Chapter 19 Lids: Congenital and acquired abnormalities − practical management
Management of congenital lid conditions
Lid coloboma
The coloboma is described in terms of its position using the Tessier classification, and in terms of its extent.1 An examination is carried out to exclude associated ocular and systemic abnormalities. Initial management aims to protect the ocular surface with lubrication and occlusive dressing taking care not to induce amblyopia with them. A forced duction test is performed on all children with an eyelid coloboma for underlying adhesions2 which need early treatment. This should be carried out early and it usually requires an examination under anesthesia. A small coloboma can be closed under the same anesthetic. If a more complicated repair is required, timing depends on the underlying ocular surface protection but delaying repair allows growth of soft tissues increasing options for advancement and closure. If corneal exposure cannot be controlled, the eyelid reconstruction is urgent. A defect less than 25% of the lid length can be repaired by excision of the coloboma margins and direct closure. For defects of 25–50% of lid length, a lateral canthotomy and cantholysis allows the wound edges to come together. For defects of 50% or more, tissue will need to be added from elsewhere. In the lower eyelid, the posterior lamellar can be reconstructed using tarsoconjunctival grafts from the upper lid, together with advancement myocutaneous eyelid flaps or skin grafts. Eyelid sharing procedures are better for older children or eyes in which there is no visual potential, due to the risk of occlusion amblyopia. They may be necessary in cases of uncontrolled exposure; in these circumstances the flap should be divided after 2 weeks, and followed with aggressive occlusion therapy.
The coloboma in Treacher-Collins syndrome (see Chapter 18) is a pseudocoloboma in which there is a defect of subcutaneous tissue rather than a true eyelid discontinuity. The syndrome is variably severe, including an abortive form. Severe cases may require craniofacial surgery prior to eyelid surgery in order to re-establish malar support. In less severe cases, the lids can be built with oculoplastic surgery alone. In mild cases, the lateral canthus can be repositioned with a lateral canthoplasty, but extensive undermining and repositioning of the periocular soft tissues is necessary to maintain the new canthal position. In moderate cases, with absence of vertical and horizontal eyelid soft tissue, the lid can be reconstructed with the use of hard palate mucous membrane grafts or ear cartilage to support the lid. The lateral canthus can be secured with wire fixation to bore holes in the lateral orbital rim. Moderately severe cases may require transposition flaps from the upper to lower lids with a lateral canthal strip.
Cryptophthalmos
Cryptophthalmos is a rare condition in which the upper eyelid and eyebrow fail to develop and the cutaneous epithelium is continuous with conjunctiva at the superior fornix. There is usually severe dysgenesis of the anterior segment as well. The condition can be complete, incomplete, or partial (congenital symblepharon) (see Chapter 18).
In complete cryptophthalmos there is no real chance of gaining vision even with reconstructive surgery. In incomplete cryptophthalmos there may be some chance of achieving useful vision or reasonable cosmesis, but this is unusual: then the same concerns pertain as in eyelid colobomas. The urgency of surgery depends on whether the condition is unilateral or bilateral, the presence of visual potential, and the degree of corneal exposure. If the condition is unilateral, no visual potential exists, and exposure is controlled, surgery should be delayed to allow for the relaxation of tissues, which occurs as the infant matures.3
Ablepharon
Complete failure of eyelid development is rare (see Chapter 18). Urgent treatment is required to protect the ocular surface followed by early lid reconstruction. The results depend on the severity of the lid changes and the integrity of the underlying structures. Treatment of true ablepharon has poor results; however, treatment of milder cases (microblepharon), by vertical stretching of the lid and anchoring at the lateral orbital rim, is more successful. Although the eyelid may open minimally initially due to “bow-stringing” of the tight eyelid, this improves significantly within 6−8 weeks of surgery.
Ankyloblepharon
In ankyloblepharon (see Chapter 18) the eyelid margins are partially or completely fused together with a reduction in the palpebral aperture. Ankyloblepharon filiforme adnatum is a similar condition in which one or more skin tags join the two lids and there is usually a normal horizontal palpebral aperture: it is treated by division of the tag or tags.
