CHAPTER 119 Lymphomas Presenting in the Head and Neck
Lymphomas are malignant neoplasms of lymphocytes and their precursor cells. Historically, lymphomas were classified merely by their histologic appearance, specifically cell size (e.g., small, large, mixed) and architecture (nodular or diffuse). The current classification system is the World Health Organization (WHO) system, which defines specific subcategories of lymphoma according to the immunologic and molecular characteristics of the lymphoma cells, as well as the morphology.1 Most subtypes of lymphoma can potentially involve the head and neck, either as the only site of disease or as one of many sites of involvement. Because an enlarged cervical or supraclavicular lymph node is a common presentation of many lymphomas, otolaryngologists are often the first physicians to evaluate and biopsy these patients, as well as the first to inform patients of their diagnosis. Understanding the pathology, clinical features, treatment, and prognosis for each of the nodal and extranodal lymphoma subtypes that can present in the head and neck will allow for a more accurate and efficient evaluation. In addition, a brief discussion of the diagnosis and prognosis by the head and neck specialist is extremely valuable to patients and their families while they are awaiting an initial appointment with a medical oncologist.
Epidemiology
It is estimated that 74,300 new cases of lymphoma will be diagnosed in the United States in 2008, including 66,100 cases of non-Hodgkin’s lymphoma (NHL) and 8200 cases of Hodgkin’s lymphoma (HL).2 The incidence of NHL rose dramatically between 1970 and 1995 but has stabilized over the past 14 years. The cause of this increase is incompletely understood. The human immunodeficiency virus (HIV) epidemic and the increase in NHL after solid-organ transplants account for only a minority of the new lymphomas. The incidence of NHL is slightly higher in men than women and increases exponentially with age. The most reproducible environmental risk factor includes exposure to certain pesticides or herbicides, and inconsistent associations have been reported with hair dyes, certain occupations, smoking, consuming foods high in animal fat, and receiving blood transfusions.3 Infectious agents including Epstein-Barr virus (EBV), HIV, human T-cell leukemia virus (HTLV)-1, Helicobacter pylori, Chlamydia psittaci, hepatitis C, HHV8, and Borrelia burgdorferi have been proposed as etiologic agents in the pathogenesis of some cases of NHL.4 Other factors associated with a significant increased risk of NHL include autoimmune disorders, most commonly Sjögren’s syndrome and rheumatoid arthritis, although it is difficult to separate the effects of immunosuppressive drugs used to treat these diseases and the underlying autoimmune disease.
HL has a bimodal age distribution in developed countries, with the first peak occurring in the third decade of life and the second peak occurring after age 50 years. Men have a slightly higher incidence than women. There is an association between HL and factors that decrease exposure to infectious agents at an early age including advanced maternal education, early birth order, decreased number of siblings, and living in a single-family residence. A history of infectious mononucleosis increases the risk of HL twofold to threefold and suggests EBV as an etiologic agent.5 There is a slightly increased risk of HL in patients infected with HIV and other conditions associated with chronic immunosuppression. An increased incidence among first-degree relatives, a significant concordance rate among identical but not fraternal twins, and linkage with certain HLA types suggest a genetic predisposition for HL.6 The incidence of HL varies significantly with geography, suggesting either an environmental or a genetic association. HL is rare in Japan, but interestingly, the incidence increases in Japanese Americans, suggesting an important environmental component.7
Clinical Presentation of Lymphomas of the Head and Neck
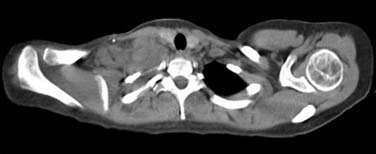
Classical HL occurs most commonly in young adults and usually presents as painless lymphadenopathy in the cervical and/or supraclavicular regions. In contrast to NHL, HL spreads in a contiguous pattern and rarely involves the preauricular or occipital nodes or extranodal sites of the head and neck such as the tonsil or sinus. Infraclavicular involvement in patients with bulky supraclavicular nodes is common in HL but is rarely seen in NHL. Bulky, matted nodes are not uncommon (Fig. 119-1). Although staging studies reveal mediastinal adenopathy in more than 85% of patients with HL, symptoms of cough, chest pain, dyspnea, and superior vena cava (SVC) syndrome are uncommon, even in patients with bulky mediastinal disease. Systemic symptoms or “B” symptoms including fevers (temperature > 38° C), drenching night sweats, and weight loss occur in 30% to 40% of patients with stage III or IV disease, but in less than 10% of patients with stage I or II disease. A hallmark of HL, generalized, severe pruritus, occurs in approximately 25% of patients with HL, often precedes the diagnosis by months, can be a presenting symptom of both early and advanced-stage disease, and has no known prognostic significance. Alcohol-induced pain in involved lymph nodes is a rare symptom of HL (<1%). A rare subtype of HL, nodular lymphocyte-predominant HL (LPHL), usually presents as a solitary cervical, axillary, or inguinal lymph node. In LPHL the mediastinum is generally spared, and in contrast to the contiguous pattern of lymph node involvement in classic HL, there is no consistent pattern of spread.
