26
Laryngeal Leukoplakia and Neoplasm
Vocal communication is an important element of human interaction. Voice is produced by the coordination of expiration and vocal fold closure. At the vocal folds, the gelatinous superficial lamina propria allows the overlying mucous membrane to vibrate fluidly while expired air flows over it, producing periodic acoustic energy, with the pharynx acting as a resonance chamber. We recognize this acoustic energy as the human voice. Lesions that begin on the mucous membrane of the vocal fold adversely affect vibration because the periodicity of the acoustic energy is disturbed.
Vocal cord vibration generates rhythmic waves of pressure in the air through the interaction of the vocal fold “cover” and the airstream. The “body-cover” theory of vocal fold vibration states that the underlying tissues, the deep connective tissue layer of the lamina propria, the vocal ligament, and the vocalis muscle, are relatively static, whereas the superficial lamina propria and the mucosa open and close to allow air to pass between the opposed mucosal surfaces. The mucosa moves in an oscillating fashion such that motion of one cord is the mirror image of the other. The mucosal wave originates at the inferomedial aspect of the vocal cord epidermis and propagates rostrally with expiratory airflow. As the rostral cord surfaces separate during the mucosal wave motion, exhaled air passes between the vocal folds. The negative pressure generated as air passes between the cords, as described by the Bernoulli effect, causes the inferior aspect of the vocal folds to pull together, followed by closure of the rostral aspect of the cords. Flow ceases until the build up of subglottic pressure overcomes the resistance of the closed vocal folds, and the cycle begins again.
Efficient vocal fold closure and the unique viscoelastic properties of the mucosal surfaces and superficial lamina propria are necessary for the formation of the mucosal wave. Lesions of the vocal folds may prevent symmetrical closure of the vocal folds or alter the viscoelastic properties of the tissues and interrupt the mucosal wave function. The result is a voice that is hoarse with a decrease in the vocal range. In this chapter, we analyze the histopathology of premalignant and early-stage malignant tumors of the vocal cords and the resultant abnormalities of vocal fold vibration as imaged with videostroboscopy.
 Histopathology
Histopathology
Laryngeal leukoplakia is defined as a white patch on the vocal cord and has been reported to have a malignant transformation potential of 1 to 40% (Fig. 26.1).1 Leukoplakia is the result of cellular changes in the overlying vocal fold epithelium and must be differentiated from candida infection of the vocal fold (Fig. 26.2). Leukoplakia may appear as a uniformly smooth superficial lesion affecting a portion of one or both vocal folds or as a thick, rough area of the vocal fold (Fig. 26.3). Some of these lesions extend across the anterior commissure (Fig. 26.4). Others involve a patch-like distribution across the vocal fold (Fig. 26.5). Rarely, leukoplakia may affect the supraglottic structures, the arytenoid body, and the interarytenoid region (Fig. 26.6). Some leukoplakia is associated with erythema, and the term erythroleukoplakia is used (Fig. 26.7). Erythroleukoplakia is the most likely of these lesions to be malignant.2,3
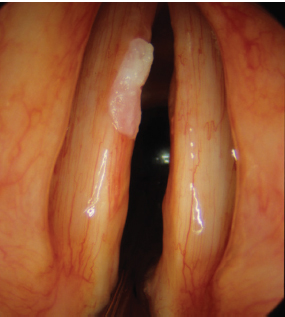
Fig. 26.1 A focal area of leukoplakia involving one vocal fold with variable thickness.
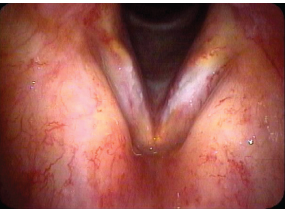
Fig. 26.2 Leukoplakia must be differentiated from candida infection of the vocal fold. This patient had received radiation therapy for laryngeal carcinoma 3 years previously. Although the exam is worrisome for recurrent carcinoma, these lesions resolved with antifungal therapy.
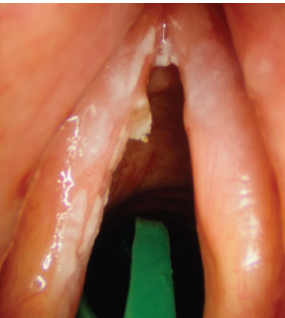
Fig. 26.3 Leukoplakia may appear as a patchy lesion with variable thickness as well as patchy white debris that is easily dislodged from the surface of the vocal fold as noted in the anterior commissure of this image.
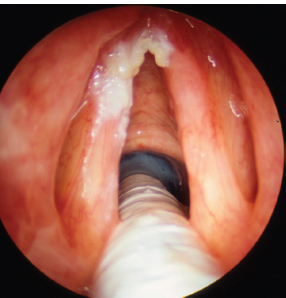
Fig. 26.4 Leukoplakia can extend across the anterior commissure.
