Chapter 64 Leukemia
Introduction
Common sites of disease at presentation are bone marrow, blood, lymph nodes, liver, and spleen. The eye is the only site where the leukemic involvement of nerves and blood vessels can be directly observed and it may act as a “sanctuary” for leukemic cells against chemotherapy. Eye complications may occasionally be the major residual disability1 but serious eye involvement is unusual.2 Ophthalmic manifestations may be dramatic, requiring prompt diagnosis and treatment and are more a feature of relapse than of initial presentation. The ocular manifestations of acute leukemia are divided into direct (infiltration of the anterior segment, the orbit, or the CNS) and indirect (secondary to hematologic changes such as hyperviscosity, anemia, thrombocytopenia, and immunosuppression).3
Orbital leukemia is a small, but significant cause of proptosis in children4 and is more likely to be found in uncontrolled disease, in the first decade and with AML. It is associated with higher mortality. Orbital presentation may occur without eye involvement and it may be the only manifestation, especially in AML. Myeloid leukemia may present as an isolated solid tumor mass (granulocytic sarcoma) at a variety of sites, including the orbit (Fig. 64.1). A greenish tinge to the tissue mass led to the term chloroma: this appearance may be due to myeloperoxidase or altered blood products.

Orbital involvement in leukemia may be due to bone or soft tissue infiltration, tumor formation, or hemorrhage; the lacrimal gland, or lacrimal drainage apparatus may be primarily involved, with a more benign diagnosis. Children with orbital involvement present with proptosis, chemosis, and, rarely, muscle involvement; these may occur early in the disease. Exposure keratitis may occur. It may be difficult to differentiate between primary leukemic infiltration and complications such as hemorrhage or opportunistic infection; a biopsy may be necessary.5 A biopsy should be from the center of the abnormal area, not from the periphery where secondary inflammatory changes may occur. Review of the blood count and blood film by a pediatric oncologist, and a thorough clinical assessment prior to biopsy, together with a bone marrow examination at the time of biopsy, are important steps.
Lids
The lids are usually only involved as a part of orbital infiltration, but can be due to direct leukemic infiltration.4
Conjunctiva
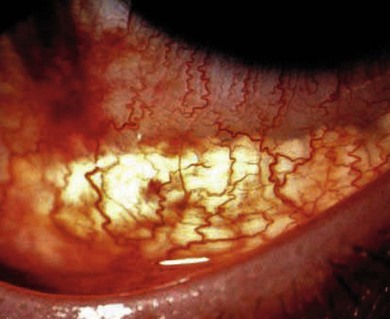
The conjunctiva may be involved by hemorrhage (Fig. 64.2), infiltration (Fig. 64.3), or hyperviscosity, when the vessels are tortuous or comma-shaped. Conjunctival mass formation, though rare, can be the presenting sign in acute leukemia.3

Cornea and sclera
Being avascular, the cornea is not often involved in the leukemias, but it may be involved in herpes simplex or zoster in the immune-compromised child, or by other inflammatory disease. Corneal ulcers may be the presenting sign in acute leukemia6 and perilimbal infiltrates have been described in acute monocytic leukemia.7
Lens
Cataracts occur frequently in patients who have had total body irradiation, related to the total dose and to the rate and fractionation of administration.8 The use of steroids to treat graft-versus-host disease may cause or exacerbate cataracts.
Anterior chamber, iris and intraocular pressure
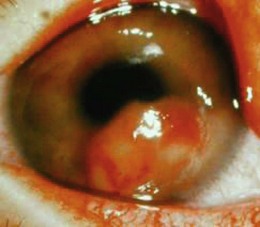
Most reported cases have been of relapse in ALL (Fig. 64.4) but, rarely, children present with a leukemic hyphema or hypopyon. In ALL, anterior segment relapse accounts for up to 2% of all relapses; it is very rare in AML.4,9
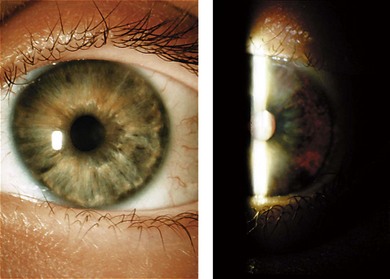
The infiltration is most likely to be blood-borne rather than CNS related9 and the relatively frequent occurrence of isolated anterior segment relapse supports the concept of the eye as a sanctuary site.10 Because of the blood–eye barrier, chemotherapeutic agents do not penetrate the eye so well as at many other sites, allowing leukemic cells to survive, causing signs and symptoms after chemotherapy has stopped. Symptoms include redness, watering, photophobia, pain, and visual loss. The parents may notice changes in the shape or reactions of the pupil or in the color and appearance of the iris (Fig. 64.5). Leukemia accounts for 5% of pediatric uveitis3.

Secondary glaucoma is common and is associated with corneal edema, pain, and redness.
The iris may be thickened diffusely (Fig. 64.6) or in the form of one or more nodules or a mass of variable size; the thickening of the iris obliterates the iris crypts and may give a rather featureless iris. The iris may also be thinned with loss of pigment (Fig. 64.7). The iris color may be changed, usually by a brownish discoloration. Rubeosis may occur. It is often the failure of standard treatment for uveitis that draws the ophthalmologist’s attention to the underlying leukemia. If in diagnostic doubt, perform anterior chamber paracentesis and iridectomy:9 a paracentesis alone may not be sufficient to give an accurate diagnosis. Pathologic studies show leukemic infiltration of the iris and trabecular meshwork,4 and the hypopyon consists of leukemic cells, necrotic tissue, and proteinaceous exudate. Leukemic cells may be difficult to find. Patients with glaucoma have leukemic obstruction of the outflow channels and episcleral vessels.

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