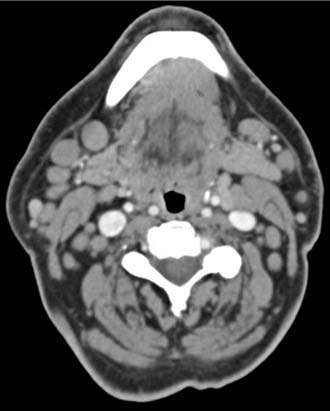
Presenting symptoms of NHLs vary substantially depending on the pathologic subtype of NHL and the site(s) of disease. Indolent lymphomas such as follicular (FL) or small lymphocytic (SLL) lymphomas often present with painless, peripheral adenopathy. Multiple soft, mobile, bilateral cervical nodes ranging in size from 1 to 2 cm are common presentations of both FL and SLL (Fig. 119-2). Matted peripheral lymph nodes are uncommon. Isolated head and neck involvement is unusual with these subtypes of lymphoma, and examination of axillary and inguinal regions usually reveals additional enlarged nodes. SLL can involve the tonsillar regions. Because spontaneous regressions occur in up to 20% of patients with FL, the patient may describe a history of waxing and waning adenopathy, with nodes present for years in some cases. Most patients with indolent lymphoma feel well at presentation, and B symptoms including fevers, drenching night sweats, and weight loss are unusual. Patients with SLL frequently have involvement of the peripheral blood, and a complete blood count may reveal a lymphocytosis. Peripheral blood flow cytometry may provide a diagnosis and obviate the need for a tissue biopsy. Indolent lymphomas are uncommon before age 50.
Biopsy Techniques and Specimen Handling
Tissue biopsy is essential in the diagnosis and management of patients with lymphomas. Recent advances in the immunology and molecular biology of lymphomas, as well as new diagnostic reagents and methods, have resulted in more precise diagnoses. The most recent WHO classification includes more than 25 subtypes of NHL, with B-cell neoplasms representing 80% to 90% of NHLs (Table 119-1). When the clinical history is suggestive of lymphoma, but initial histologic review and immunohistochemistry by flow cytometry or on paraffin-embedded tissue sections are nondiagnostic, molecular testing for T-cell receptor and immunoglobulin heavy-chain gene rearrangements should be considered. Cases in which the pathologic diagnosis seems inconsistent with the clinical history should be reviewed by an expert hematopathologist.
Table 119-1 Proposed World Health Organization Classification for NHL
| B-cell neoplasms |
| Precursor B-cell lymphoblastic leukemia/lymphoma* |
| Mature B-cell neoplasms |
| B-cell chronic lymphocytic leukemia/small lymphocytic lymphoma |
| B-cell prolymphocytic leukemia |
| Lymphoplasmacytic lymphoma |
| Mantle-cell lymphoma |
| Follicular lymphoma† |
| Marginal zone B-cell lymphoma of mucosa-associated lymphoid tissue (MALT) type |
| Nodal marginal zone lymphoma ± monocytoid B cells |
| Splenic marginal zone B-cell lymphoma |
| Hairy cell leukemia |
| Diffuse large B-cell lymphoma† |
| Subtypes: mediastinal (thymic), intravascular, primary effusion lymphoma |
| Burkitt’s lymphoma |
| Plasmacytoma |
| Plasma cell myeloma |
| T-cell neoplasms |
| Precursor T-cell lymphoblastic leukemia/lymphoma* |
| Mature T-cell and NK-cell neoplasms |
| T-cell prolymphocytic leukemia |
| T-cell large granular lymphocytic leukemia |
| NK-cell leukemia |
| Extranodal NK/T-cell lymphoma, nasal-type |
| Mycosis fungoides† |
| Sézary syndrome |
| Angioimmunoblastic T-cell lymphoma |
| Peripheral T-cell lymphoma (unspecified)† |
| Adult T-cell leukemia/lymphoma (HTLV1+)† |
| Systemic anaplastic large-cell lymphoma (T- and null-cell types)† |
| Primary cutaneous anaplastic large-cell lymphoma† |
| Subcutaneous panniculitis-like T-cell lymphoma |
| Enteropathy-type intestinal T-cell lymphoma |
| Hepatosplenic γ/δ T-cell lymphoma |
NHL, non-Hodgkin’s lymphoma; NK, natural killer.
