Laser Surgery in Glaucoma
Howard S. Weiss MD, MPH
Kenneth S. Schwartz MD
Arthur L. Schwartz MD
INTRODUCTION
The word laser is an acronym for light amplification by stimulated emission of radiation. It was only natural that ophthalmologists were among the first surgeons to use therapeutic lasers, since the clear media of the eye, combined with mirrors and lenses, allows the ophthalmic surgeon to direct light energy to treat structures inside the eye. A discussion of introductory laser physics is found elsewhere in these volumes Duanes.
LASER IRIDECTOMY/IRIDOTOMY
History
The ability of light energy to create a hole was demonstrated by Boerhave in the 18th century. He used the thermal effect of light energy focused through a magnifying glass to burn a hole in a piece of paper.1 The terms iridectomy and iridotomy are used interchangeably to describe the creation of a hole in the iris. In 1956, Meyer-Schwickerath reported the use of the light energy of xenon arc photocoagulation to create an iridotomy.2 This technique unfortunately yielded a high incidence of corneal and lenticular opacities. Subsequently, the ruby laser was used to create iridotomies in rabbits and humans.3,4,5 Zweng et al.and colleagues, L’Esperance and Kelly, and Patz,6,7,8 in their pioneering work with continuous-wave argon laser energy, adapted it to be delivered through a slit-lamp system, enabling precise focusing as well as the possibility of treating the iris plane.
The argon laser has a wavelength of 454 to 514 nm and is an intense coherent light beam of pure blue green blue–green color. This wavelength range It is located in the part of the spectrum that is optimal for effective interaction with both hemoglobin and pigment. These properties, and the ability to focus the energy precisely on the plane of the iris, initially made continuous-wave argon laser energy the ideal method of creating holes in the iris.
Several investigators have reported series of patients in whom argon laser energy was used to produce iridectomies.9,10,11 Difficulties in achieving patent iridectomies in eyes with dark brown irides or light blue irides were overcome by modifying treatment parameters and using a special contact lens developed by Abraham.
From these early reports beginning in 1973, laser iridectomy has been performed on hundreds of thousands of patients. The relative safety of the procedure and ease of performance combined with few complications accounted for its overwhelming acceptance by ophthalmologists. By the early 1980s, argon laser iridectomy had replaced the traditional surgical iridectomy as the procedure of choice for creating a hole in the iris.
It was in 1984 that the first reports of the successful performance of an iridectomy using the neodymium: yttrium-aluminum-garnet (Nd:YAG) laser were published.12,13 Moster et al.and associates in 1986 reported a controlled study comparing argon and Nd:YAG iridectomies.14 The mean number of applications to produce iris perforation was 6 with the Nd:YAG laser and 73 with the argon laser. Microhyphema was more prevalent in the Nd:YAG iridectomy group, but there was less inflammation.
In 1987, Tomey et al. and colleagues reported on 271 consecutive patients (373 eyes) in whom Nd:YAG laser iridectomy had been performed.15 They believed that the Nd:YAG laser offered the following advantages: lower energy level; lower incidence of spontaneous closure of the iridectomy; less inflammation; fewer required applications; absence of thermal injury to the cornea, lens, and retina; efficacy with opaque corneas; and effectiveness independent of iris color.
The Nd:YAG laser creates iridectomies by a different mechanical principal than the argon laser. The laser medium contains yttrium, aluminum, and garnet crystal with suspended neodymium atoms. It has a wavelength of 1,064 nm, which is invisible to the naked eye and is in the infrared range, but it is paired with a low-powered continuous-wave helium neon aiming beam that produces a red light, which is used for focusing. Most Nd:YAG lasers are of the fundamental q-switched type and work by producing photodisruption of tissue. The photodisruption process releases shock waves in the form of plasma that mechanically disrupts tissue. Iris color, though not important as a chromophore for the Nd:YAG laser as it is with the argon laser, does play a role. Very little YAG laser energy is required to perforate blue irides, while higher levels of energy must be employed for the thicker tissue of brown irides. Additionally, pigment liberation during Nd:YAG laser procedures on dark brown iridies can require cessation of the procedure and completion of the iridectomy at a subsequent office visit. Some Nd:YAG lasers are capable of producing thermal effects using continuous-wave or pulsed action.
During the late 1980s the q-switched Nd:YAG laser became the laser of initial choice for performing iridectomies. This is because of the relative ease of performance, the reduced rate of closure of the iridectomies, and less postoperative inflammation.
Indications
The indications for laser iridectomy have replaced most of the indications for a surgical iridectomy (Table 1). Currently, most residents do not get the opportunity to see or perform a surgical iridectomy, and this is a tribute to the development of laser technology and the improved techniques. A surgical iridectomy is done only if a laser iridectomy cannot be performed. This may occur in eyes with uncontrolled pressure and significant corneal edema that cannot be cleared by medical treatment. An eye with a flat anterior chamber or with corneal scarring that obscures iris details may also be unable to have a laser iridectomy performed.
