Chapter 20 Lid and orbital infantile peri-ocular hemangiomas (capillary hemangiomas) and other vascular disease
Vascular lesions of the orbit include tumors such as capillary and cavernous hemangiomas and hemangiopericytomas together with malformations such as venous-lymphatic malformations (lymphangiomas), orbital varices, and arteriovenous malformations. Infantile peri-ocular hemangiomas (capillary hemangiomas), common benign vascular tumors, are characterized by rapid growth during the first year of life and show regression over the next several years1,2 Cavernous hemangiomas and hemangiopericytomas are predominantly seen in adults, but may rarely cause proptosis in childhood. Venous-lymphatic malformations (lymphangiomas) are vascular malformations that infrequently present in early childhood and are complicated by bouts of hemorrhage and rapidly progressive enlargement. Varices and arteriovenous malformations primarily present in the second and third decades.
Tumors
Infantile peri-ocular hemangioma (capillary hemangioma)
Infantile peri-ocular hemangioma (capillary hemangioma), a hamartoma, is the most common childhood orbital tumor. It occurs more frequently in females than males in a ratio of 3 : 23 with no inheritance pattern. Its incidence is increased by prematurity.4 It is distinguished from other orbital vascular lesions by spontaneous regression. Numerous techniques are available to manage this potentially disfiguring disorder which affects vision: there is no “one size fits all” approach for this unpredictable tumor; patients whose lesion resolves rapidly with treatment could have done so without treatment. We are fearful of uncontrolled growth, as seen in Fig. 20.1. Treatment of periocular hemangiomas is a team effort involving pediatricians, dermatologists, and ophthalmologists. Decisions to treat using propranolol, systemic or intralesional steroids, or surgery are based on the position of the lesion, the presence of amblyopia, rapidity of growth, and discussion of risk/benefits with informed parents. Children must be followed closely, watching for rebound growth and checking for amblyopia.

Its histopathology varies with its clinical phase; in its early proliferative phase, it consists mostly of numerous dividing endothelial cells; vascular spaces are rare and small. It is rich in mast cells, whose function is not clear. There may be numerous mitotic figures which could lead to an incorrect diagnosis of malignancy in rapidly enlarging lesions. The characterization of poorly differentiated lesions may be helped by reticulin stains or by the identification of factor VIII, which is produced by the endothelial cells, using peroxidase or fluorescein antibody techniques.3 In more mature tumors, vascular spaces are larger, with fewer flattened endothelial cells. The tumor is not encapsulated and tends to infiltrate surrounding structures. In the involutional phase, the endothelial cells are replaced by adipocytes and there is deposition of fibrous tissue.
The natural history of infantile peri-ocular hemangioma (capillary hemangioma), rapid enlargement followed by spontaneous involution, is unique for vascular tumors. Their vascular endothelium expresses placenta-associated antigens,5 not expressed by other vascular tumors or normal skin, which has led to speculation that infantile hemangiomas develop either because of angioblasts abnormally differentiating toward placental vascular phenotypes or as the result of placental cell embolization of fetal tissues.5 The presence of maternal–fetal microchimerism for infants with solitary hemangiomas was supported by a subsequent molecular genetic study.6 Recently, the potential role for hypoxia in hemangioma development has been stressed.7
Clinical features
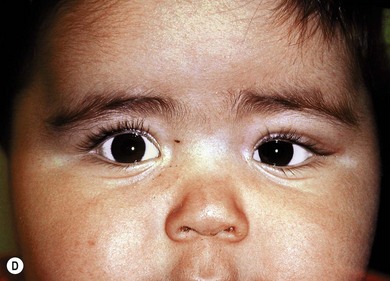
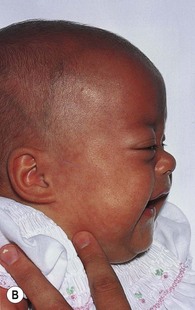
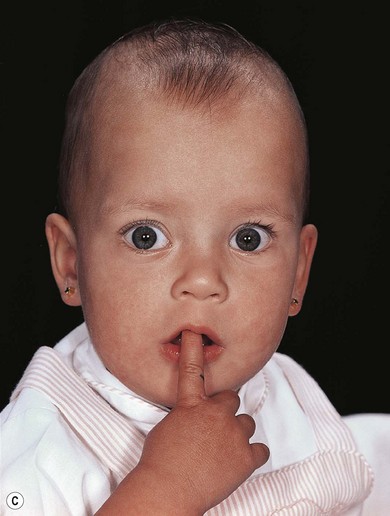
One-third of infantile peri-ocular hemangiomas (capillary hemangiomas) (Fig. 20.2) are present at birth; all have appeared by the age of 6 months. The appearance of the tumor may be preceded by a faint cutaneous flush. Usually, rapid growth lasting 3 to 6 months is followed by a period of stabilization and then regression (Fig. 20.3). Margileth and Museles1 found that 30% of 336 hemangiomas had regressed by the age of 3 years, 60% by 4 years, and 76% by 7 years.