* The classification of acute lymphoid leukemias will expand on the classification of precursor B-cell and T-cell malignancies, incorporating both immunophenotypic and genetic features.
† Morphologic and/or clinical variants of these diseases are not listed, for the purpose of clarity and ease of presentation.
Fine-Needle Aspiration
Due to the lack of fibrosis and a unique cytologic appearance and immunophenotype, small lymphocytic lymphoma and lymphoblastic lymphoma can often be accurately diagnosed solely on the basis of a fine-needle biopsy. Lymphoblastic lymphoma (LL), a high-grade lymphoma, often presents with SVC syndrome or severe dyspnea and progresses extremely rapidly. The ability of pathologists to provide a preliminary diagnosis within hours on the basis of an FNA of a supraclavicular or mediastinal node may allow earlier initiation of therapy. In one report of eight children with LL, FNA was employed as the initial diagnostic procedure.8 Immunophenotyping established the T cell derivation in all cases, and treatment was initiated only on the basis of FNA results in six cases. Two patients had subsequent surgical biopsies that confirmed the FNA diagnosis of LL. In a separate retrospective study, nine out of nine cases of lymphoblastic lymphoma were correctly identified on the basis of specimens obtained by FNA.9
Stewart and colleagues10 reported that FNA of palpable lymph nodes correctly identified 61 of 67 (91%) malignant lymphomas, with 27% of the cases representing recurrent lymphomas. However, in a more recent study, Hehn and colleagues11 found that a specific and complete histologic diagnosis of lymphoma was obtained in only 27 of 93 FNA attempts (29%) at initial diagnosis, and in only 9 of 22 FNA attempts (41%) done in the setting of recurrent disease. Importantly, these 115 needle aspirations were interpreted by 70 different pathologists in the community setting and only 43% had concurrent ancillary studies such as flow cytometry. Howlett and colleagues12 reported results of an audit of 276 patients who underwent FNA and subsequent surgery for evaluation of a “neck lump” at one of five hospitals in the Sussex cancer network in the United Kingdom during 2004. Of the 276 aspirations, 105 (38%) were nondiagnostic, 54 of 104 (52%) in the neck node group, 23 of 54 (43%) in the salivary gland group, and 28 of 118 (24%) in the thyroid group. Only patients in the thyroid group had ultrasound guidance for the procedure. Interestingly, 15 of the 54 nondiagnostic FNAs in the neck node group were NHL at surgery, as well as 3 of the 23 cases in the salivary gland group and 1 of the 28 thyroid cases. Additionally, 2 of 12 neck node aspirations and 2 of 24 salivary gland aspirations diagnosed as benign revealed NHL at surgery.
Core-Needle Biopsy
Several studies evaluating core-needle biopsy for lymphoma diagnosis have been published.13–16 In one study, 241 patients with lymphoma underwent core-needle biopsy as their initial biopsy.13 Overall, an 82.5% success rate was observed. Several studies included both patients undergoing initial evaluation, as well as patients with suspected relapse or progressive disease.14–16 Core-needle biopsy procedures yielded sufficient material for formulation of a treatment plan in 83% to 93% of patients. A recent report of 88 patients undergoing ultrasound-guided core-needle biopsy for head and neck masses included 16 patients with a final diagnosis of lymphoma.17 In 3 of 16 patients inadequate tissue was obtained by core-needle biopsy, and the patients had subsequent excisional biopsies. In 12 of 13 with “adequate” tissue to make a diagnosis of lymphoma, full subclassification of the lymphoma was possible and treatment initiated on the basis of the core-needle biopsy. Importantly, these 12 patients did not have an open biopsy to confirm the results of the needle biopsy. Gong and colleagues18 compared results of FNA and core-needle biopsy in 74 patients with lymphoma. FNA with flow cytometry was insufficient in 47% of patients and core-needle biopsy was insufficient in 28% of patients.
