SECTION I In all fields of medicine, a focused history is an essential starting point in the care of the patient. The order and method in a well-composed vitreoretinal history are similar to those in any medical history (Table 1–1), and the information obtained helps to develop both the diagnosis and the treatment plan. A comprehensive form (Fig. 1–1, pages 2 to 7) can be most useful in helping the physician to collect the necessary data. Simply stated, the chief complaint is usually a single sentence or phrase, from the patient’s perspective, stating the reason for seeking medical attention. It is the patient’s response to the examiner when asked, “Why did you come to the office today?” As an example, in ophthalmology, the most common chief complaint is, “My vision is blurred.” The history of present illness (HPI) is a well-constructed paragraph that includes all the salient details evolving from the chief complaint. This will identify the problem in more detail (Table 1–2).
History, Physical Examination, and Diagnosis
1
Key Questions for a Focused History
What Is the Chief Complaint?
What Is the History of Present Illness?
| Chief complaint |
| History of present illness |
| Past medical/surgical history |
| Medications |
| Allergies |
| Family history |
| Review of systems |
| Social history |
| Which eye or part of the vision is involved? |
| When did the symptom start? How long did it last? Is it progressing? |
| What is the severity? |
| What is the context? What initiated the symptoms? |
| Does anything make it better or worse? |
| Are any other nonocular symptoms present? |