Infantile peri-ocular hemangiomas (capillary hemangiomas) are most commonly in the upper lid or orbit (Fig. 20.3). Their appearance varies according to the depth of involvement (Fig. 20.3A); superficial cutaneous lesions have a red lobulated appearance, giving rise to the name “strawberry” nevus (see Fig. 20.8A). These superficial lesions consist initially of a confluence of telangiectasias that progress to raised, nodular lesions. They may enlarge and become blueish in color with crying. Subcutaneous hemangiomas are often blueish in color. Lesions situated deep to the orbital septum may present with proptosis without cutaneous discoloration. Occasionally, the proptosis is severe enough to cause corneal exposure. One-third of hemangiomas involve several levels of depth. A deeply situated lesion causing only proptosis with no cutaneous signs may present a diagnostic dilemma. A helpful diagnostic sign is the increase in proptosis with crying (Fig. 20.2). In 30% of patients, “strawberry” nevi are found at other cutaneous sites.2 Occasionally, enormous growth occurs obliterating facial structures (Fig. 20.1).
Amblyopia is common with orbital infantile peri-ocular hemangioma (capillary hemangioma), with a prevalence between 43% and 60%.2,8 Rarely, this results from occlusion of the visual axis by a bulky tumor. More often it results from distortion of the globe by tumor causing corneal astigmatism. The axis of the corrective plus cylinder is directed toward the tumor. This may persist after the hemangioma has regressed but usually resolves, at least partially, particularly if the hemangioma resolves or is treated early.9,10 Prolonged occlusion can result in ipsilateral myopia and the resultant anisometropia may be another amblyogenic factor. Secondary strabismus is common as a result of the interruption of binocularity or displacement of the globe by the tumor.
Systemic complications of infantile peri-ocular hemangiomas (capillary hemangiomas) are rare:3
1. Kasabach-Merritt syndrome: a potentially life-threatening coagulopathy resulting from consumption of fibrinogen and platelet entrapment within a large vascular hemangioma. It usually responds to platelet replacement and corticosteroids.
2. PHACE(S) syndrome (posterior fossa abnormalities, hemangioma, arterial lesions, cardiac abnormalities, eye and sternal abnormalities) with serious cardiovascular and neurologic complications and frequent ocular involvement including amblyopia, strabismus, anterior polar cataract, ptosis, and optic neuropathy.11 A careful ocular, cardiac, and neurologic examination is necessary for patients with extensive facial infantile peri-ocular hemangiomas (capillary hemangiomas).
Investigation
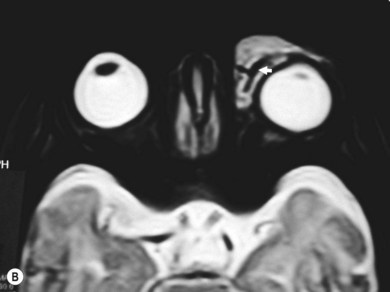
Doppler ultrasound may help to secure the diagnosis.12 The extent of the lesion can be assessed by computed tomography (CT) scanning. A soft tissue density mass is seen to infiltrate the orbit, with smooth or nodular margins, often crossing boundaries between compartments such as the muscle cone or orbital septum. Bony erosion may be seen. Enhancement is variable, according to the vascularity of the lesion and its stage of development. T2-weighted magnetic resonance imaging (MRI) is useful to delineate the tumor since the lesion is hyperintense due to its intrinsic blood flow (Fig. 20.4). T1-weighted gadolinium-enhanced views with fat suppression to improve contrast give the best assessment of the anatomic relationships of the tumor. Obtaining an magnetic resonance angiogram and venogram (MRA and MRV) at the time of the MRI may rule out other vascular anomalies that can mimic hemangiomas. Lesions confined to the posterior orbit, especially during a period of growth, may occasionally be mistaken for a malignant tumor such as rhabdomyosarcoma; biopsy may be indicated.