Euryblepharon
Euryblepharon (see Chapter 18) is congenital primary enlargement of the palpebral aperture, usually greatest laterally. There is a localized outward and downward displacement of the lateral canthus and downward displacement of the lower lid. Mild cases may require no treatment or simple lubrication. If there is a danger of corneal exposure, the lateral canthus may be tightened and positioned more superiorly and posteriorly. Wide undermining and repositioning of the soft tissues is necessary or the tissues tend to migrate to their original location. If the eyelid is short vertically, skin grafts and/or posterior lamellar grafts with overlying soft tissue advancement may be required. Free grafts usually result in suboptimal cosmesis in young children.
Ectropion
The initial treatment of ectropion in childhood is conservative, using lubrication to prevent exposure keratitis. Surgery is aimed at treating the underlying cause: shortage of skin or increased lid laxity (paralytic ectropion is discussed later) and is usually delayed until the child is older and has more soft tissue with which to work. Ectropion associated with a shortage of skin occurs in congenital conditions such as Down’s syndrome, blepharophimosis (Fig. 19.1), and acquired conditions such as ichthyosis, dermatomyositis, and trauma. A localized scar can be lengthened with a Z-plasty, and a generalized shortage of skin corrected with a skin flap or graft. Increased lid laxity causing ectropion is found in congenital conditions such as megaloblepharon and euryblepharon and can occur after trauma. It is treated with lid-shortening procedures.4

Eversion
Treatment of congenital eversion (see Chapter 18) is aimed at repositioning the everted eyelids so that the underlying soft tissue swelling and chemosis can resolve. Once this has occurred, the eyelids remain in proper position. Repositioning the eyelids and pressure patching or taping for 5−7days is usually sufficient. More severe cases can be treated by intermarginal sutures.
Epiblepharon
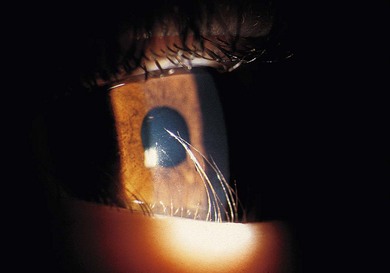
Epiblepharon is a horizontal fold of skin across the upper or lower eyelid that may push the lashes against the cornea (see Chapter 18). The lid margin remains in a normal position. Epiblepharon usually resolves by 5−6 years of age as the facial bones grow. It is usually asymptomatic and is seldom associated with keratitis (Fig. 19.2). Surgical intervention is reserved for those patients in whom it causes corneal compromise despite conservative treatment (i.e. lubrication) or it persists into adolescence. Quickert sutures can be used in milder cases, or excision of an ellipse of skin and orbicularis muscle with tarsal fixation is used in more severe cases.5,6
Entropion
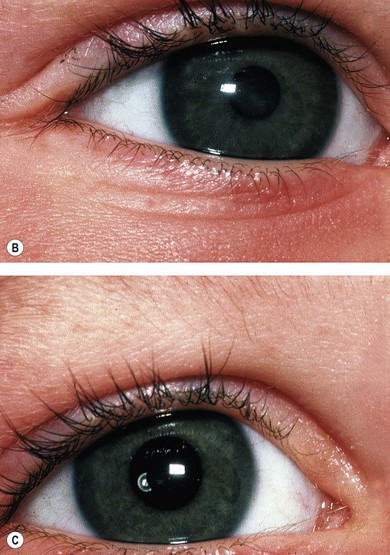
In congenital entropion (see Chapter 18), the eyelid margin is inverted (Figs 19.3 and 19.4). This often requires prompt surgical intervention to prevent corneal infection and scarring. It should be distinguished from epiblepharon, where a skin fold causes a secondary turning of the lower lid lashes. Surgery is directed toward re-everting and stabilizing the eyelid with excision of skin and orbicularis, reattachment of the lower eyelid retractors to the inferior border of the tarsus, and then re-fixating the skin edges to the inferior tarsal border.



