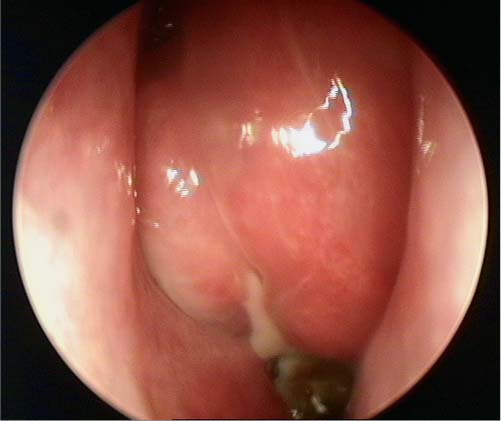
26 Learning from a Difficult Case: Inverted Papilloma Involving the Anterior Wall of the Maxillary Sinus Although an inverted papilloma (IP) is the most common benign neoplasia of the paranasal sinuses, its features have always been controversial. It was thought that it frequently undergoes malignant transformation, that it invades the orbit and the brain, and that it recurs many years after its excision. We know now that this is not true. The initial reports of up to 53% risk of malignant transformation referred (in a significant portion of the cases) to missed ab initio malignant tumors. A retrospective review of 123 cases of IP at the Institute of Laryngology and Otology at Gray’s Inn Road Hospital in London1 showed elegantly how reports of malignant change have decreased at the same time as reports of synchronous malignancy have risen. A review of 2297 cases of documented synchronous and metachronous tumors revealed that the real risk of malignant transformation of IP is ~3%, but the risk of an IP harboring a carcinoma is more than double (7–8%).2 Similarly, 21 cases of an IP invading the brain have been reported in the literature:3 10 of which had SCC, and 9 of the 11 remaining patients had recurrent disease. The cases involving the orbit are rare enough to merit publishing as case reports.4 In terms of timing of recurrence, we now understand that recurrences are mostly cases of residual disease, with 80% of them presenting within 2 years from resection. The management advocated for IP in the seventies was simple intranasal excision, which perhaps unsurprisingly was associated with recurrence rates of up to 71%.5 A decade later, the application of the principles of oncologic head and neck surgery led to more extensive surgery (lateral rhinotomy/medial maxillectomy) being performed—and the recurrence rates plummeted to less than 20%.6 The introduction of the endoscope led to the first attempts at endoscopic removal.7 As more surgeons published their results, it became feasible in 2006 to undertake a meta-analyses of their outcomes.8,9 These meta-analyses looked at 292/353 and 714/1060 cases of endoscopic and open techniques, respectively, and both reached broadly similar results, namely, that the endoscopic approach is associated with better outcomes and lower recurrence compared with the external approach: 12 versus 17% or 12 versus 20%, respectively. However, caution is indicated in interpreting these findings: They were based on simple observational studies which (in the case of the second meta-analysis) lacked nonrandomized or even historical controls. It is also not clear how adequately synchronous tumors were excluded, how many of those treated had recurrent tumors, how thorough was the follow-up, and more importantly, how was selection bias dealt with. At the dawn of the endoscopic excision, the smallest tumors would (logically) have been chosen for endoscopic management. Although these meta-analyses reveal that endoscopic excision has become the current standard, they also make clear that there is a need to standardize excision, follow-up, exclusion of synchronous tumors, and apply staging.10 We feel that a discussion of endoscopic versus external excision can be potentially misleading. The use of an endoscope, per se, tells us about the “endoscopic approach” as much (or as little) as the use of a scalpel tells us about an external approach. What is important is what is removed and how it is removed rather than how it is visualized while being removed. We favor a targeted/step approach, tailoring the excision to the extent of the disease. The IP is endoscopically evaluated and the possibility of creating free margins is checked. The attachment of the IP is determined. The most limited approach possible is chosen. When the IP is attached to the orbital roof or the superior part of the lateral or posterior wall of the maxillary sinus, removal by a normal infundibulotomy is usually possible. Attachments to the lower part of the lateral or posterior wall can sometimes be removed by making a big antrostomy or an extra access through the inferior meatus or the anterior wall. If the attachment is very broad or located at the medial wall of the maxilla, a more radical approach is often indicated with complete removal of the medial wall (medial maxillectomy). The inferior turbinate, is removed when involved by disease or for visualization, as part of medial maxillectomy, whereas the middle turbinate is removed only when involved by the IP. Based on this rationale, we routinely plan surgery after assessing both the computed tomography (CT) and the magnetic resonance imaging (MRI) scans. We specifically look for signs of osteitis, to help us identify the area of attachment to the sinus wall.11 We are prepared to change plans intraoperatively, always aiming to achieve a removal on healthy margins, and ideally en bloc. To attain this, we actively search intraoperatively for the site of attachment of the IP and remove it with a 1-cm cuff of healthy mucosa around it. After the IP removal, the areas of mucosa adjacent to the IP attachment are burned with diathermy and/or the underlying