Chapter 148 Laser Treatment of Choroidal Melanoma
Introduction
Photocoagulation, as introduced by Meyer-Schwickerath in 1949,1 was among the first eye-salvaging treatment methods for choroidal melanomas and the first to make use of a light source. The armamentarium of eye salvaging treatment modalities for choroidal melanomas has significantly enlarged since then, including radiation techniques (brachytherapy, teletherapy with protons, and stereotactic conformal radiation with photons) and surgical excision (transscleral or transretinal). Techniques and light sources for laser treatment of choroidal melanomas have changed as well. Transpupillary thermotherapy making use of infrared lasers at a subcoagulation level was introduced in 1992 by Journée-de Korver and colleagues2 and utilized for primary treatment of small uveal melanomas. Other laser techniques like photodynamic treatment of uveal melanomas were evaluated but still have to be considered as experimental treatment. Although the initial enthusiasm for laser treatment of uveal melanomas has been dampened, laser treatment in all its varieties is a powerful tool in the management of choroidal melanomas when used in selected cases and as an adjunct to other treatment methods. This chapter discusses the current role of laser treatment in the management of choroidal melanomas in relation to the alternative treatment methods currently available.
Laser techniques available for the treatment of intraocular tumors
By convention, photocoagulation is considered to be laser treatment at a temperature level of >75°C. Photocoagulation attempts to destroy a uveal tumor with light from a high-intensity light source, which originally was not a laser but a xenon arc light.3
Non-coagulative laser treatment techniques include low-power long-exposure treatment techniques making use of a conventional argon blue-green laser4 or infrared laser.5 Depending on the wavelength of the laser used the lesions are located deeper in the choroid when infrared or near infrared lasers are used and lesions created by argon blue-green lasers do not extend 1 mm in size while infrared lasers may result in a depth of tumor necrosis of several millimeters.5
Photocoagulation
Photocoagulation treatment is started by circumvallating the tumor with an intensive chorioretinal scar followed by direct treatment of the tumor with high-intensity burns including disruption of the tumor tissue and occasionally appearance of gas bubbles inside the target tissue. As expected, this technique may result in numerous treatment-related retinal complications including retinal breaks, epiretinal membrane formation vascular occlusion and tractional retinal detachment. Moreover, only small tumors can be treated and even in this subset of small tumors a relatively high recurrence rate of uveal melanomas after photocoagulation treatment has been reported. In particular, extrascleral extension of the melanoma may occur growing underneath the fibrous scar overlying the tumor remnants. Consequently, photocoagulation treatment as sole treatment of a uveal melanoma has been abandoned in most centers.6
Transpupillary thermotherapy
Technique
The term “transpupillary thermotherapy” (TTT) was introduced by Journée-de Korver et al.5 to describe a technique in which a near-infrared or infrared light source for long-term exposure laser treatment of uveal melanomas is used. There is controversy in the literature on whether the word “thermotherapy” is appropriate, or whether this treatment technique should be regarded as long-exposure subthreshold photocoagulation using a long wavelength light source, since a whitish-gray discoloration of the target tissue at the end of the procedure is recommended.7 As published by Journée-de Korver et al.5 thermotherapy is different from hyperthermia, which by definition is heating the tumor to a temperature of 42–44°C to enhance the cytotoxic effect of ionizing radiation on tumor cells. In TTT, temperatures of approximately 45–60°C within the tumor are reached with irreversible cytotoxic effects so that additional radiotherapy may be not required.8
Infrared or near-infrared light penetrates deeper into the choroidal tissue than light from argon blue-green lasers theoretically avoiding undesirable coagulation effects in the retina. In contrast to other wavelengths, the absorption of ocular media for infrared is very low (approximately 4–7%).5 Disadvantages include the invisibility of the actual laser beam resulting in the need for an aiming beam and an increased risk of choroidal hemorrhage because of the deeper penetration of the laser light. Numerous light sources based on a semiconductor diode laser are commercially available which may be used for TTT.
