinoma | 7 (6) | 6 (7) |
| Melanoma | 7 (6) | |
| Olfactory neuroblastoma | 5 (4) | 7 (8) |
| Fibrosarcoma | 3 (3) | 9 (11) |
| Papillary adenocarcinoma | 2 (2) | |
| Transitional cell carcinoma | 2 (2) | |
| Plasmacytoma | 2 (2) | |
| Hemangiopericytoma | 1 (1) | |
| Lymphoma | 1 (1) | |
| Carcinosarcoma | 1 (1) | |
| Chondrosarcoma | 1 (1) | |
| Neuroendocrine | n/a | 2 (3) |
A large retrospective review of 220 patients with nasal and paranasal sinus malignancies showed a 5-year survival rate of 40%.1 The National Cancer Institute created the Survival, Epidemiology, and End Result (SEER) database in 1973. This database enables accurate estimates for cancer incidence and mortality in the United States. In 2006, Davies and Welch5 used this database to compile recent incidence and mortality rates for head and neck cancer. The data suggest that mortality for sinus malignancies decreased by 11% between 1990 and 2001.
Numerous environmental agents are considered to have a causal relationship with carcinoma of the paranasal sinuses. The following are all associated with squamous cell carcinoma: aflatoxin, found in certain foods and dust; chromium, nickel, mustard gas, polycyclic hydrocarbons, and other organic chemicals, usually from manufacturing processes; and mesothorium (Thorotrast), a radiopaque dye used as a contrast medium within the antrum. Wood dust has a particular association with adenocarcinoma of the ethmoid sinus. Tobacco smoke, salted or smoked foods, woodworking, heavy metal exposure, and hydrocarbon refining have all been linked with a higher incidence of these malignancies. There is a 2 : 1 male to female preponderance, likely due to the higher rates of male workers in the occupations listed. Additionally, human papillomavirus, including subtypes 6, 11, and 18, has been identified in inverted papilloma and associated squamous cell carcinoma.6
Anatomy
Maxillary Antrum
As noted by Ohngren,7 the most prognostically significant structures are above and behind the maxillary antrum. Superior to this structure are the orbit and the ethmoid sinus. The posterior boundary includes the pterygoid plates, the pterygoid space, and the infratemporal fossa. The other boundary areas are more easily resected en bloc and thus are less worrisome when involved. Anteriorly lies the canine fossa, inferiorly the alveolus, and medially the nasal cavity.
Lymphatics
Ohngren7 emphasized the importance of precise understanding of the lymphatic drainage of the nose and paranasal sinuses as a prerequisite to adequate therapy. He contested the established dictum that these tumors do not often metastasize. He held that they do metastasize but that clinical evidence of early metastasis is absent because the primary drainage is to the lateral and retropharyngeal nodes. He believed that the relative success of his therapy hinged on electrocoagulation and irradiation of the rich lymphatic channels passing from the nose and paranasal sinuses posteriorly to the retropharynx which remains an important therapeutic concept.
Symptoms
In the review of 115 patients by Jackson and colleagues,2 the symptoms associated with malignancy were nasal obstruction (61%), localized pain (43%), epistaxis (40%), swelling (29%), nasal discharge (26%), epiphora (19%), palate lesion (10%), diplopia (8%), cheek numbness (8%), decreased vision (8%), neck mass (4%), proptosis (3%), and trismus (2%). As the disease becomes more advanced, the tumor infiltrates adjacent structures, giving rise to these symptoms as follows:
Physical Findings
Diagnostic Assessment
Imaging Studies
Computed Tomography
Computed tomography (CT) is the initial imaging modality of choice for paranasal sinus disease. CT is superior to magnetic resonance imaging (MRI) for detection of bony involvement. CT scanning is also particularly helpful for evaluation of tumor involvement of the retroorbital and orbital apex region, where there should be a “central low density region of fat surrounding the optic nerve with a radial arrangement of the extraocular muscles.”9 Loss of this plane implies advanced disease because the veins in this area extend directly to the cavernous sinus. CT is also valuable in assessing infiltration of the nasopharynx, where normal anatomy consists of a very thin layer of mucosa over the medial pterygoid plate. Thickening in this region implies tumor infiltration.9 When evaluation of intracranial extension is necessary, contrast-enhanced CT may improve the definition of tumor from adjacent brain.
Surgical Options
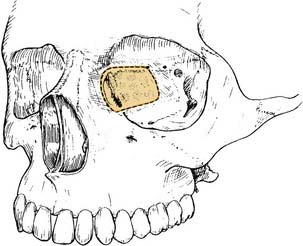
Extirpation of paranasal sinus tumors is a challenging exercise in surgical planning, which may be considered in three phases. First, one must assess the bony and soft tissue structures to be included for en bloc resection. Second, the approach must be designed to provide adequate exposure while preserving functional tissue and cosmetic integrity whenever possible. Third, the repair should be planned to use prosthetics or soft tissue techniques to the best advantage. See Figure 83-2 for anatomic reference.
Figure 83-2. Anatomic reference for the surgical options available for treatment of malignancies of the paranasal sinuses.