TABLE 1. Indications for Laser Iridectomy | |
|---|---|
|
With the advent of the Nd:YAG laser and the development of the Abraham and Wise lenses, it is possible to achieve a patent iridectomy by using laser-directed energy in virtually 100% of patients.15
Angle-Closure Angle Closure Glaucoma Due to Pupillary Block
An iridectomy is indicated to relieve angle-closure glaucoma caused by a pupillary block mechanism. This occurs when pressure posterior to the iris is higher than the pressure anterior to the iris causing a peripheral convexity that blocks the trabecular meshwork. By equalizing the pressure between the posterior and anterior chambers, the anterior chamber is deepened and the angle opens, allowing aqueous to drain through the trabecular meshwork. Laser iridectomy is the procedure of choice in all forms of angle-closure glaucoma in which a pupillary block mechanism exists. In eyes with non-nonpupillary block angle closure, an iridectomy is not helpful or indicated. This can occur in eyes with uveitic glaucoma, neovascular glaucoma, the iridocorneal endothelial syndrome, or after surgery or trauma. A thorough slit-lamp microscopic exam with careful gonioscopy is needed to evaluate an eye in which pupillary block angle closureangle-closure glaucoma is suspected.
Pigmentary Glaucoma
A controversial indication for laser iridectomy is pigmentary glaucoma caused by a hypothesized reverse pupillary block, which results in concavity of the iris, causing chafing of the iris pigment epithelium by the lens zonule, subsequent dispersion of pigment, and raised intraocular pressure. This indication rests on the concept that pigmentary glaucoma is due not only to the posterior bowing of the iris, found in large myopic eyes, but also to a reverse pupillary block in which higher pressure is found anterior to the iris causing the iris to develop the peripheral concavity. This pressure differential could develop due to temporary ocular structural changes due to accommodation16 or blinking.17 In theory, iridectomy would equalize pressure between the anterior and posterior chambers, breaking this reverse pupillary block, relieving iris concavity and subsequent iris pigment dispersion.17 Ultrasound biomicroscopy has demonstrated flattening of iris concavity after iridectomy,18 and aqueous cell counts have shown a 65% reduction in aqueous melanin granules after iridectomy.19 A However, a retrospective study of 46 patients with bilateral pigmentary glaucoma who were followed for two 2 years after uniocular laser iridectomy did not clearly demonstrate reduced intraocular pressure.20 A large, prospective study is needed to address this issue.
Preoperative Preparation
The important aspects of preparation involve the maintenance of the clearest cornea possible, a constricted pupil, and control of inflammation and intraocular pressure (iopIOP). If an eye has experienced an acute glaucoma attack that is being treated medically but still is inflamed or has an edematous cornea that precludes safely performing an iridectomy, it may be prudent to control the inflammation, let the corneal edema clear, and perform the iridectomy later. The patient should be placed on a miotic during this interval plus instructed to frequently use topical steroids and any other glaucoma medications necessary to control iopIOP. During this treatment interval, the fellow eye should have a laser iridectomy performed to eliminate the possibility of it having an acute attack. However, if it is feasible, the iridectomy should be performed in the acute eye on the day of presentation, thus eliminating the possibility of a subsequent attack of angle closure. A thoroughly experienced surgeon may consider making a paracentesis to reduce the intraocular pressure, allowing a hazy cornea to clear sufficiently to perform the laser iridectomy.21
If the patient has noncongestive narrow-angle glaucoma and is on a miotic, the miotic should be instilled 1 hour before laser surgery. If the patient has not been on a miotic, pilocarpine 1% should be instilled 1 hour before laser surgery. In eyes with dark brown irides, pilocarpine 2% may be used. The miotic constricts the pupil and promotes penetration of the laser energy by placing the iris on stretch and making it thinner. It also reduces the contraction of the iris and pupil peaking, which sometimes is seen as the iris is treated with argon laser energy. A small pupil also reduces the possibility of laser energy inadvertently going through the pupil and striking the retina. Pretreatment with a topical alpha-agonist reduces the chance of a post-postlaser pressure spike.22,23 If intraocular pressure is elevated despite the miotic and the alpha agonist, then a beta blocker and a carbonic anhydrase inhibitor, if not contraindicated, should also be used before laser treatment. Prostaglandin drops are generally not used since both angle closureangle-closure glaucoma and laser treatment stimulate release of endogenous prostaglandins and because of their delayed onset of action.
Laser Contact Lens
The use of a lens with antireflective anti-reflective coating and a strong plus button greatly facilitates the ability to penetrate the iris and has improved the success rate in achieving iridectomies. It is so important to the success of the procedure that its use is considered mandatory. The Abraham lens consists of a modified Goldmann-type fundus lens with an 8-mm hole trephined into its periphery (Fig. 1) and a 66-D plano convex button bonded into the trephine hole. The Wise lens has a 103-D button. All front surfaces are covered with an antireflective coating. The convex lens enlarges the laser beam at the corneal surface, thus reducing the chances of epithelial corneal changes and decreasing the laser beam diameter at the iris surface, which increases the power density (Fig. 2). The power density at the cornea is one fourth as great with the Abraham lens but is increased to four times as great at the iris surface, which facilitates penetration. The lens also holds the lids apart and allows the surgeon to control eye movements. The gonioscopic solution improves the optics of the lens and reduces heat buildup, thus decreasing the incidence of corneal burns.