The key questions usually answered in the HPI concern location, timing, duration, severity, context, modifying factors, and associated symptoms. The location in an ophthalmic history identifies which eye is involved and whether both eyes are involved. In addition, if the complaint involves the patient’s vision, the history identifies whether it is the central or the peripheral vision that is affected. The timing and duration explain when the complaint began and whether it is permanent, transient, or progressive. The patient often describes the severity of visual loss in relation to some visual task, such as reading small print (newspaper) or recognizing faces. Modifying factors describe alleviating or aggravating associations that affect the complaint, for example, positional changes or time of day. Associated symptoms are those noted to occur with the ocular problem, such as the onset of headache following ocular migraines or nausea associated with papilledema. The patient always should be questioned about the nonsymptomatic eye to elicit any subtle or vague changes that might be important to the underlying condition.
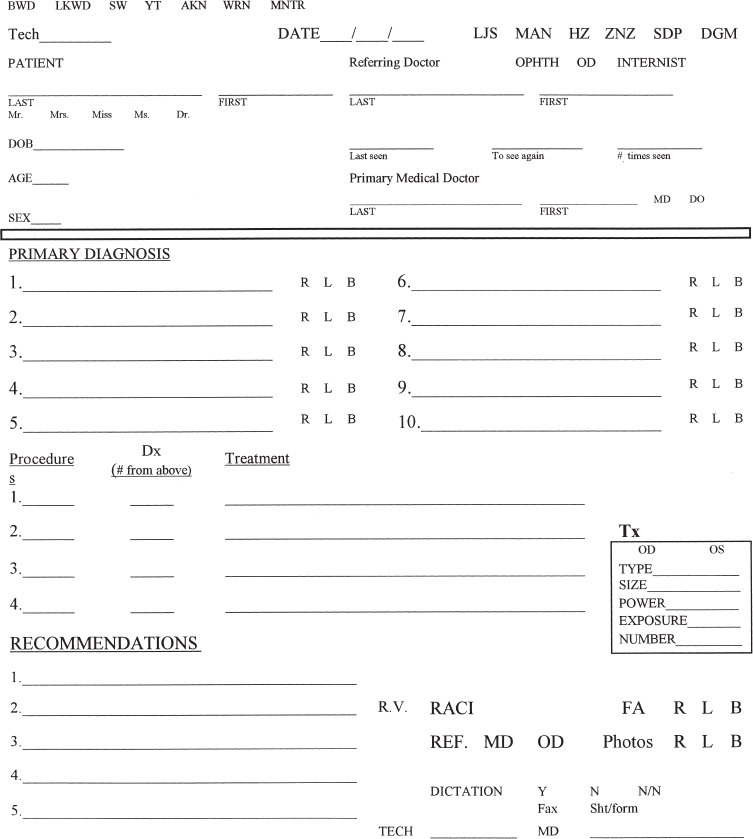
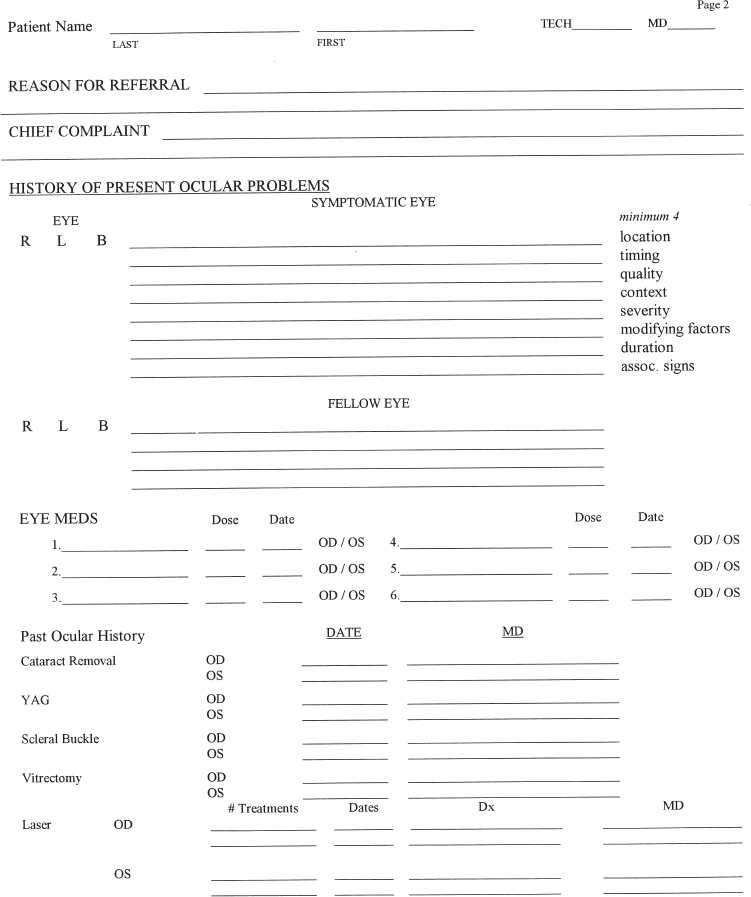
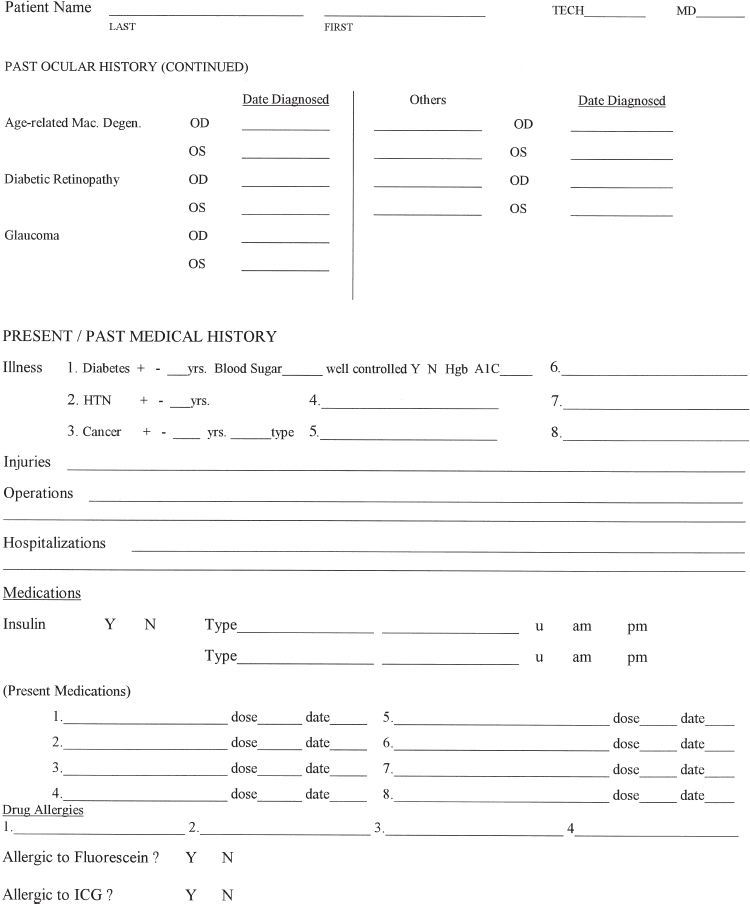
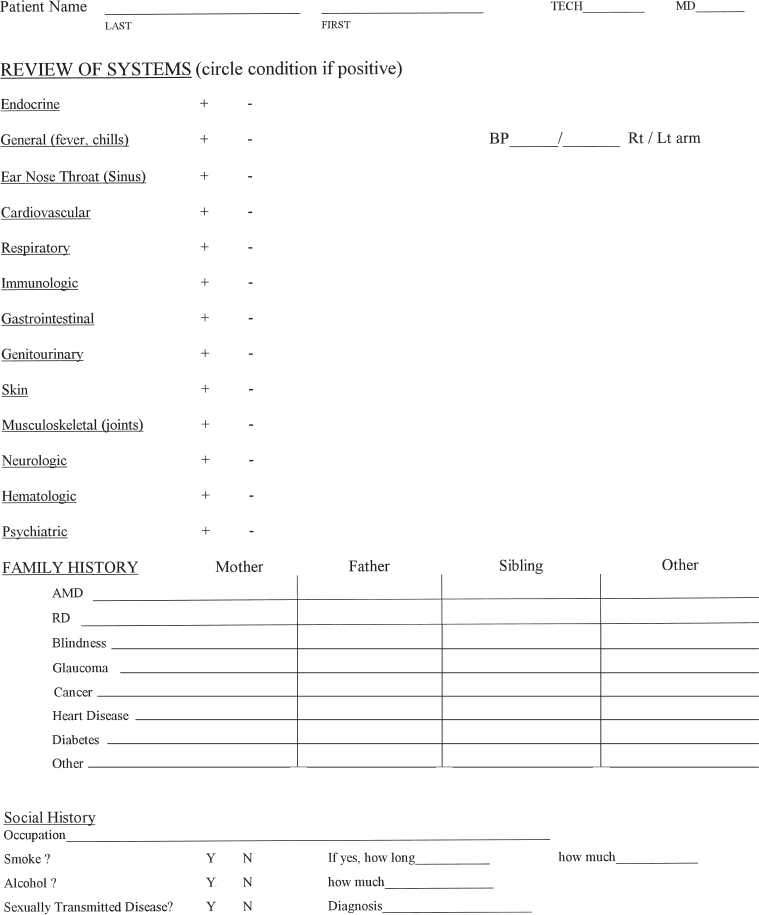
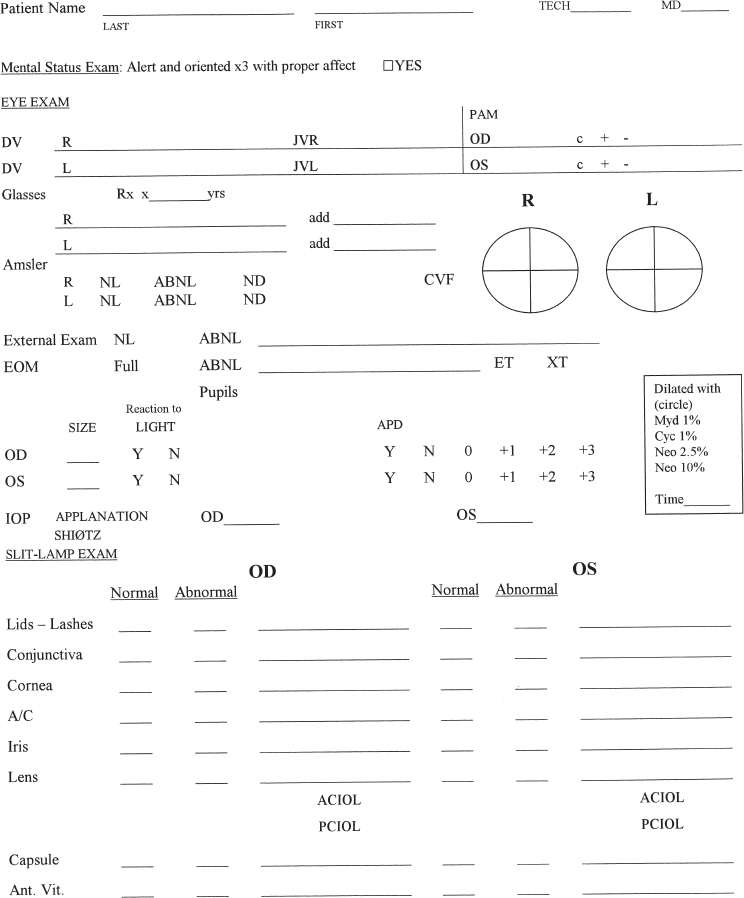
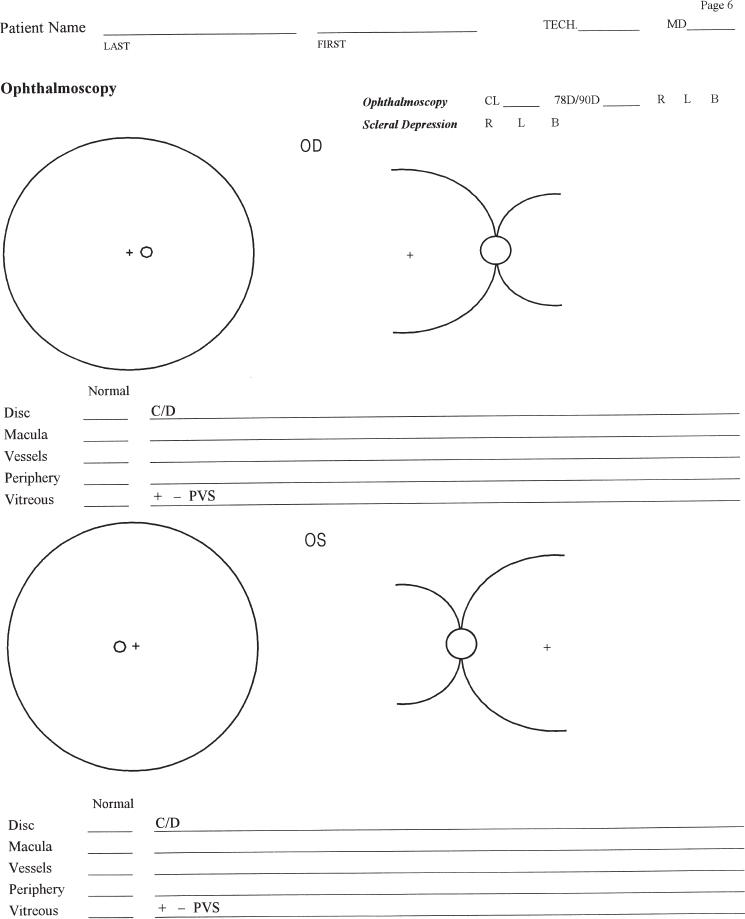
FIGURE 1–1. Initial evaluation and management documentation form.
| Natural refractive state |
| Ocular trauma |
| Ocular laser procedures |
| Ocular surgeries |
| Glaucoma |
| Macular degeneration |
What Is the Past Ocular History?