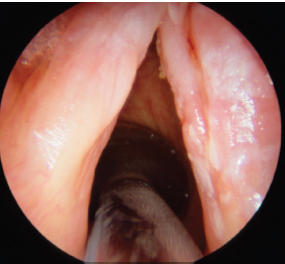
Fig. 26.5 The patchy nature of some leukoplakia lesions of the larynx can involve the true vocal fold as well as the ventricular fold.
Leukoplakia on the vocal cord represents a broad spectrum of pathology, with an array of corresponding malignant potential. Leukoplakia, without surrounding erythema, may represent a benign transformation called hyperkeratosis or parakeratosis. These lesions are confined to the vocal cord mucosa and have a thickened but ordered cellular maturation from the basal layer to the surface and thus do not demonstrate any degree of dysplasia. On the other hand, a grossly similar leukoplakia of the vocal fold may demonstrate increasing disorder of the cellular maturation process from the basal layer to the surface and represent mild, moderate, or severe dysplasia, depending on the degree of abnormality. The risk of malignant transformation increases as the severity of dysplasia increases.4 Lesions that are diagnosed as mild dysplasia are expected to transform in 2 to 12% of cases, and moderate dysplasia transforms in 7 to 27% of cases. Carcinoma in situ is diagnosed when the dysplastic changes are severe, yet the lesion does not penetrate the basement membrane. Invasive carcinoma occurs when the abnormal epithelial cells invade the tissues below the basement membrane (Figs. 26.8 and 26.9).
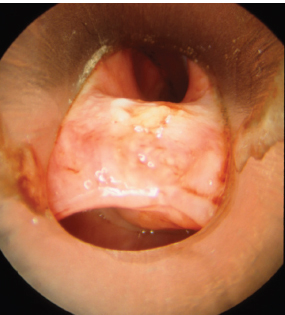
Fig. 26.6 A rare case of leukoplakia of the interary-tenoid region. The vocal folds are in the upper portion of the image hidden by the laryngoscope.

Fig. 26.7 This image reveals patchy erythroleukoplakia.
 Videostroboscopic Evaluation of Leukoplakia
Videostroboscopic Evaluation of Leukoplakia
The evaluation of patients with leukoplakia using videostroboscopy yields valuable information. The technique allows for the video-documentation of the geographic distribution of leukoplakia over time. In many patients, the distribution of leukoplakia remains stable over time, and when the distribution of leukoplakia increases along the length of the vocal fold, malignant transformation should be considered. The use of videostroboscopy to evaluate and follow patients with leukoplakia is highly valuable. In patients with thin, superficial leukoplakia, the vocal fold vibration pattern may remain completely intact with a normal vibratory phase, amplitude, periodicity, and glottic closure. In this group of patients, malignancy is highly unlikely. In patients with isolated thick leukoplakia, the affected vocal fold may vibrate with normal vibration amplitude, periodicity, and phase; however, the glottic closure may be affected by the thick lesion. In addition, the area of thick leukoplakia will often demonstrate an adynamic segment within the vocal fold mucosa. Some of these isolated lesions may represent a benign lesion, whereas others may be malignant. Thus, these lesions may warrant surgical excision with a close resection margin and maximal preservation of the underlying superficial layer of the lamina propria.
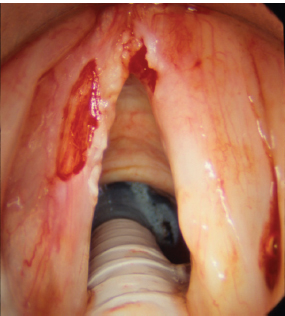
Fig. 26.8 An incisional biopsy of the lateral aspect of the left vocal fold was performed for an umbilicated lesion of the lateral aspect of the vocal fold after microinfusion. This biopsy revealed squamous cell carcinoma.
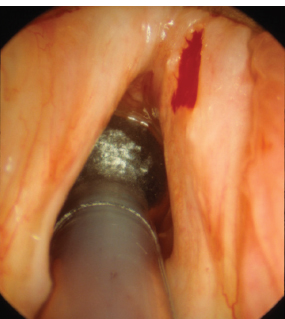
Fig. 26.9 This patient has been treated for isolated leukoplakia involving the free edge of the vocal fold with an excision of the lesion and preservation of the superficial layer of the lamina propria, in hopes of preserving vocal function. The pathologic examination revealed carcinoma in situ.