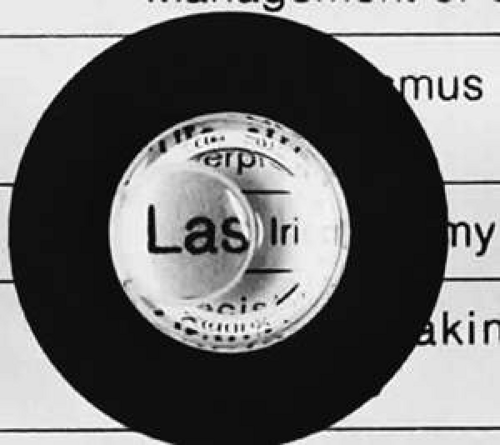 Fig. 1. Fundus lens Lens with a high plus button eccentrically placed. The Abraham lens has a +66-D D button, and the Wise lens has a + +103-D D button. |
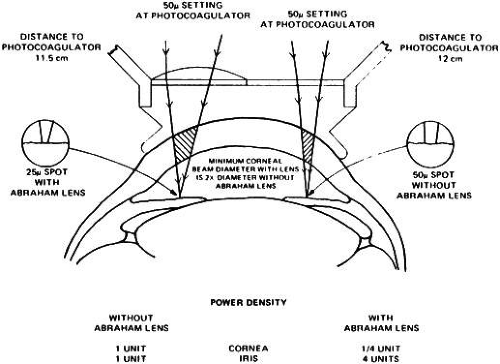 Fig. 2. Relative power density and spot size at the cornea and iris using an Abraham iridectomy lens. (Courtesy of R. Abraham.) |
The excellent optics of these lenses improves the visibility and magnifies the treatment site, thus reducing the depth of field and improving the precision of the laser focusing. All of these factors make these lenses an important adjunct to the successful production of iridectomies.
Surgical Technique
Both the surgeon and patient should be as comfortable as possible. A Velcro head strap helps to keep the patient well positioned with the forehead against the head bar. Patients tend to move backward, away from the slit lamp when the contact lens is placed on their cornea, and this makes precise focusing more difficult. An elbow rest is helpful to steady the surgeon’s arm and reduce fatigue. If present, the patient’s shirt collar button may be released and necktie loosened, and patients should be cautioned not to hold their breath. The laser room should be well ventilated to ensure patient comfort. A drop of topical anesthesia (e.g., proparacaine 0.5%) is used in all patients. Retrobulbar anesthesia is not necessary. The contact lens is placed on the eye with the trephined hole superiorly. The location of the iridectomy should be in the midperiphery of a constricted iris, about one third the distance from the limbus to the pupil, usually between the half past 10- and half past 1 1-o’clock positions (Fig. 3). An existing crypt or area of thin stroma will be easier to perforate. Vessels should be avoided to minimize bleeding. By placing the iridectomy under the upper lid, the possibility of a postoperative problem with glare or diplopia is reduced. The iridectomy should not be placed at the site of the resting lid margin since the prism created by the tear film meniscus at the lid margin can sometimes create glare or diplopia postoperatively. In the rare eye that has been filled with silicone oil, the iridectomy should be placed inferiorly to avoid blockage by the oil. Regardless of the site chosen, it is important to aim the laser beam away from the macula. The aiming beam should be perpendicular to the contact lens surface and through the center of the lens button.
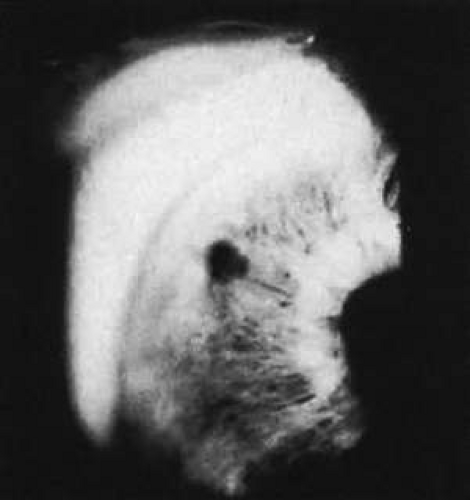 Fig. 3. Superonasal location of iridectomy site at the half past 10 10-o’clock position in the left eye, about one third the distance from the limbus to the pupil. |
In pupillary block angle closure, the signal that the laser beam has perforated the pigment epithelium is a stream of pigment clumps carried by the posterior chamber aqueous humor into the anterior chamber in a mushroom-cloud configuration. The end point of treatment is the direct visualization of the anterior lens capsule with the slit lamp. Transillumination is not a good technique to determine the patency of an iridectomy. There can be extensive transillumination, especially in blue eyes, whereas the iris stroma still may be intact with no through-and-through iridectomy (Fig. 4). After the iridectomy, the central anterior chamber depth usually is not affected; however, deepening of the peripheral anterior chamber is a reliable sign that the iridectomy has achieved its functional purpose.