bone is drilled with a diamond burr, to remove microscopic extensions of the IP. Fig. 26.1 Preoperative endoscopic photograph of the tumor in the nasal cavity. Fig. 26.2 Computed tomography scan of the sinuses: note the osteitis sign. Fig. 26.3 Magnetic resonance imaging of the sinuses. A 65-year-old woman presented in our clinic with progressive left-sided nasal obstruction. On rigid endoscopy, a large fleshy polyp was visualized extending through the middle meatus, deflecting medially the middle turbinate and partly obstructing the nasal cavity (Fig. 26.1). A biopsy confirmed the clinical diagnosis of an inverted papilloma. The CT and MRI scans are shown in Figs. 26.2 and 26.3. On the basis of the scans and the histologic report, a medial maxillectomy, anterior and posterior ethmoidectomy was planned. We start by applying topical cocaine powder in cotton buds soaked in 1 mg/mL epinephrine. Initially, we assess the extent of the tumor specifically trying to identify the location and extent of attachment. If we decide that the medial wall has to go because of the broad attachment to the medial wall and floor of the maxillary sinus, we subsequently proceed with a medial maxillectomy (see Video 26.1). In this case, we start by incising the mucosa with a 45-degree disposable keratome knife and subsequently reflect the mucosa over the projected osteotomy sites. A 3-mm chisel is used for both osteotomies, always first anterior to the nasolacrimal duct then under the inferior turbinate. The medial wall of the maxillary sinus is subsequently reflected medially and the nasolacrimal duct identified and cleanly resected with sharp scissors. If necessary, the maxillectomy opening is further enlarged anteriorly and inferiorly with a 15-degree diamond burr and a Kerrison punch, aiming always to completely visualize the anterior wall of maxillary sinus. At this stage, the whole attachment of the papilloma in the maxillary sinus should be clearly visualized. We find that malleable suction elevators are very helpful for removing a 10-mm cuff of normal mucosa around the papilloma attachment. Subsequently, the papilloma is followed in the ethmoids, from the lamina papyracea to the middle turbinate, all the way to the sphenoid ostium. The frontal recess is visualized via a Draf 2a. The sphenopalatine artery is ligated and the papilloma is removed en bloc. The bony maxillary wall where the papilloma was attached is drilled using a 70-degree diamond drill and the cavity inspected with a 70-degree endoscope. We sent all the specimens (including that in the debrider trap) for histology, to avoid missing a synchronous malignant tumor. A complete removal of inverted papilloma is vital, if one is to avoid recurrence and the need for subsequent operations. As shown in this case, we feel that it is frequently possible to perform an en bloc resection and remove completely the tumor using a targeted approach. In the case of maxillary sinus tumors involving the anterior maxillary wall, adequate visualization and subsequently complete removal can be accomplished via a medial maxillectomy (endoscopic Denker), in our opinion in most cases without the need for canine fossa trephination. However, the use of a 30- and 45-degree endoscope and curved drills and shavers is imperative, as is assessment of the whole specimen in the pathology laboratory. • Always assess the papilloma with both CT and MRI. The bony detail included in the CT is important to recognize the presence of intrasinus septa, Haller cells, and the relative depth of the orbit and the nasolacrimal duct; MRI (especially T2-weighted MRI with intravenous contrast) can differentiate between tumor and retained secretions. • It is increasingly recognized that the papilloma attachment can be predicted with some degree of accuracy from signs of osteitis: always try to assess the CT for such signs. • Hypotensive anesthesia and adequate local vasoconstriction are useful for a bloodless field and adequate visualization during the operation. • Try to remove en bloc the medial maxillary wall and the papilloma. Use a3-mm chisel to perform the inferior and anterior/medial osteotomies on the maxillary sinus wall. • Always aim to clearly visualize and cleanly cut the nasolacrimal duct. In our opinion, there is no indication for the routine use of nasolacrimal duct stents. • A70-degree diamond drill and curved suction diathermy are important to completely remove any remnants of the papilloma as well as its attachments in the maxillary sinus walls. • Remember to send the whole specimen (including any parts of the specimen within the debrider trap) for histology. Although the chance of malignant transformation of a papilloma is minimal, the chances of a synchronous malignant tumor are not insignificant.
 Management
Management
 Our Technique
Our Technique
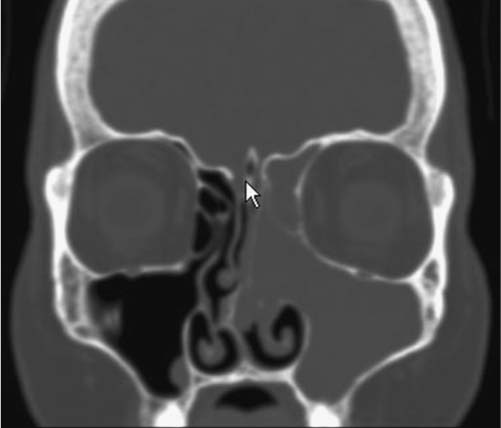
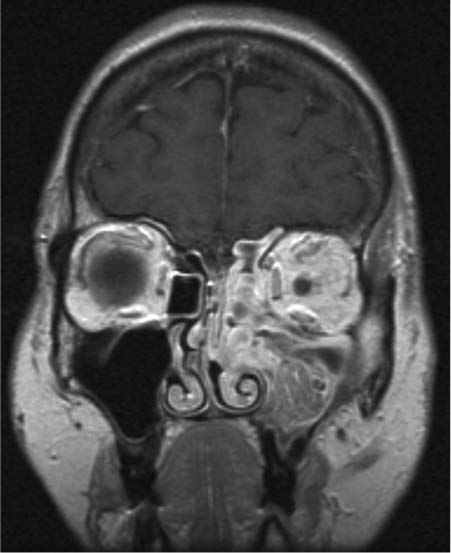
 The Case
The Case
 Discussion
Discussion
Learning from a Difficult Case: Inverted Papilloma Involving the Anterior Wall of the Maxillary Sinus
Pearls
< div class='tao-gold-member'>Only gold members can continue reading. Log In or Register to continue

Full access? Get Clinical Tree