In patients with bilateral leukoplakia and diffuse leukoplakia, the vibratory nature of the vocal fold is severely disturbed, and the periodic nature of vocal fold vibration is so abnormal that vocal fold vibration is absent as seen on videostroboscopy. The aperiodic nature of the fundamental frequency prevents the filter board within the videostroboscopic unit from providing light output that is asynchronous to the vocal fold vibration. Without adequate tracking of the sound source signal, videostroboscopy has minimal use. In these situations, the vibratory characteristics listed above cannot be evaluated. High-speed imaging may provide a significant improvement in the evaluation of these diffuse lesions and their effect on vocal fold vibration. In addition, patients with diffuse leukoplakia use significant supraglottic compression during voice production. The supraglottic compression is often so severe that visualization of the vibratory surfaces of the vocal fold during voice production is exceedingly limited. Similarly, in patients with inflammatory illness of the vocal fold, the vibration pattern is seen as restricted in amplitude along the full length of the vocal fold. This finding is seen in patients with unilateral erythroplakia.
When comparing hyperkeratosis, parakeratosis, and various degrees of dysplasia, videostroboscopy may not yield significant differences. These are all benign lesions that involve the vocal fold epithelium and do not extend into the superficial lamina propria. In theory, it may be possible to determine if there is deeper invasion by a vocal fold lesion when observing the degree to which the lesion alters vocal fold vibratory characteristics. From what is known about the biomechanics of vocal fold vibration, it is assumed that lesions that appear to vibrate on top of the superficial layer of the lamina propria, along with normal vibration of the surrounding tissues, imply minimal alteration of the vocal fold microstructure and are more likely to be benign. Similarly, lesions that involve the superficial layer of the lamina propria (invasive carcinoma) would be expected to reveal a greater degree of stroboscopic abnormality. In very superficially invasive lesions, the vibration abnormality is expected to be limited to the lesion itself. As the degree of invasion progresses, videostroboscopy might demonstrate a generalized loss of vocal cord vibration at the site of leukoplakia that extends to the surrounding vocal fold mucosa (Video Clip 35). Unfortunately, the expected changes in vibration with increasing degrees of tissue invasion are not clinically reliable. In a blinded study of premalignant and early-stage malignant changes of the vocal folds, Colden et al. demonstrated that the vibratory characteristics of the two groups of lesions are not consistently distinguishable by expert raters.5
As squamous cell carcinoma lesions advance in stage, vocal cord fixation or impaired movement of the vocal fold can be seen. Videostroboscopy shows changes not only of the vocal fold mucosa but also changes due to incomplete glottic closure associated with vocal paresis or paralysis. The loss of glottic closure is often associated with a contralateral ventricular fold hyperfunction as a compensation strategy.6 This can limit the overall view of the mucosal wave during stroboscopic analysis. When the mucosal wave can be viewed in these patients, severe aperiodicity is common due to the restriction in the pliability of the vocal fold mucosa.
 Further Work-Up for Definitive Diagnosis
Further Work-Up for Definitive Diagnosis
As the degree of dysplasia is thought to be the most reliable predictive factor for malignant transformation in laryngeal leukoplakia, a pathology evaluation must always be performed. A deep vocal fold biopsy provides a clear picture of the depth of the lesion but can result in scarring of the vocal fold mucosa and superficial lamina propria leading to vibration abnormalities at the biopsy site with devastating phonation results. Biopsies, therefore, should be performed using microlaryngeal techniques that maximally preserve normal structures.
The possibility of using a brush biopsy rather than a tissue biopsy to determine the risk of malignant transformation in leukoplakia has been studied. Woo quotes an 87% positive predictive value for brush biopsies using excisional or punch biopsy as a standard.7 The ease of performing brush biopsy as an office procedure is more attractive to the patient and potentially allows the physician to closely monitor the progression of these lesions. The principal advantage of the brush biopsy is that this technique does not present any risk of injury to healthy tissues, thus functional changes due to biopsy are rare.
References
1. Bouquot JE, Gnepp DR. Laryngeal precancer: a review of the literature, commentary, and comparison with oral leukoplakia. Head Neck 1991;13:488–497
2. Qin GZ, Park JY, Chen SY, Lazarus P. A high prevalence of p53 mutations in premalignant oral erythroplakia. Int J Cancer 1999;80:345–348
3. Mashberg A, Meyers H. Anatomical site and size of 222 early asymptomatic oral squamous cell carcinomas: a continuing prospective study of oral cancer. II. Cancer 1976;37:2149–2157
4. Isenberg JS, Crozier DL, Dailey SH. Institutional and comprehensive review of laryngeal leukoplakia. Ann Otol Rhinol Laryngol 2008;117:74–79
5. Colden D, Zeitels SM, Hillman RE, Jarboe J, Bunting G, Spanou K. Stroboscopic assessment of vocal fold keratosis and glottic cancer. Ann Otol Rhinol Laryngol 2001;110:293–298
6. Bielamowicz S, Kapoor R, Schwartz J, Stager SV. Relationship among glottal area, static supraglottic compression, and laryngeal function studies in unilateral vocal fold paresis and paralysis. J Voice 2004;18:138–145
7. Woo P. Office-based laryngeal procedures. Otolaryngol Clin North Am 2006;39:111–133
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