Tarsal kink/upper lid entropion
Congenital upper lid entropion is rare but often associated with a horizontal kinking of the tarsus. As with lower lid entropion, there is a risk of corneal scarring and infection. It can be corrected by incising the tarsus along the kink, and then repositioning the anterior lamella of the eyelid (Fig. 19.5).


Epicanthal folds
Epicanthal folds are folds of skin which extend from the upper eyelid toward the medial canthus. The fundamental difference between epicanthal folds and epiblepharon is that epicanthal folds are caused by a relative shortage of skin where the soft tissue is stretched tautly between the medial eyelid and the medial canthus instead of following the contour of the nasal angle. Epicanthal folds only require urgent treatment if they cause trichiasis or obstruct vision. They are largely an esthetic issue and become less prominent with development of the bridge of the nose and stretching of the overlying skin. As the folds represent lines of skin shortage, they can be broken up and lengthened with various different flaps. A simple epicanthic fold can be treated with a Z-plasty. Two separate Z-plasties can be used when a fold affects both the upper and lower lids. A mild epicanthic fold associated with telecanthus can be treated with a Y–V plasty and shortening of the underlying medial canthal tendon. If there is a marked epicanthic fold associated with telecanthus, a double Z-plasty can be combined with a Y–V plasty.7,8
Telecanthus
Telecanthus is an increased width between the medial canthi, with a normal interpupillary distance. If there is an overgrowth of bone with an increase in the interorbital width the condition is referred to as hypertelorism. Telecanthus can usually be improved by shortening the medial canthal tendons without involving a significant reduction in bone.9 Mild cases can be treated by medial canthal plication with a non-absorbable or wire suture combined with a Y–V plasty. More severe cases may require transnasal wiring combined with a Y–V plasty. Posterior placement of the wire is necessary for a good cosmetic result. The thickness of the anterior lacrimal crest and medial orbital wall bone can be reduced with a burr at the same procedure. If a transnasal wire is required, it is essential to have preoperative radiologic evidence of the height of the cribriform plate to avoid damage to the intracranial structures. The correction of hypertelorism requires craniofacial surgery to mobilize the orbital rims and reduce the intervening ethmoid bones.
Blepharophimosis
“Blepharophimosis” means small eyelids. In the blepharophimosis syndrome, the horizontal palpebral aperture is reduced and this is associated with epicanthus inversus, ptosis, and telecanthus (see Chapter 18).
Treatment is directed toward promoting visual development and improving cosmesis. Patients should be refracted and amblyopia and strabismus are common.10 Resting lid position determines the urgency of ptosis correction. If a marked ptosis contributes to amblyopia, either by obstructing the visual axis, or by inducing astigmatism, ptosis surgery is urgent.
The treatment of blepharophimosis syndrome is staged. Hypertelorism, epicanthus inversus, and telecanthus can be repaired at one sitting. Various techniques have been described to rearrange the medial canthal tissues, but a simple Y to V advancement with medial canthal tendon plication, or, in the case of more severe telecanthus, transnasal wiring, is most effective. In addition, the epicanthal folds generally improve with development of the mid-face. Ptosis surgery is done as a second procedure because correcting the telecanthus may worsen the ptosis. Moreover, levator function is usually very poor; thus, if there is no risk of amblyopia, ptosis surgery can be delayed until the child is sufficiently developed to carry out a brow suspension with autologous fascia lata or temporalis fascia (Fig. 19.6).


Management of congenital and acquired ptosis
History and examination
Chapter 18 reviews the various causes of congenital vs. acquired ptosis. A careful history to confirm the congenital or acquired nature of the condition and associated phenomenon is important. With congenital ptosis the parents may report that the condition seemed to improve initially after birth and then plateaued after a few months.
A full eye examination should be performed, with attention to the position of the lid on downgaze, levator excursion from down- to upgaze, extraocular motility, facial or eyelid dysmorphism or mass, aberrant movements of the lid associated with extraocular excursions or jaw movement, pupillary size and reactivity, and variability in eyelid height. Best corrected visual acuity, fixation preference, and retinoscopy or subjective refraction should be performed to rule out associated amblyopia. Further investigations may be indicated, for instance with third nerve palsies or congenital Horner’s syndrome.11
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