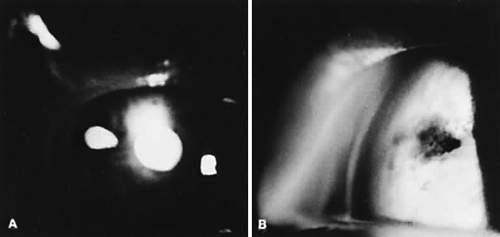 Fig. 4. A:. Extensive transillumination defect in blue iris nasally. B:. Iris of same patient with iridectomy much smaller than the transillumination defect because of intact iris stroma. |
In most cases, the Nd:YAG laser is the laser of initial choice for iridectomy. In some settings the argon laser may be the only available device. If good progress is not being made with the argon laser, it is prudent to switch to a Nd:YAG laser.
Nd:YAG Laser Iridectomy
Recommended settings for the Nd:YAG laser range from 3 to 7 mJ per burst and from one to three pulses per burst. It is safest to begin with a single pulse of approximately 4 to 6 mJ. The importance of precise focusing on the anterior stroma cannot be overemphasized. This produces maximum photodisruption and minimizes the possibility of lens injury.
Thick brown irides are more difficult to penetrate. Sometimes, the iris stroma shreds without a through-and-through opening achieved. It can be helpful to make a crypt with the argon laser and then punch through with the Nd:YAG laser. In a few cases, the reverse procedure is followed: the Nd:YAG laser is initially used, and the iridectomy opening can be completed with argon laser energy. In thick brown irides, using two to three pulses per burst often is helpful. The iridectomy typically is a slit (Fig. 5).
 Fig. 5. The Nd:YAG laser iridectomy typically appears slitlike. |
In patients who are on anticoagulant therapy or have bleeding disorders, it is advisable to use argon laser energy. Bleeding from the iridectomy site is rare with the argon laser because the tissue destruction involves thermal coagulation. Bleeding at the iridectomy site is common with the use of Nd:YAG laser energy because the photodisruption process (Fig. 6) does not coagulate the iris vessels. If bleeding does occur it usually stops spontaneously and can be minimized by applying gentle pressure with the contact lens to temporarily raise the intraocular pressure. Moster et al.and colleagues reported bleeding from the iridectomy site in 34% of eyes after Nd:YAG iridectomy but in no eyes after argon laser iridectomy.14
 Fig. 6. Bleeding from a a patent Nd:YAG iridectomy site. (From Pollack IP, Robin AL, Dragon DM et al: Use of the neodymium:YAG laser to create iridotomies in monkeys and humans. Trans Am Ophthalmol Soc 82:307, 1984, with permission.) |
Argon Laser Iridectomy
Table 2 outlines the recommended treatment parameters for argon laser iridectomy. A variety of techniques have been described to facilitate the creation of an argon iridectomy. Some of these include placing stretch burns in a circle (drumhead technique) and then placing penetrating burns in the center of the circle. Abraham and Miller recommend using stretch burns to cause a hump in the iris and then using penetrating burns to punch through the hump.10 The stretch burns contract the iris, but they are not used for penetration. Stretch burns usually are placed with a 200-μm spot size and a 0.2-second duration, using 200 to 400 mW of power.
TABLE 2. Treatment Parameters for Argon Laser Iridectomy | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
A well-accepted standard technique using the argon laser is to begin initial treatment with a 50-μm spot size and a 0.2-second duration, with about 850 mW of power. The aiming beam must be precisely focused on the surface of the iris to superimpose the burns. These two factors—precise focusing and superimposition—are the keys to success. Often, iris perforation can be achieved within 10 applications, and for any iridectomy, the tissue reaction to the initial burns often is an indicator as to the ease of the procedure. If bubble formation is seen at the site of the burn, this indicates stromal vaporization. The clinician then should focus at the base of the bubble, continuing to deliver energy until the stroma has been perforated. This is helpful in the light blue iris.
The easiest irides to perforate with the argon laser are hazel and light brown. The most difficult are light blue irides with minimal pigment and thick, dark brown irides. If good progress is not made at the initial treatment site, the clinician can move to another site. However, if charring is seen, which has the appearance of a black piece of coal, then switching to a chipping technique has been found to be helpful in dark brown irides. The duration is reduced to 0.02 seconds and the power increased to 1 to 1.5 W. This short-duration burn avoids charring at the base and reduces the chance of endothelial burns. However, it may take 100 to 300 applications to complete the iridectomy using these short-duration burns.
Light blue irides require a different technique. Blue eyes have little melanin pigment in the stroma, and a longer duration burn provides an increased thermal effect, which is necessary to get through both stroma and pigment epithelium in these lightly pigmented irides. A power setting of 800 to 1,000 mW and duration of 0.2 to 0.5 seconds is used with a 50-μm spot size. The clinician looks for an iris freckle or an iris crypt that would make penetration easier. The patient’s eye usually will not stay still for the full 0.5 seconds, so it is necessary to be able to quickly cut off the laser energy before 0.5 seconds if eye movement is seen. A vaporization bubble sometimes is seen at these settings, and by aiming at the base of the bubble, it is often feasible to achieve perforation in two or three shots of 0.5 seconds’ duration each. Most of the argon laser treatment is directed toward enlarging the iridectomy and cleaning the pigment out from its edges. The edges of the initial perforation site are treated with laser energy to enlarge the actual opening and reduce the chance of subsequent closure from pigment proliferation. Care must be used because laser energy will be going through the iridectomy, possibly hitting the lens and retina.