Management
Management should be conservative, with treatment of significant refractive error and amblyopia while awaiting spontaneous regression (Fig. 20.5). The appearance of superficial pale stellate areas of scarring (“Herald spots”) on a “strawberry” lesion is a useful early indicator of spontaneous regression. Amblyopia therapy should be accompanied by spectacle correction of the astigmatic error of the affected eye with appropriate glasses (Fig. 20.6).


Active treatment to reduce the size of the tumor is only indicated if there is occlusion of the visual axis or if a posterior lesion results in progressive proptosis with optic nerve compression, corneal exposure, and significant or progressive amblyopia. Methods of treatment include topical or systemic beta-blockers,15–17 local or systemic steroids,10,13,14 surgical excision,18 radiotherapy, laser,19 and injection of sclerosing agents.
A dramatic reduction was noted in the size of infantile peri-ocular hemangiomas (capillary hemangiomas) in children treated with propranolol (Fig. 20.7) for cardiac disorders.20 At doses of 1–3 mg/kg/day, a response may be seen within a few days. Subsequent studies have shown a response rate of up to 90%; side-effects such as hypotension, bronchospasm, bradycardia, heart block, and hypoglycemia can be avoided with careful monitoring.15,16 This observation has revolutionized the treatment of hemangiomas; beta-blockers are now the first choice for most ophthalmologists. Topical timolol 0.5% also has been reported to be effective, and with far fewer side-effects than with systemic beta-blockers is appealing.17 Randomized trials comparing systemic and topical propranolol to corticosteroids are ongoing.


Nowadays steroids are considered a useful but ‘second line’ alternative to beta-blockers. Kushner21 reported good results with injection of local steroid into the hemangioma. The steroid should be injected slowly throughout the tumor while the needle is withdrawn to reduce the risk of central retinal artery embolization,22 a rare complication. Tumor regression should be noted within 2–4 weeks, and further injections may be necessary (Fig. 20.8). Other complications include local fat atrophy, skin hypopigmentation, eyelid necrosis, and periorbital calcification. While systemic side-effects are less common with intralesional rather than systemic steroids, care must be taken to make certain that adrenal insufficiency does not occur during concurrent illness, trauma, or surgical stress.3,13 Ultrasound guidance may be helpful for posteriorly situated lesions.23 The whitish skin discoloration that is sometimes noted from superficial accumulation of depot steroid after injection is usually transient. The risk of dissemination of vaccines should lead to discussion with the pediatrician of infants about to have systemic or intralesional steroid treatment.

Systemic steroids (1.5–5.0 mg/kg/day) may be preferable for very extensive or posteriorly situated lesions (Fig. 20.9). The exact dose is undetermined. However, the response of over 90% for doses greater than 3 mg/kg/day falls to less than 70% for doses of 2 mg/kg/day and less.13 The side-effects of growth retardation, gastrointestinal bleeding, behavior changes, and adrenal suppression may make this therapy less desirable. A rebound increase in size has been noted after discontinuation of oral steroid.

Sight-threatening lesions which have failed to respond to steroids or beta-blockers may be amenable to treatment with interferon alpha 2a,24,25 although the response to this treatment may be slow and the side-effects uncertain in infants. Other immunomodulators, vincristine and cyclophosphamide, have been used to treat hemangiomas (primarily visceral). Their use in treating infantile orbital infantile peri-ocular hemangiomas (capillary hemangiomas) seems limited.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