The past ocular history should include a complete summary of any previous eye diagnosis or surgery (Table 1–3). This includes the refractive state of the eye and, if it is pseudophakic, the refractive state prior to cataract surgery. In the case of corrected myopia secondary to lens implant surgery or refractive surgery, the prior myopic status can be estimated as low, medium, or high. This estimation is based on the patient’s recollections of how thick his or her glasses were before the surgery or how close he or she had to hold a newspaper to read it clearly without correction. These simple questions often will reveal the “previously” high myope.
The ocular surgery history should include all procedures and specific inquiry about laser surgery; many patients will omit this information because they do not consider it ocular surgery. Any history of ocular trauma is important, including both recent and remote events. Such events include blunt trauma to the eye or head and penetrating trauma with or without a retained foreign body. The history of trauma can be important with regard to management and also to nonmedical issues, such as insurance and litigation.
Previous ocular diagnoses should be listed, including noting which eye was involved. In particular, those diagnoses common to the particular demographic involved should be sought. Examples include macular degeneration in the older white patients and glaucoma in African Americans. Inquiring about any eye medications or eyedrops often reveals an underlying diagnosis that was previously overlooked (e.g., topical aqueous suppressants, artificial tears).
What Is the Past Medical History?
Systemic conditions often influence the development of vitreoretinal disease and can affect their management. A list should be compiled of previous medical diagnoses, surgical procedures, hospitalizations, medications, and allergies (Table 1–4). A patient may forget to mention a particular medical diagnosis that can be inferred from the medications taken or previous surgery performed. An example is the patient who fails to note a history of cardiovascular disease but lists using nitroglycerin or having undergone previous heart surgery.
| Previous medical diagnoses or illnesses |
| Hospitalizations |
| Surgeries |
| Injuries |
| Medications (including over-the-counter) |
| Drug allergies |
What Systemic Diseases Are Important in the Diagnosis?
Some medical illnesses, including diabetes mellitus, hypertension, sickle cell anemia, leukemia, and sepsis, have a direct link to vitreoretinal disorders. Among these, diabetes and hypertension are prevalent as well as causative or contributory to many retinal disorders. In fact, diabetes mellitus is the most common systemic condition that causes blindness. In patients with diabetes, the duration of the disease significantly influences the severity of the retinopathy. Also, as shown in the Diabetes Control and Complications Trial, the more well controlled the blood sugar, the lower the incidence of severe retinopathy.1 Therefore, asking the patient about the duration of the disease (years), the usual range of blood sugars, or even the hemoglobin A1c can provide clues to diagnosis and treatment. In addition, associated diabetic complications, such as nephropathy, neuropathy, and peripheral vascular disease, can provide guidance as to likely ocular involvement from diabetes mellitus.2
What Systemic Factors Are Important in Determining Treatment and Anesthesia?
Other systemic conditions are important when considering the treatment plan, especially if surgery is required. Medications to which the patient is allergic are to be avoided, although often a more detailed allergy history will determine that the supposed allergy was more likely a medication side effect or a coincidental happening at the time the medication was used. An example is nausea with intravenous fluorescein injection, which is a side effect, not an allergic reaction. Particular allergies that should be noted include those to fluorescein and indocyanine green (ICG), two dyes commonly used in the diagnosis of retinal disorders. ICG allergic reactions are more likely in people who have shellfish or iodine allergies, and the physician must use clinical judgment in deciding whether ICG angiography should be done in these cases.
Some medical conditions can be exacerbated by systemic absorption of topical eye medications. In particular, the beta-blocking aqueous suppressants can have harmful effects on heart rate and blood pressure as well as on the patient’s mood. Even the more common eyedrops, such as atropine, which can cause altered mental status, and phenylephrine, which can raise blood pressure, should be used judiciously in patients who already have these diagnoses. A common method used to avoid these complications of treatment is punctal occlusion, which requires digital pressure at the medial canthal area for several minutes after instillation of the eyedrop. If a patient at risk of complications from systemic absorption of eyedrops is unable to perform punctal occlusion, the choice of topical agents may have to be modified or at least the signs of systemic toxicity closely monitored by patient, family, and physician.
