 n unusual-looking nodule at the limbus should always lead you to suspect a malignancy, and it must be removed in toto. It is important to achieve clean margins when removing these nodules, so as not to leave any tissue that might prove malignant later on. A nodule may have excessive vascularity, which must be addressed during excision. Bipolar cautery or heat cautery can serve this purpose, but these often cause unnecessary trauma to the tissues. The following cases illustrate how the Fugo blade can be used in removing limbal nodules.
n unusual-looking nodule at the limbus should always lead you to suspect a malignancy, and it must be removed in toto. It is important to achieve clean margins when removing these nodules, so as not to leave any tissue that might prove malignant later on. A nodule may have excessive vascularity, which must be addressed during excision. Bipolar cautery or heat cautery can serve this purpose, but these often cause unnecessary trauma to the tissues. The following cases illustrate how the Fugo blade can be used in removing limbal nodules.
CASE STUDIES
Case 1
A 60-year-old farmer had noticed the formation and growth of a “white thing” at the limbus for over 6 months. A 5-mm hard white lesion sitting astride the lateral limbus appeared heavily vascularized.
TECHNIQUE
Anesthesia
Make a hole was made in the conjunctiva with a 100-µm Fugo blade tip. Administer lignocaine 2% through a cannula to inflate it around the lesion.
Surgical Technique
- Use a hockey-stick knife to separate the nodule from the corneal side (ours succeeded only partially).
- Incise the conjunctiva all around the lesion with a 300-µm Fugo blade tip at low energy and medium power setting.
- Push the lesion and cut toward the limbus with the same tip. Remove only the top layers.
- Lift the remaining tissue over the surface of the sclera with a forceps and perform ablation until the field became reasonably clean (Fig. 12.1).
- Remove the nodular tissue remaining on the cornea with a fine forceps. Then use a 600-µm Fugo blade tip a medium power and energy to clear and polish the cornea, limbus, and exposed sclera. Rub the activated tip under a stream of saline, removing the remaining lesion without excessive loss of healthy tissue.
- Leave the sclera bare for coverage by the conjunctiva in the postoperative period.
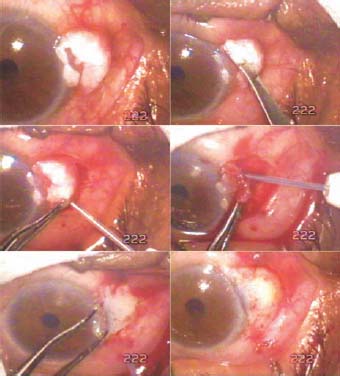
Figure 12.1. A hard nodule at the limbus. The hockeystick knife was ineffective. The nodule is dissected free of the underlying tissues with a 300-µm Fugo blade tip, and the base of the nodule is polished clean with a 600-µm Fugo blade tip.
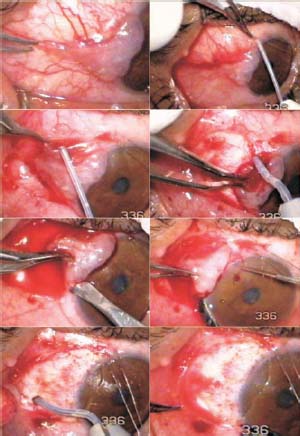
Figure 12.2. A fleshy vascularized mass is at the limbus. The mass is lifted with lidocaine after making a conjunctival hole with 100-µm Fugo blade tip. The fornix side is cut, lifted, and dissected toward the limbus. Next the limbal side is lifted and the whole mass is removed. The based is cleaned and polished with the 600-µm Fugo blade tip.
Postoperative Management
Prescribe mitomycin 0.02% for instillation seven to eight times a day for a period of 7 days, along with antibiotic–steroid ointment three times a day. In our case, the histologic examination report received after 1 week was negative for malignancy, and the patient had an uneventful recovery.
Case 2
A 57-year-old truck driver presented with a fleshy vascularized nodule on the medial side of the cornea. The appearance of the nodule was unusual, almost the reverse of a commonly seen pterygium with the fleshy base situated toward the cornea and the apex toward the medial canthus. The nodule was removed in a manner similar to that used in Case 1 (Fig. 12.2). The histologic examination report received after 1 week was negative for malignancy. This patient, too, had an uneventful recovery.
Summary
Use of the Fugo blade to remove unusual limbal lesions has one great advantage: the ability to remove the finest visible remains of pathologic tissue with greater accuracy and with minimal damage to normal tissue.
Suggested Reading
Kellan R, Fugo RJ. Device increases safety, efficiency of cataract surgery. Ophthalmol Times. 2000;25:7–9.
Roy FH. Course for Fugo blade is enlightening, surgeon says. Ocular Surg News. 2001;19:35 38.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