Postoperative Management
The major postoperative treatment involves monitoring and controlling IOP and the expected mild postoperative inflammation. Moster et al.and colleagues report that 76% of patients had a maximal elevation of IOP in the first hour, whereas 16% peak at the second hour, and 8% reached maximal elevation during the third hour.14 Thirty-one percent of the Nd:YAG laser-treated eyes and 34% of the argon laser-treated eyes had an IOP rise greater than 8 mm Hg above baseline. Therefore, we routinely pretreat all eyes with apraclonidine or brimonidine and monitor IOP after a laser iridectomy procedure. If there is a pressure spike, the patient is treated and seen the next day; otherwise, the patient is seen between 5 and 7 days later, at which time the second eye can undergo laser treatment if necessary.
Methods to reduce the incidence and magnitude of a postlaser iridectomy pressure spike include pretreatment with apraclonidine or brimonidine and miotics if they have not been used in the last 2 hours, instilling a beta blocker or carbonic anhydrase inhibitor if not contraindicated, and considering the use of an oral osmotic or carbonic anhydrase inhibitor if there is significant cupping and field loss. Robin et al.and associates demonstrated that topical para-aminoclonidine (apraclonidine hydrochloride; Iopidine, Alcon) was effective in reducing significant pressure spikes after argon laser iridectomy.22 Forty-three percent of eyes treated with placebo and no eyes treated with apraclonidine had an IOP rise more than 10 mm Hg above baseline. Brimonidine has been shown to have efficacy equal to that of apraclonidine.23 By reducing the incidence and magnitude of the pressure spike, there is less chance for further glaucomatous damage. No significant differences in postoperative IOP spikes have been found between the argon and Nd:YAG lasers. In the authors’ combined experience of several thousand laser iridectomies, we are aware of only a small number of eyes requiring incisional surgical intervention (e.g., paracentesis or filtration surgery) to control a pressure spike after laser iridectomy.
The IOP elevation may be related to the release of pigment and inflammatory debris clogging the trabecular meshwork. In eyes with poorly controlled IOP or eyes that have severely compromised outflow facilities, IOP elevations are more likely to be seen. By monitoring the IOP postoperatively if there is a significant elevation, treatment with pressure-lowering agents can be carried out. Tonographic studies done in monkeys at varying intervals after laser iridectomy have not shown decreases in outflow facility, which indicates the pigment liberated does not permanently clog the trabecular meshwork.24 Topical steroids are used to control iritis, which is seen in all patients. The usual treatment schedule is one drop of prednisolone acetate four times a day, and this usually can be discontinued by 4– to 7 days postoperatively. Miotics are continued at least temporarily if the patient has been on them preoperatively. Miotics also are used if there is a question about the patency of the iridectomy.
Postoperative gonioscopy should be done to assess the effect of the iridectomy on the angle configuration and to determine the extent of permanent synechiae, if present. If there is a patent iridectomy, the pupil is dilated on an early postoperative visit to prevent the formation of posterior synechiae and to visualize the posterior pole and peripheral retina, which might not have been possible before. Also, one may check the intraocular pressure after dilation as a mydriatic provocative test, to rule out the possibility of a plateau-iris configuration. If the argon laser has been used, the patient is observed over the next 6 weeks to watch for pigment proliferation leading to closure of the iridectomy. If closure occurs, the iris is retreated to open the iridectomy and enlarge it.
Complications
Corneal Changes
Corneal changes include epithelial and endothelial burns. They usually are transient but can impair the ability to complete an iridectomy because the laser energy cannot be delivered accurately and effectively. It helps to reposition re-position the eye and aim through a noninvolved portion of the cornea. It may be necessary to go to another location if visibility is not adequate. Endothelial burns are caused by the thermal effects of argon laser treating the iris, especially in eyes with shallow chambers. They usually resolve within a few weeks but can cause focal endothelial cell loss. Investigators have not been able to demonstrate statistically significant endothelial cell loss during follow-up periods of 1 year after argon laser iridectomy.25,26 Schwartz and coworkers et al. reported on five eyes of three patients who developed corneal decompensation after undergoing argon laser iridectomy for angle-closure glaucoma.27 They found that a history of pre-existing corneal guttata, episodes of angle-closure glaucoma with elevated IOP and inflammation, and the need for repeat treatments all seemed to predispose to this rare complication.
Nd:YAG iridectomies can cause focal endothelial cell loss if the disruption takes place less than 1 mm from the corneal endothelium,28 and decreased endothelial cell counts at 1 year follow–up have been documented.29. As with argon laser iridectomy, corneal edema has not, however, been shown to be a clinically significant problem after Nd:YAG iridectomy.