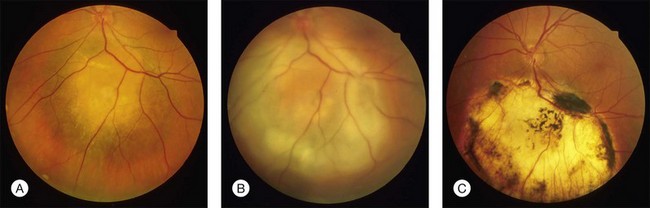
In clinical practice, TTT is performed with retrobulbar anesthesia using a slit lamp and a contact lens. A laser beam with a spot size of 3 mm and a maximal power density of 12 W/cm2 is used. At the second half of the exposure time of at least 1 minute, a grayish discoloration of the tumor tissue should be visible, indicating a temperature of the target tissue of 60–65°C. Ideally, no occlusion of retinal vessels and no coagulation effects in the overlying retina should occur. Three to four treatment sessions are needed which should result in an atrophic scar with central pigment and visible sclera at the treatment site (Fig. 148.1).
Potential complications of TTT are related to the heat delivered to ocular structures and include accidental combustion of the anterior segment, retinal vascular occlusions, retinal and vitreous hemorrhages, macular edema, nerve fiber bundle defects with subsequent visual fields defects and epiretinal membrane formation with traction on the retina.9,10
Experimental data provided evidence that the absorption of heat is enhanced in particular in amelanotic tumors by systemic administration of a chromophore like indocyanine green immediately before TTT.11,12 Although a prospective randomized trial did not find any beneficial effect in supplemental use of indocyanine green in TTT of choroidal melanomas,13 other authors did find enhanced local tumor control when indocyanine was used in combination with TTT.14
TTT as primary treatment of choroidal melanoma
When TTT was introduced in the treatment of choroidal melanoma, short-term follow-up data impressively showed that in appropriate cases tumor regression may be achieved in more than 90%. Tumors considered being appropriate for TTT included melanomas with a largest tumor diameter of <12 mm and not more than 4 mm thickness located posterior to the equator where the clinical diagnosis of a malignant melanoma was established.8,15
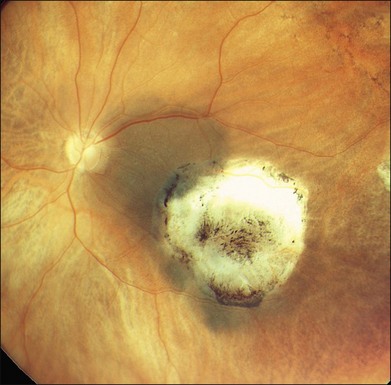
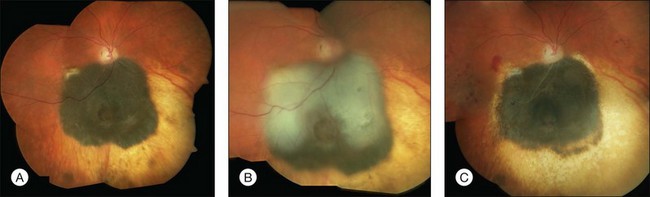
Studies with a longer follow-up, however, have dampened the initial enthusiasm showing that conventional photocoagulation and TTT may be not as different as previously thought.16 Shields and associates were among the first to find that 9% of the tumors developed recurrent growth (Figs 148.2, 148.3).9 Patients with tumors abutting or overhanging the optic disc or those requiring more than three sessions for tumor control were more likely to develop tumor recurrence. Other groups have published similar results in particular in juxtapapillary tumors10,17–23 The pattern of recurrence has been evaluated in a histopathological series of seven eyes enucleated after TTT.24 The authors found a lateral growth of the tumor and an extrascleral extension in five out of seven cases, which were detected only in a single case ultrasonographically. Other groups also reported extrascleral extension after TTT.6,24,25 These findings correlate to similar histologic findings after conventional photocoagulation, making it highly questionable that TTT is advantageous.

Progressive choroidal vascular remodeling and retinochoroidal anastomosis in sequential indocyanine angiograms may indicate recurrent tumor growth after TTT.26,27 These findings suggest that vascular occlusion after TTT is not complete as previously thought, which may explain the high recurrence rate after stand-alone TTT.
These controversial aspects of TTT as sole treatment of choroidal melanomas have recently been reviewed by a group of ocular oncologists.16 They found recurrence rates as high as 56%.19 They concluded that the potential risk for visual loss is lower for TTT compared to local radiation. Local tumor control, however, is insufficient, making TTT not effective for the treatment of small choroidal melanomas.
TTT as ancillary treatment of choroidal melanoma
While stand-alone treatment of choroidal melanomas with TTT is disappointing combined treatment offers promising options.28 TTT as ancillary treatment may be used for several indications including so-called “sandwich therapy,” geographical misses after radiotherapy or surgical excision and insufficient regression or recurrent growth of the tumor (Figs 148.4, 148.5).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