Classic “Open” Procedures
External Ethmoidectomy
INDICATIONS
The most limited operation to be discussed, external ethmoidectomy, is appropriate for removal of small tumors of the ethmoidal region and as an approach to biopsy and drainage of tumors of the sphenoethmoid region and the medial orbit (Fig. 83-3).
BENEFITS
The external ethmoidectomy approach allows excellent cosmesis and preservation of functional tissue.
Inferior Medial Maxillectomy
Medial Maxillectomy
Radical Maxillectomy
INDICATIONS
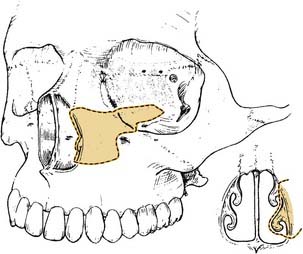
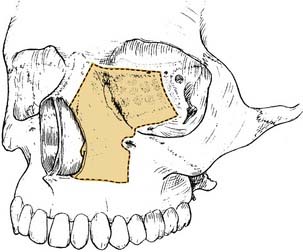
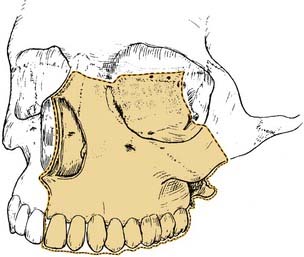
Radical maxillectomy is the standard operation for advanced carcinoma of the maxilla (Fig. 83-6). Considerable debate exists regarding the proper application of this procedure, because the amount of tissue to be removed depends on a careful assessment of the extent of tumor involvement. Another uncertainty relates to the establishment of proper indications for removal of the orbital contents in combination with radical maxillectomy.
SURGICAL APPROACH
The Weber-Ferguson incision is used with extensions around the eyelids to preserve those soft tissues. A skin or dermis graft is used to line the defect.10 A preformed obturator can be of great assistance in the immediate postoperative period because it acts as a support for packing and provides immediate dental function.
BENEFITS
Radical maxillectomy is adequate treatment for malignant tumors confined to the maxilla and those with extension to the facial soft tissues, lateral palate, or anterior orbit but without invasion of the eye, ethmoidal roof, posterior orbit, or pterygoid region. Historically, when the procedure was supplemented by irradiation, a cure rate approximating 30% was expected.2 However, in the update by Sisson and associates3 on their experience, patients who received multimodality therapy consisting of surgery, irradiation, and chemotherapy achieved a 5-year survival rate of 49%.3
There is little debate regarding the indications for resecting the orbital contents in patients with advanced paranasal sinus carcinoma.10a As indicated by Ketcham and Van Buren,8 the decision to excise the orbital contents was made on the basis of achieving an en bloc resection of the tumor. However, those researchers implied that as imaging became more precise, more selective resection might be possible. Perry and colleagues11 emphasized the impact of CT on surgical planning and documented that selective preservation of the orbital contents is appropriate and achieves adequate local control in properly selected cases.11 This finding was consistent with the experience of Weymuller and coworkers,12 who also could not demonstrate better local control or survival when the orbital contents were included in maxillectomy procedures. This position was later further supported by the experience of Larson and associates.13
LIMITATIONS
Even when orbital exenteration is included, a maxillectomy fails to provide an adequate resection when the tumor has escaped superiorly (ethmoidal roof) or posteriorly (orbital apex, pterygoid region). When these areas are demonstrably involved, one must decide whether to undertake craniofacial resection or use a regimen as described by Sakai and colleagues14 that relies on chemotherapy, curettage, and irradiation.
Craniofacial Frontoethmoidectomy
INDICATIONS
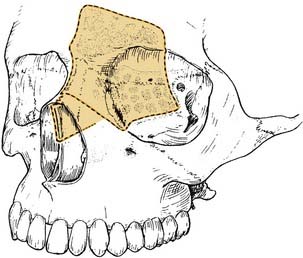
Craniofacial frontoethmoidectomy is specifically designed to provide en bloc resection for tumors of the ethmoidal and frontal regions (Fig. 83-7). By including exposure of the anterior cranial fossa, the procedure makes possible complete resection of the ethmoid and frontal sinuses, and dural resection may be included when necessary. As previously noted, one or more margins of these extensive resections are often limited by proximity to the eye or brain, resulting in surgical margins that are “microscopically positive” for tumor.
SURGICAL APPROACH
The craniofacial frontoethmoidectomy approach described by Kaplan and associates15 allows excellent exposure with preservation of the supraorbital rim to decrease the cosmetic impact of the procedure. Although removal of the eye is unpleasant to consider, Ketcham and Van Buren8 have documented an improved survival when orbital resection is combined with craniofacial resection (57%, vs. 26% without exenteration).
BENEFITS
An international collaboration reviewing 188 patients published a report in 2005. The reported mortality associated with craniofacial resection was 4.5%, and the complication rate was 33%.16 Surgical margins, histologic type, and intracranial extension were independent predictors of survival. Shah and associates17 reported their experience with 71 patients, which showed an overall 5-year survival of 56% and a median survival of 4.2 years. Like the international group, Shah and associates17 showed that intracranial involvement predicted significantly worse survival.