What Is a Review of Systems?
A review of systems is a systematic search for other illnesses through questioning the patient about symptoms unrelated to the chief complaint (Table 1–5). A full medical review of systems can be helpful in patients with undiagnosed systemic conditions that are linked to vitreoretinal disease or with systemic conditions that can affect treatment plans (Table 1–5). One common example is the undiagnosed diabetic patient, who may be having nocturia or paresthesias (Table 1–5). The review of systems may lead the physician to suspect a previously undiagnosed medical condition that affects the risks associated with treatment. For example, shortness of breath or occasional chest pains might indicate possible heart disease. It certainly would be advantageous to know about this condition before undertaking surgery.
| General: fever, chills |
| Endocrine: weight loss or gain, lethargy, polydipsia |
| Ear, nose, throat: hoarseness, tinnitus, nasal congestion |
| Cardiovascular: chest pressure, shortness of breath, orthopnea |
| Respiratory: shortness of breath, cough, mucus production |
| Immunologic: recurrent infections, high-risk HIV behavior |
| Gastrointestinal: nausea, diarrhea, heartburn |
| Genitourinary: nocturia, hematuria, frequency |
| Dermatologic: changing moles or skin lesions |
| Musculoskeletal: stiffness of joints, swelling, weakness |
| Neurologic: paresthesias, weakness |
| Psychiatric: depression, anxiety |
A more specific ocular review of symptoms can be helpful in diagnosing complex or multiple ocular conditions and in planning treatment. A simple way to classify this type of review is by ophthalmic subspecialty: anterior segment, glaucoma, neuroophthalmology, oculoplastics, strabismus, and posterior segment. An example would be the patient with macular degeneration who also has intermittent diplopia or ptosis secondary to undiagnosed myasthenia gravis.
What Is a Relevant Family History?
A relevant family history is used to uncover vitreoretinal diseases in some fully or partially inherited ocular conditions (Table 1–6). An efficient method of identifying severe inherited ocular conditions is to ask whether any extended family members have lost vision, especially at a younger age. Typically, this will reveal families with macular dystrophies, retinal detachments, retinoblastoma, and other such conditions. It is sometimes helpful to examine some of the family members as part of a more thorough family history.
| Blindness at young or middle age |
| Retinal detachment |
| Macular degeneration |
| Glaucoma |
| Ocular cancer |
| Diabetes |
What is a Relevant Social History?
A relevant social history includes the patient’s occupation, living arrangements, smoking, and alcohol use. Occupational concerns revolve around whether the patient will be able to continue in that line of work. Many vitreoretinal diseases are extremely disabling and can involve both eyes eventually. The patients need to be aware of a realistic prognosis and to be able to make plans regarding time off from work, short-term disability, or long-term disability.
Postoperative living arrangements are more important than ever because vitreoretinal surgery has evolved into an outpatient surgical specialty. Frail patients or those with poor vision in the postoperative period will need assistance with eyedrops, systemic medications, and possibly activities of daily living. These needs may be short-term or long-term, depending on the prognosis. Also, if a patient needs to travel or fly shortly after surgery, the surgical plan may have to avoid the use of intraocular gases.
Summary
A well-constructed history often points the physician in the right direction for diagnosis and treatment. In addition, it can help the astute surgeon lower the risk of some complications and lead to a more satisfactory outcome.
REFERENCES
- The Diabetes Control and Complications Trial Research Group. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med. 1993;329:977–986.
- Miller DG, Singerman LJ. Diabetic retinopathy: medical considerations. In: Saer JB, ed. Vitreo-Retinal and Uveitis Update. Proceedings of the New Orleans Academy of Ophthalmology Symposium. The Hague: Kugler Publications; 1998:239–244.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