Prebiopsy Corticosteroids
Historical teaching dictates that patients with suspected lymphoma should not receive corticosteroids before biopsy because of the theoretic risk of obscured results because of rapid tumor response. In reality, except in the rare case of lymphoblastic lymphoma, steroids are unlikely to have a significant detrimental effect if tissue is obtained within 24 to 48 hours of the first dose. In one study of 86 children with mediastinal lymphoma, 23 received prebiopsy corticosteroids. In five (22%) an adverse effect on the pathologic diagnosis was observed, one patient with HL and four with probable lymphoblastic lymphoma.19 However, the only indication for prebiopsy steroids should be severe, life-threatening airway compromise. Although patients with SVC syndrome can be quite symptomatic, these symptoms are not life threatening over the short term and steroids should not be administered until diagnostic tissue is obtained. If lymphoblastic lymphoma is suspected, every effort should be made to obtain tissue within 1 day of presentation and before administration of steroids.
Nodal Lymphomas of the Head and Neck
Hodgkin’s Lymphoma
As described earlier, most patients with HL present with asymptomatic peripheral adenopathy, most commonly cervical and supraclavicular. The incidence peaks between 15 and 40 years of age. Severe, generalized pruritus is common in HL, rare in NHL, and often precedes the diagnosis by months. Systemic symptoms including fever of greater than 38° C for 3 consecutive days, drenching night sweats, or unexplained weight loss of more than 10% of body weight in the preceding 6 months occur in about 25% of patients with HL, but they are uncommon in early-stage disease.20 Pruritus, systemic symptoms, and many of the laboratory abnormalities seen in HL are probably a result of cytokine production by Reed-Sternberg cells.
HL is a neoplastic proliferation of Reed-Sternberg (R-S) cells or R-S variants, large cells with abundant cytoplasm and multiple or multilobed nuclei. R-S cells are surrounded by host inflammatory cells including lymphocytes, plasma cells, neutrophils, and eosinophils. R-S cells are derived, in most cases, from germinal center B cells.21 The World Health Organization classifies HL as either “classic” HL or nodular LPHL. LPHL and classic HL have different natural histories, prognoses, and treatments.21 Immunohistochemical studies accurately distinguish LPHL from classical HL and should be performed if histology is equivocal. In classical HL, the large atypical cells generally express CD15 and CD30, whereas other T- and B-cell–associated antigens are usually negative. In contrast, the tumor cells of LPHL are CD20+ (a pan-B-cell antigen), CD45+ (leukocyte common antigen), CD15−, and variably reactive for CD30, an immunophenotype often seen in B-cell NHL. Flow cytometry is nondiagnostic in HL.
Staging
The Ann Arbor staging system for HL and NHL is detailed in Table 119-2. The designation E applies to extranodal involvement, which is limited in extent and contiguous with lymph node disease. Extranodal involvement of HL of head and neck sites is extremely rare. Proper staging requires computed tomography (CT) scans of the chest, abdomen, and pelvis. CT scans of the neck are optional and probably add little to a thorough physical examination but may aid in designing radiotherapy portals if radiotherapy is planned. The mediastinal mass ratio (MMR), defined as the ratio of the maximal transverse diameter of the mediastinal mass to the maximal transverse intrathoracic diameter, is an important prognostic factor and should be calculated in all patients with significant mediastinal adenopathy. An MMR greater than 0.33 by chest radiograph (CXR) or 0.35 by CT portends a worse prognosis and may influence treatment recommendations. Positron emission tomography (PET)/CT upstages and potentially alters treatment in 10% to 20% of patients with HL compared with CT alone and should be considered in the initial staging of patients with early-stage disease.22,23
Table 119-2 Ann Arbor Staging System for Lymphoma*
| Stage I | Involvement of a single lymph node region or lymphoid structure, or involvement of a single extralymphatic site (IE) |
| Stage II | Involvement of 2 or more lymph node regions on the same side of the diaphragm, which may be accompanied by localized contiguous involvement of an extralymphatic site or organ (IIE) |
| Stage III | Involvement of lymph node regions on both sides of the diaphragm, which may also be accompanied by involvement of the spleen (IIIS) or by localized contiguous involvement of an extralymphatic site or organ (IIIE) |
| Stage IV | Diffuse or disseminated involvement of 1 or more extralymphatic organs or tissues, with or without lymph node involvement |
* The absence or presence of fever (>38° C), unexplained weight loss (>10% body weight), or night sweats should be denoted by the suffix letters A or B, respectively.