Lens Opacities
Focal anterior subcapsular lens opacities at the iridectomy site frequently are seen with argon laser iridectomy and also can be found after Nd:YAG iridectomy (Fig. 7). A small, one 1-year observational series of Asian patients treated with prophylactic argon and Nd:YAG laser iridectomies reported cataract progression.30 Two-year follow-up in a larger series showed visual acuity the same or improved in 85% of eyes undergoing therapeutic argon laser iridectomy.31 Breaks in the anterior lens capsule in eyes undergoing Nd:YAG iridectomy have been demonstrated histopathologically in patients subsequently undergoing intracapsular cataract extraction.32 No differences in cataract formation were demonstrated in rabbit eyes when comparing argon and Nd:YAG laser iridectomies.33 In monkeys, treatment parameters of one or two bursts and less than 6 mJ reduce the incidence of lens opacities with the Nd:YAG laser, and if a capsule break should occur, fibrous proliferation seals it.34
The widespread concern that laser iridectomy may cause rapid development of visually significant cataracts because of inadvertent rupture of the anterior lens capsule fortunately has not been shown. To minimize lens damage it is helpful to focus on the anterior iris stroma and to perform the iridectomy peripherally, where the patient’s convex lens is further away from the pigmented epithelium of the iris.
Closure of the Iridectomy
Closure of a patent laser iridectomy almost never occurs with Nd:YAG procedures. With argon procedures, closure may be either immediate or delayed. It is important to recheck the iridectomy site at the same time that the patient’s IOP is monitored postoperatively because the iridectomy site may be occluded by the landsliding of pigment epithelium into it from its edges. The opening can be enlarged, if necessary, with a few more applications of laser energy. If late closure occurs, it usually occurs by 6 weeks and is a result of pigment proliferation. Performing a large, clean initial iridectomy reduces the likelihood of an iridectomy closing and the need for retreatment. Blue irides treated with the argon laser had a 35% incidence of retreatment in our series of over 200 eyes treated between 1977 and 1982, whereas brown irides had only a 15% retreatment rate. The blue eyes had the greater need for retreatment because of the difficulty of obtaining a large iridectomy and tendency for pigment proliferation to fill in the iridectomy (Fig. 8).
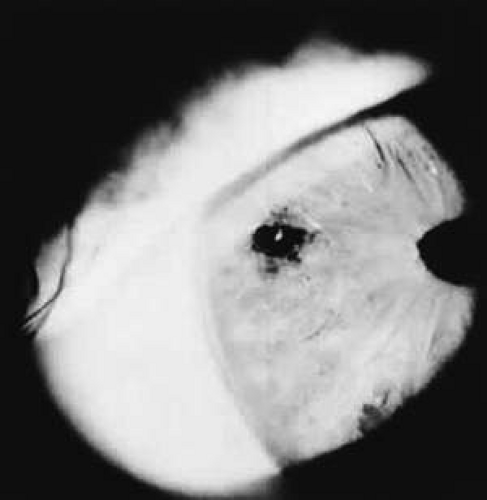 Fig. 7. Focal anterior lens capsule opacity visible through iridectomy opening. |
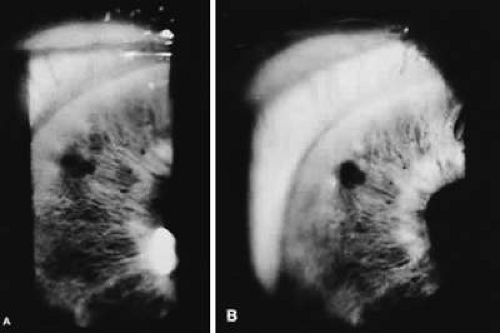 Fig. 8. A:. Iridectomy site has been closed by pigment proliferation. B:. Iridectomy reopened after a second laser treatment. |
Diplopia and Glare
Occasionally, patients may complain of an extra image or a light reflex from the iridectomy site. By placing the iridectomy under the upper lid, these complications are significantly reduced. However, some iridectomies have been placed inferiorly or at the three or nine3- or 9- o’clock position with no problems. If the iridectomy is located at the border of the lid margin, these symptoms seem more likely to occur, possibly due to the prismatic effect of the tear meniscus formed at the lid margin. Over time, this problem will become less bothersome to most patients.
ADVANTAGES OF LASER VERSUS SURGERY
It is no longer necessary to compare the advantages of laser iridectomy with surgical iridectomy. Laser iridectomy has revolutionized the management of angle-closure glaucoma. It has unburdened both the patient and the ophthalmologist. In the past, one of the hardest tasks was to convince a patient who had just experienced an acute congestive attack of angle-closure glaucoma to undergo an intraocular surgical procedure in a nonsymptomatic “healthy eye” while the acute eye was quieting down. Another difficult scenario was that of the patient with creeping angle-closure glaucoma who was totally asymptomatic and needed bilateral surgical iridectomies. The ease of laser iridectomy, in contrast to incisional surgical iridectomy, has made both patients and doctors more willing to proceed with the desired treatment course.
In patients with uncontrolled combined-mechanism glaucoma, a laser iridectomy can be performed to determine if it alone will control the IOP without having to subject the patient to two incisional procedures if filtering surgery was (Ed: Should this be were or was?)to be eventually necessary. Since laser iridectomies are relatively safe and simple to perform, it is a concern that the indications can be easily abused, and that patients who do not need an iridectomy will be offered it. This may be a result of an inaccurate gonioscopic examination, a subjective examination, or one not uniformly mastered. Laser iridectomy also may be unnecessarily performed if the mechanism of primary angle closure is not truly understood. It then might be performed in eyes with peripheral anterior synechiae that are secondary to uveitis, rubeosis, or iridocorneal endothelial syndrome, i.e., disorders caused by a nonpupillary block angle-closure mechanism.
