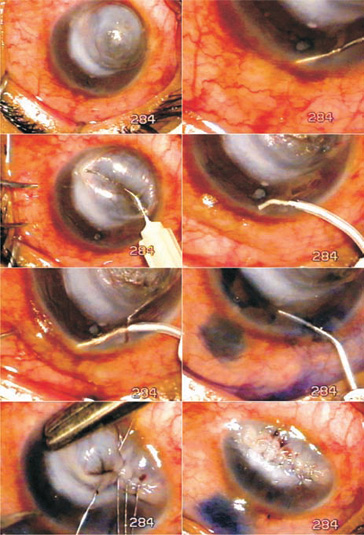
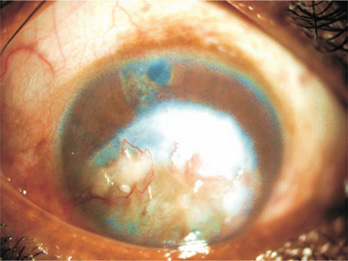
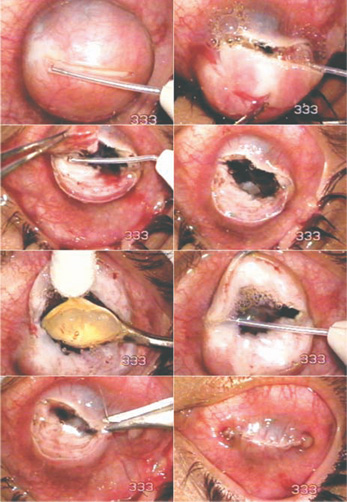
CASE STUDIES The patient was a 30-year-old, very poor man in whom a large anterior staphyloma had developed after corneal ulceration 1 year before. The staphyloma jutted out between the lids and remained exposed day and night, causing great discomfort. Light perception was present and intra-ocular pressure (measured digitally) was very high. Bouts of pain left the patient incapacitated for hours. He and his family were on the verge of starvation because of his inability to work. Many treatments were available to this patient. However, keratoplasty would be costly and beyond the patient’s financial capability. And because donor corneas were unavailable, even free of charge, keratoplasty was out of the question. The patient insisted that I remove his disfigured, painful eye and outfit him with an artificial eye, so that he would be more presentable for hiring. We refused that course of treatment because the eye had light perception. Moreover, an artificial eyeball requires great care to maintain a healthy socket. We found a treatment that would reduce the patient’s high intra-ocular pressure, contain the unsightly staphyloma, and offer a quick recovery so that he could return to work. Surgical Technique There was no anterior chamber and the patient’s intra-ocular pressure was high. As a first step, intra-ocular pressure had to be reduced. Glaucoma surgery was performed by injecting visco-elastic material through a corneal pocket incision to separate the iris from the cornea. Iridectomy was done with the Fugo blade, and ab interno filtration followed. The patient was called back after 1 week for staphylectomy. The surgery was done as described below. Figure 45.1. Subtotal anterior staphyloma (Case 1). Ab interno filtration is done through a corneal pocket incision. The edges of the staphyloma are infolded and joined together with 80-µm stainless steel sutures. Postoperative Management Postoperatively, the patient was very comfortable and extremely satisfied. He returned to work 3 days after surgery. When the patient returned for followup 4 months later, the eye was quiet, there was no staphyloma, the sutures were in place, and his digital intra-ocular pressure appeared normal. He was able to see hand movements through the iridectomy at the 12 o’clock position. The sutures were in place and did not irritate the eye. The sutured tissues appeared to have fused the edges of the staphyloma (Fig. 45.2). Figure 45.2. The appearance of the eye (Case 1) 4 months after surgery. The patient was a 23-year-old farm worker in whom an ocular deformity had developed in one eye after an injury and infection, resulting in loss of vision, 5 years previously. Because he could not close the eye while blinking and sleeping, he was bothered by the constant sensation of having a foreign body in his eye. He requested that I remove the eyeball and replace it with an artificial eye. Examination showed a staphyloma extending from limbus to limbus; it looked like a cannonball. Digital tonometry appeared to be normal. The surgery was done as described below. Surgical Technique Figure 45.3. Total anterior staphyloma (Case 2) is incised, excised, and pared with the Fugo blade. The crystalline lens is removed. The edges of the cut staphyloma are sutured with 80-µm vanadium steel sutures. Figure 45.4. The operated eye (Case 2) 3 months after surgery. The eye is quiet and completely healed. Postoperative Management Two weeks after surgery, one loose irritating steel suture was removed. A thin gap in one area of the incision indicated that the wound was not closed, but a Seidel test was negative. Three months later, the site appeared the same as before and the eye was quiet. Summary The two cases described above demonstrate the utility of the Fugo blade in managing unusual cases in novel ways. These cases also show how minimally traumatic filtration surgery can be integrated with a primary surgical procedure. Suggested Reading Grieser EJ, Tuli SS, Chabi A, et al. Blueberry eye: acquired total anterior staphyloma after a fungal corneal ulcer. Cornea. 2009;28:231–232.
 ungal, bacterial, or mixed corneal infections are common in poor countries. Corneal infections result from neglect of the infectious processes from the start and ineffectiveness of treatment once started. Partial or total anterior staphyloma are common; all that is left is to make the patient comfortable or to do some kind of surgery to improve their appearance. Sometimes an unusual situation calls for an innovative solution. As the following two cases illustrate, the Fugo blade can be included in surgery when tissue ablation or incision is involved.
ungal, bacterial, or mixed corneal infections are common in poor countries. Corneal infections result from neglect of the infectious processes from the start and ineffectiveness of treatment once started. Partial or total anterior staphyloma are common; all that is left is to make the patient comfortable or to do some kind of surgery to improve their appearance. Sometimes an unusual situation calls for an innovative solution. As the following two cases illustrate, the Fugo blade can be included in surgery when tissue ablation or incision is involved.

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