DISADVANTAGES OF LASER VERSUS SURGERY
Compared with surgical iridectomy, there are no disadvantages to laser iridectomy. However, it may not be possible to perform a laser iridectomy if there is significant corneal edema or a flat chamber. If patency cannot be achieved, a surgical iridectomy then must be performed. With argon laser energy there is a remote risk of a macular burn, and with both types of laser treatment there is the risk of a postoperative IOP spike and possible visual field loss involving fixation. Laser surgery requires the use of costly equipment that must be well maintained, and this expense may become more of a problem unless the cost of laser instruments decreases to match changes in reimbursement, an unlikely event.
LASER TRABECULOPLASTY
Since the early 1980’s, argon laser trabeculoplasty (ALT) has been the primary initial surgical treatment for uncontrolled open-angle glaucoma unresponsive to medical therapy. It has experienced a worldwide acceptance and has revolutionized the management of the glaucoma patient. The indications for ALT have been continually refined, as have the modifications in the surgical technique, to reduce complications. Much has been learned about long-term results, the role of retreatment, and ALT’s role as initial therapy for patients with newly diagnosed open-angle glaucoma.
History
Krasnov first reported laser treatment of the trabecular meshwork in 1973.35 He used a high-powered ruby laser to make microscopic punctures through the trabecular meshwork and into the Schlemm’s’s canal. The openings functioned for only a few months, and retreatment was required to maintain the effect, but initial excellent IOP lowering was reported. Worthen and Wickham were the first to report on treating part of the angle (90°) with argon laser energy.36 They reported a mean IOP reduction of 9.6 mm Hg in 20 patients with limited follow-up. They subsequently reported long-term follow-up with 50% of the treated eyes having an IOP of less than 25 mm Hg after 4 years of follow-up.37 They were appropriately cautious in their recommendations, partially because of the report by Gaasterland and Kupfer in 1974 on the experimental production of glaucoma in monkeys by heavy repeat treatment of the angle with argon laser energy.38 This report raised the possibility that laser therapy could aggravate rather than help glaucoma in some situations, and thus dampened the enthusiasm for this treatment modality. In 1979, Wise and Witter reported a greater than 90% success rate in argon laser-treated phakic eyes in open-angle glaucoma.39 Their technique differed from the report of Worthen and Wickham in that they treated all 360° of the angle. Schwartz and coworkers et al. reported on 35 phakic eyes with clinically uncontrolled open-angle glaucoma that underwent 360° treatment. The IOP of the untreated eye was used as a control. The mean pressure change in the treated eye at 4 months was 10 mm Hg, and this was maintained throughout the initial 18-month follow-up period.40 At the 1980 American Academy of Ophthalmology meeting, this report40 and others by Wise41 and Wilensky and Jampol,42 demonstrated the efficacy of 360° argon laser treatment to the trabecular meshwork.
Indications
Before the advent of ALT, the side effects of medical therapies had to be endured because the major alternative was filtering surgery with its known complications. Initially, laser trabeculoplasty was reserved for end-stage glaucomatous eyes, patients who refused filtering surgery, previous surgical failures, or patients who were poor surgical risks. The experience that has been gained has radically altered the indications. Patients with open-angle glaucoma including exfoliation syndrome and pigmentary glaucoma are being offered ALT earlier and earlier in the therapeutic sequence. Fewer patients are being subjected to the side effects of miotics and carbonic anhydrase inhibitors.
ALT is not recommended for patients with juvenile glaucoma or glaucoma secondary to uveitis or angle recession. It is unlikely to provide young patients with a lifetime cure, and a filtering procedure or tube shunt is a more appropriate initial surgical choice for these patients. Also, if patients have an IOP that is above 35 mm Hg and requires a low target pressure, filtering surgery usually is recommended, since ALT is unlikely to lower IOP enough to reach the target pressure.
ALT is usually not offered to patients who have elevated IOP without any signs of damage to the optic disc or visual field, or to patients who have IOP well controlled with tolerated medical therapy. Whereas less than 1% of patients are made worse by ALT with a resulting IOP higher than at baseline, one may hesitate to subject a patient with a normal optic disc and visual field to the risks of filtering surgery because of an untoward effect from premature ALT.
The Glaucoma Laser Trial (GLT)43,44,45,46,47 was a multicentered randomized clinical trial involving 271 patients that was designed to assess the safety and efficacy of ALT as initial treatment for newly diagnosed open-angle glaucoma patients compared with treatment using topical medications. Each patient had one eye randomly assigned to initial treatment with ALT and the other eye assigned to therapy with timolol maleate 0.5%. At 2 years, the laser-treated eyes had a lower mean IOP than the medication treated eyes, and fewer laser-treated eyes required two or more medications to control IOP (p < 0.001). Forty-four percent of the laser-treated eyes were controlled by ALT alone. With the same follow-up period, 30% of the medication-treated eyes were controlled by timolol, and only 66% were controlled within the stepped medication regimen, whereas 89% of the eyes treated with ALT plus medications were controlled. Medication was initiated or changed for either eye according to the same step regimen if the IOP was not controlled.
The long-term results of the GLT and the GLT follow-up study47 showed that at 7 years, eyes initially treated with ALT had lower eye pressures and less visual field and optic nerve damage than eyes initially treated with topical medications. The conclusion of the study was that “initial treatment with argon laser trabeculoplasty was at least as efficacious as initial treatment with topical medications.”47
Preoperative Preparation
Patients are instructed to continue all glaucoma medications on their regular schedule. Patients are routinely pretreated with an alpha-2 agonist, i.e., brimonidine or apraclonidine, to prevent a significant IOP spike that could adversely affect visual function.23,48 Alpha-2 agonists work by decreasing aqueous production. The effect is additive to beta blockers. The eye should not be exposed to diagnostic procedures before the treatment because this can affect corneal clarity.
Surgical Technique
Laser trabeculoplasty is performed as an outpatient procedure using topical anesthesia. The gonioscopic mirror of an antireflection-coated, three-mirror lens with a flange to retract the lids is used routinely. Other lens choices include the Ritch trabeculoplasty. It is a rare patient whose small palpebral aperture requires a single-mirror goniolens. Before starting treatment, it is critical to identify the angle landmarks: the Schwalbe’s’s line, the trabecular meshwork, and the scleral spur. The treatment may begin with the gonioscopic mirror at the 12 12-o’clock position viewing the inferior angle. The inferior angle tends to be the most open part and has the most pigmentation, making angle structures more clearly defined in this area. This facilitates identification of the angle landmarks and avoids treating the wrong part of the angle. Some patients have a high iris roll and a prominent Sampaolesi’sSampaolesi’s line, and it is easy to mistake the Sampaolesi’sSampaolesi’s line for the pigmented trabecular meshwork and treat the wrong part of the angle.
Occasionally, the initial plan may be to perform a trabeculoplasty, but after more careful study of the angle, areas of peripheral anterior synechiae may be recognized or the approach may be so narrow that it may be concluded that treatment of the trabecular meshwork would be difficult. In these eyes, a laser iridectomy is performed initially to treat the narrow angle component or to facilitate future trabeculoplasty. It is usually preferred to assess the effect of the iridectomy on IOP and angle configuration before later proceeding with trabeculoplasty, but some glaucomatologists prefer to perform both at the same time. If only a small area of the angle is obscured because of a high iris roll, an argon laser gonioplasty (see discussion below) can be performed.49 If more than 10 ten laser goniplasty applications are required to open the angle, it is preferable to perform an iridectomy and reschedule the trabeculoplasty. It is not recommended to perform trabeculoplasty immediately after the laser iridectomy because of increased postoperative inflammation, corneal clarity changes, and possible greater problems with postlaser IOP elevations.
The use of a fixation light for the contralateral eye assists the patient in maintaining the appropriate eye position. Before the initiation of treatment, the eyepieces are focused and the argon laser is set to the standard treatment parameters: a spot size of 50 μm, a duration of 0.1 seconds, and an average power of 800 mW (range 600 to 950 mW). It is critical to check these parameters because lasers in a hospital or clinic setting are used by multiple ophthalmologists for a variety of intraocular procedures. During the treatment, the power setting required to blanch the trabecular meshwork or cause a small bubble formation is empirically determined. It is helpful to use a standardized treatment technique, for example, starting with the mirror at the 12 12-o’clock position and rotating it in a clockwise manner. Initial treatment of 180° of the angle always would be the temporal 180° in the right eye; the nasal 180° in the left eye. A continuous-wave argon laser blue– green light is routinely used (Fig. 9).
 Fig. 9. A continuous wave continuous-wave of argon laser energy is delivered to the trabecular meshwork. (Courtesy of I. Pollack.) |
Argon laser burns are placed at the anterior border of the pigmented trabecular meshwork (Fig. 10). Thomas et al.and colleagues have shown that the more posterior the treatment, the greater the incidence of IOP elevation and formation of posterior synechiae.50 A power setting that produces blanching or depigmentation at the point of impact with a slight vaporization bubble is optimal (Fig. 11). Some investigators do not think it is necessary to gauge the tissue reaction and use a standardized treatment parameter of 800 mW in nearly all patients. We usually treat 180° at the initial setting, although 360° can be treated if clinically indicated. The spacing of the laser burns is the same whether 180° or 360° are treated, that is, 20 to 25 burns per 90° of angle treated, regardless of the area treated (Fig. 12). Previously, the laser beam was aimed at the center of the pigmented trabecular meshwork, but now it is aimed at the anterior border of the pigmented trabecular meshwork. Histologically, this corresponds to the junction between the anterior nonpigmented and posterior pigmented trabecular meshwork. This location is preferred because posterior laser treatment caused a higher incidence of IOP elevation in the immediate postoperative period. Traverso et al. and coworkers report the development of peripheral anterior synechiae in 43% of eyes that were treated posteriorly but only in 12% of eyes treated anteriorly.51 Posteriorly placed burns also are more likely to cause patient discomfort. The procedure usually is well tolerated by patients as long as the iris and scleral spur are not struck with the laser beam energy.
 Fig. 10. Optimal treatment location is at the anterior border of the pigmented trabecular meshwork.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|